
References
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405
- Huisman MV, Barco S, Cannegieter SC, et al. Pulmonary embolism. Nat Rev Dis Primers. 2018;4:18028. doi:10.1038/nrdp.2018.28
- Koch E, Lovett S, Nghiem T, Riggs RA, Rech MA. Shock index in the emergency department: utility and limitations. Open Access Emerg Med. 2019;11:179-199. doi:10.2147/oaem.s178358
- Gökçek K, Gökçek A, Demir A, Yıldırım B, Acar E, Alataş OD. In-hospital mortality of acute pulmonary embolism: predictive value of shock index, modified shock index, and age shock index scores. Med Clin (Barc). 2022;158(8):351-355. doi:10.1016/j.medcli.2021.04.035
- Spampinato MD, Covino M, Passaro A, et al. Predicting in-hospital mortality in pulmonary embolism patients: development and external validation of the PATHOS score. Clin Exp Emerg Med. 2023;10(1):26-36.
- Çağlar A, Akıllı NB, Köylü R, Alpaydın MS. Jugular vein diameter: a new player in normotensive pulmonary embolism. Clin Imaging. 2021;74:4-9. doi:10.1016/j.clinimag.2020.12.034
- Toosi MS, Merlino JD, Leeper KV. Prognostic value of the shock index along with transthoracic echocardiography in risk stratification of patients with acute pulmonary embolism. Am J Cardiol. 2008;101(5):700-705. doi:10.1016/j.amjcard.2007.10.038
- Keller K, Coldewey M, Geyer M, Beule J, Balzer JO, Dippold W. Shock index for outcome and risk stratification in acute pulmonary embolism. Artery Res. 2016;15:30-35. doi:10.1016/j.artres.2016.05.002
- Otero R, Trujillo-Santos J, Cayuela A, et al. Hemodynamically unstable pulmonary embolism in the RIETE Registry: systolic blood pressure or shock index? Eur Respir J. 2007;30(6):1111-1116. doi:10.1183/09031936.00071007
- Kara H, Degirmenci S, Bayir A, Ak A. Pulmonary embolism severity index, age-based markers and evaluation in the emergency department. Acta Clin Belg. 2015;70(4):259-264.
- Zhou J, Shan PR, Xie QL, et al. Age shock index and age-modified shock index are strong predictors of outcomes in ST-segment elevation myocardial infarction patients undergoing emergency percutaneous coronary intervention. Coron Artery Dis. 2019;30(6):398-405. doi:10.1097/mca.0000000000000759
- Bondariyan N, Vakhshoori M, Sadeghpour N, Shafie D. Prognostic value of shock index, modified shock index, and age-adjusted derivatives in prediction of in-hospital mortality in patients with acute decompensated heart failure: Persian Registry of Cardiovascular Disease/Heart Failure Study. Anatol J Cardiol. 2022;26(3):210-217. doi:10.5152/anatoljcardiol.2021.671
- Dalmau R. The diastolic shock index works…but what is it? Ann Intensive Care. 2020;10:103. doi:10.1186/s13613-020-00720-5
- Ospina-Tascón GA, García-Gallardo G, Orozco N. Using the diastolic shock index to determine when to promptly administer vasopressors in patients with septic shock. Clin Exp Emerg Med. 2022;9(4):367-369. doi:10.15441/ceem.22.401
- Kim DS, Park JE, Hwang SY, et al. Prediction of vasopressor requirement among hypotensive patients with suspected infection: usefulness of diastolic shock index and lactate. Clin Exp Emerg Med. 2022;9(3):176-186. doi:10.15441/ceem.22.324
- Avci M, Doganay F. Prognostic performance of shock index, diastolic shock index, age shock index, and modified shock index in COVID-19 pneumonia. Disaster Med Public Health Prep. 2022;17:e189.
- Lai WH, Wu SC, Rau CS, Kuo PJ, Hsu SY, Chen YC. Systolic blood pressure lower than heart rate upon arrival at and departure from the emergency department indicates a poor outcome for adult trauma patients. Int J Environ Res Public Health. 2016;13(6):528. doi:10.3390/ijerph13060528
Figures
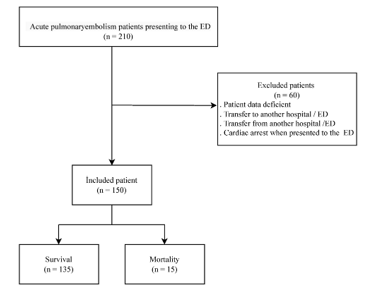
Figure 1. Flowchart of this research
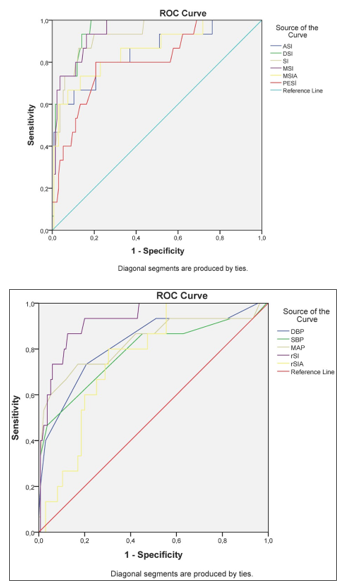
Figure 2. AUC value of shock indices in predicting the mortality of pumonary embolism patients. a; ROC curve of ASI, DSI, SI, MSI, MSIA, PESI. b; ROC curve of DBP, SBP, MAP, rSI, rSIA
Tables
Table 1. Clinical characteristics of pulmonary embolism patients
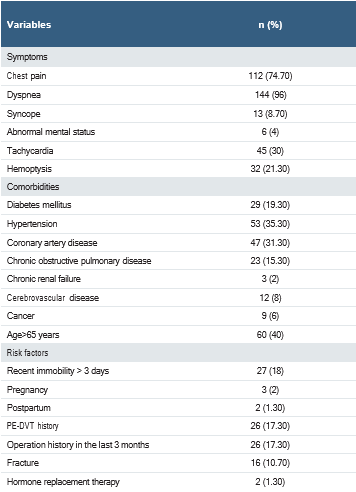
Abbreviations: PE, pulmonary embolism; DVT, deep-vein thrombosis.
Table 2. Distribution of shock indices according to mortality
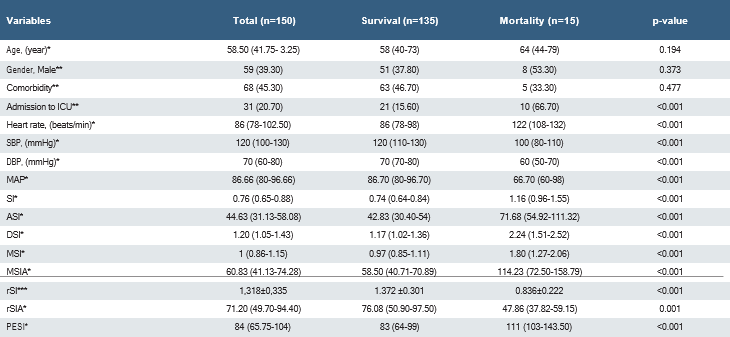
Abbreviations: ICU: intensive care unit; DBP, diastolic blood pressure; SBP, systolic blood pressure; MAP, mean arterial pressure; SI, shock index; DSI, diastolic shock index; MSI, modified shock index; ASI, age shock index; rSI, reverse shock index; MSIA, MSI multiplied by age; rSIA, rSI multiplied by age; PESI, pulmonary embolism severity index. *: median (interquartile range); : n (%);*: mean ± standard deviation.
Table 3. Optimal cut-point values in predicting hospital mortality for shock indices in pulmonary embolism patients
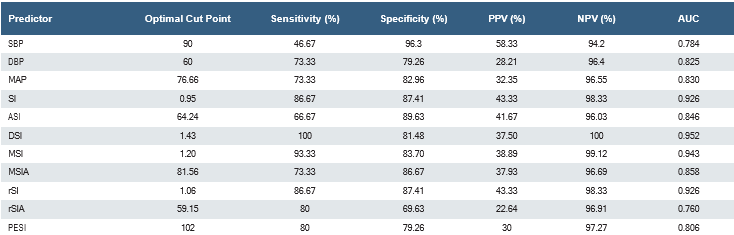
Abbreviations: PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve.
About This Article
How to Cite This Article
Mustafa İçer, Veysi Tekin. The effectiveness of shock indices in predicting mortality in acute pulmonary embolism. doi:10.4328/ACAM.22519
Publication History
- Received:
- 10.12.2024
- Accepted:
- 23.01.2025
- Published Online:
- 20.03.2025
- Printed:
- 01.11.2025