
Prognostic value of the lymphocyte-to-monocyte ratio in predicting axillary lymph node metastasis in breast cancer
Breast cancer
Authors
Abstract
AimAxillary lymph node metastasis is one of the most important parameters in determining the prognosis and therapeutic approach in patients with malignant breast disease. In recent years, systemic inflammatory markers have been shown to be associated with tumor biology and metastatic potential. The objective of this study was to investigate the relationship between the lymphocyte-to-monocyte ratio and axillary lymph node metastasis.
MethodsA total of 140 patients who underwent surgery for malignant breast disease between 2021 and 2024 were retrospectively evaluated. Demographic data, type of surgical procedure, number of excised lymph nodes, presence of metastatic lymph nodes, and hematological parameters were reviewed. The lymphocyte-to-monocyte ratio was calculated by dividing the absolute lymphocyte count by the absolute monocyte count obtained from the preoperative complete blood count. Patients were categorized into two groups according to the presence or absence of axillary lymph node metastasis, and the lymphocyte-to-monocyte ratio values were compared between the groups.
ResultsAxillary lymph node metastasis was detected in 62 patients (44.3%). The mean lymphocyte-to-monocyte ratio was 3.99 in the metastasis-positive group and 5.01 in the metastasis-negative group. Although the mean lymphocyte-to-monocyte ratio was lower in patients with nodal metastasis, this difference did not reach statistical significance according to the Mann–Whitney U test.
ConclusionIn breast cancer patients, those with axillary lymph node metastasis tended to have lower lymphocyte-to-monocyte ratio values. However, this difference was not statistically significant. Larger cohorts and prospective studies are warranted to clarify the potential role of the lymphocyte-to-monocyte ratio as a predictor of axillary nodal involvement.
Keywords
Introduction
Breast cancer is the most common malignancy among women worldwide and remains a leading cause of morbidity and mortality.1 Despite significant advances in early diagnosis and treatment modalities, axillary lymph node metastasis continues to be one of the most critical determinants of disease prognosis.2 Axillary lymph node involvement not only reflects the biological behavior and systemic dissemination potential of the tumor but also directly influences surgical strategies and adjuvant treatment decisions.3 In recent years, it has become evident that not only histopathological findings but also systemic inflammatory response markers carry prognostic significance in understanding tumor biology. Peripheral hematological parameters such as the neutrophil-to- lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) have gained attention due to their easy accessibility and low cost, making them promising tools for integration into clinical practice.4 For instance, meta-analyses across various tumor types have demonstrated that elevated NLR and PLR are associated with poorer survival outcomes, whereas higher LMR is correlated with a more favorable prognosis.5 These parameters are believed to be linked to the tumor microenvironment, reflecting the systemic immune response, and are increasingly emphasized in the literature as potential prognostic biomarkers.6 Particularly, the LMR has emerged as a notable biomarker, as it simultaneously reflects both the host immune response and systemic inflammation. Systematic reviews and meta-analyses have demonstrated that elevated LMR is significantly associated with better overall survival, progression-free survival, and cancer-specific survival in metastatic colorectal cancer7 and is an independent prognostic predictor in rectal cancer.8 In additional contexts, such as glioma and gastric cancer treated with immune checkpoint inhibitors, LMR has shown superior prognostic relevance compared to NLR and PLR.9,10 In the literature, hematological inflammatory markers such as the NLR, PLR, and LMR have been shown to carry prognostic significance across a wide range of solid tumors. However, studies specifically investigating the association between LMR and axillary lymph node metastasis in breast cancer remain limited. For instance, in a large-scale study conducted by Jia et al., high LMR was found to have only a weak association with recurrence-free survival in triple-negative breast cancer patients, whereas NLR demonstrated independent prognostic value.11 Conversely, another study reported that patients with higher LMR following neoadjuvant chemotherapy exhibited more favorable prognostic outcomes, with LMR showing strong diagnostic performance.12 Addressing this gap in the literature, the primary objective of the present study was to retrospectively evaluate the relationship between preoperative LMR and axillary lymph node metastasis in patients who underwent surgery for malignant breast disease between 2021 and 2024.
Materials and Methods
Study Design and Patient SelectionThis retrospective study was conducted on patients who underwent surgery for malignant breast disease at the Malatya Training and Research Hospital, Department of General Surgery, between January 2021 and December 2024. A total of 140 patients were included. Patients were excluded if preoperative hematological parameters were unavailable, or if they had active infection, autoimmune disease, a history of hematologic malignancy, or were receiving systemic corticosteroid or immunosuppressive therapy at the time of evaluation.
Clinical and Pathological DataPatient age, sex, histopathological diagnosis, type of surgical procedure, total number of excised lymph nodes, and presence of axillary metastatic lymph nodes were obtained from medical records and pathology reports.
Hematological Parameters and Calculation of LMRRoutine preoperative complete blood counts obtained within two weeks prior to surgery were reviewed for all patients. Absolute lymphocyte and monocyte counts were recorded, and the LMR was calculated using the following formula:
LMR = Lymphocyte Count/Monocyte Count
GroupingPatients were divided into two groups based on pathological evaluation: those with axillary lymph node metastasis (Metastasis [+]) and those without metastasis (Metastasis [–]). LMR values were compared between the groups.
Ethical ApprovalThis study was approved by the Ethics Committee of Malatya Turgut Özal University (Date: 2025-08-04, No: E-30785963-020-322362).Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). The Shapiro–Wilk test was used to assess the assumption of normality. Since LMR values did not follow a normal distribution, comparisons between groups were performed using the Mann–Whitney U test. Categorical variables were analyzed with the Chi-square test or Fisher’s exact test, as appropriate. A p<0.05 was considered statistically significant.
Ethical ApprovalThis study was approved by the Ethics Committee of Malatya Turgut Özal University (Date: 04.08.2025, Decision No: E-30785963-020-322362).
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
A total of 140 patients were included in the study, with a mean age of 58.3 ± 11.2 years. All patients were female. Histopathological evaluation revealed invasive ductal carcinoma as the most common tumor type (74.2%), followed by invasive lobular carcinoma (12.1%). Axillary lymph node metastasis was detected in 62 patients (44.3%), whereas 78 patients (55.7%) had no metastasis. The total number of resected lymph nodes did not differ significantly between patients with and without metastasis (median 14 vs. 13, p=0.338).
Regarding hematological parameters, in the metastasis-positive group, the mean lymphocyte count was 2.14 ± 0.71 × 10⁹/L and the mean monocyte count was 0.56 ± 0.19 ×10⁹/L. In the metastasis-negative group, these values were 2.36 ± 0.68 ×10⁹/L and 0.51 ± 0.17 ×10⁹/L, respectively. Although the differences were not statistically significant, the LMR was lower in patients with axillary metastasis compared to those without metastasis (3.99 ± 2.14 vs. 5.01 ± 2.87). This difference did not reach statistical significance (p=0.092) (Table 1).
The diagnostic performance of LMR in predicting axillary lymph node metastasis was evaluated using receiver operating characteristic (ROC) curve analysis. The analysis yielded an area under the curve (AUC) of 0.58, and no clinically meaningful cut-off value could be determined. Furthermore, logistic regression analysis demonstrated that LMR was not an independent risk factor for axillary metastasis (odds ratio [OR] = 0.91; 95% confidence interval [CI]: 0.80–1.04; p=0.179) (Figure 1).
Discussion
Breast cancer remains one of the most significant health challenges worldwide, not only due to its high incidence but also because axillary lymph node metastasis continues to represent the cornerstone of prognostic assessment and treatment planning.13 In this context, there is growing interest in identifying simple and inexpensive biomarkers that may complement traditional staging systems and help refine prognostic stratification.4
In this study, the relationship between the preoperative LMR and axillary lymph node metastasis in patients with breast cancer was investigated. Our findings demonstrated that LMR values were lower in the metastasis-positive group compared with the metastasis-negative group; however, this difference did not reach statistical significance, which is consistent with previous studies reporting limited independent prognostic value of LMR in breast cancer,14 while NLR has been shown to be a stronger and independent predictor, especially in triple- negative breast cancer.15 ROC curve analysis showed poor discriminatory power (AUC = 0.58), and logistic regression analysis revealed that LMR was not an independent predictor of axillary metastasis. These results suggest that LMR alone may not be a strong marker for predicting axillary involvement. The biological rationale for LMR lies in its ability to reflect the balance between immune response and inflammation. Lymphocytes play a critical role in tumor immune surveillance and suppression, whereas monocytes can differentiate into tumor- associated macrophages within the tumor microenvironment, thereby facilitating angiogenesis, invasion, and metastasis.16 Consequently, lower LMR values may indicate increased metastatic potential. Several studies in different malignancies have demonstrated that decreased LMR is associated with poor survival outcomes and increased metastasis.17 The observation of lower LMR values in our metastasis-positive group is consistent with this biological mechanism; however, statistical significance could not be demonstrated, likely due to sample size limitations and the retrospective design.
Previous studies have reported conflicting results regarding the prognostic role of LMR in breast cancer. Ma et al. demonstrated that low LMR was associated with shorter disease-free survival (DFS) and identified LMR as an independent prognostic factor in patients receiving neoadjuvant chemotherapy.18 Similarly, Goto et al. and Ni et al. reported that higher pre-treatment LMR was associated with improved survival outcomes.19,20 In contrast, Balbaloglu et al. found that inflammatory indices, including LMR, had limited value in predicting sentinel lymph node metastasis in early-stage breast cancer.14 Our results are in line with these latter findings, suggesting that the predictive value of LMR for axillary metastasis remains inconclusive.
From a clinical perspective, LMR is an easily accessible, inexpensive, and noninvasive parameter, which makes it an attractive potential biomarker. Nevertheless, the present study indicates that LMR is insufficient as a stand-alone predictor of axillary metastasis. Therefore, it should not be used in isolation but rather interpreted in conjunction with classical prognostic factors and other hematologic indices such as NLR and PLR.
Limitations
Its retrospective and single-center design introduces potential bias, and the relatively small sample size may have limited the statistical power. Furthermore, given the dynamic nature of inflammatory markers, a single preoperative measurement may not accurately reflect the overall biological status.
Conclusion
In this study, the relationship between axillary lymph node metastasis and the preoperative LMR in patients with breast cancer was investigated. Our findings demonstrated lower LMR values in patients with metastasis; however, this difference did not reach statistical significance. Both ROC curve analysis and logistic regression indicated that LMR alone is not a strong predictor of axillary lymph node metastasis.
Nevertheless, the consistently lower LMR observed in the metastasis-positive group suggests that this parameter may serve as a complementary prognostic indicator. Its accessibility, low cost, and derivation from routine hematological tests render it potentially valuable, particularly in resource-limited settings. However, integration of LMR into clinical practice requires validation through larger, multicenter, and prospectively designed studies.
Declarations
Ethics Declarations
The study protocol was reviewed and approved by the institutional ethics committee, and all procedures were conducted in accordance with relevant ethical standards and the Declaration of Helsinki.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was waived due to the retrospective design of the study.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: B.Ö.
Methodology: B.Ö., O.G.G.
Formal Analysis: O.G.G.
Investigation: B.Ö., O.G.G.
Data Curation: O.G.G.
Writing – Original Draft Preparation: B.Ö.
Writing – Review & Editing: B.Ö., O.G.G.
Supervision: O.G.G.
Abbreviations
AUC: Area Under the Curve
CI: Confidence Interval
IQR: Interquartile Range
LMR: Lymphocyte-to-Monocyte Ratio
NLR: Neutrophil-to-Lymphocyte Ratio
OR: Odds Ratio
PLR: Platelet-to-Lymphocyte Ratio
ROC: Receiver Operating Characteristic
SD: Standard Deviation
References
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
-
Wu T, Long Q, Zeng L, et al. Axillary lymph node metastasis in breast cancer: from historical axillary surgery to updated advances in the preoperative diagnosis and axillary management. BMC Surg. 2025;25(1):81. doi:10.1186/s12893-025-02802-2
-
Park KU, Somerfield MR, Anne N, et al. Sentinel lymph node biopsy in early-stage breast cancer: ASCO guideline update. J Clin Oncol. 2025;43(14):1720-1741. doi:10.1200/jco-25-00099
-
Xie J, Guo Z, Zhu Y, Ma M, Jia G. Peripheral blood inflammatory indexes in breast cancer: a review. Medicine (Baltimore). 2023;102(48):e36315.
-
Liu Y, He M, Wang C, Zhang X, Cai S. Prognostic value of neutrophil-to-lymphocyte ratio for patients with triple-negative breast cancer: a meta-analysis. Medicine (Baltimore). 2022;101(28):e29887.
-
Gu L, Li H, Chen L, et al. Prognostic role of lymphocyte-to-monocyte ratio for patients with cancer: evidence from a systematic review and meta-analysis. Oncotarget. 2016;7(22):31926-31942. doi:10.18632/oncotarget.7876
-
Naszai M, Kurjan A, Maughan TS. The prognostic utility of pre-treatment neutrophil-to-lymphocyte ratio (NLR) in colorectal cancer: a systematic review and meta-analysis. Cancer Med. 2021;10(17):5983-5997.
-
Portale G, Bartolotta P, Azzolina D, Gregori D, Fiscon V. Prognostic role of platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio in operated rectal cancer patients: systematic review and meta-analysis. Langenbecks Arch Surg. 2023;408(1):85-92.
-
Wang Y, Xu C, Zhang Z. Prognostic value of pretreatment lymphocyte-to-monocyte ratio in patients with glioma: a meta-analysis. BMC Med. 2023;21(1):486. doi:10.1186/s12916-023-03199-6
-
Su J, Li Y, Tan S, Cheng T, Luo Y, Zhang L. Pretreatment neutrophil-to-lymphocyte ratio is associated with immunotherapy efficacy in patients with advanced cancer: a systematic review and meta-analysis. Sci Rep. 2025;15(1):446.
-
Jia W, Wu J, Jia H, et al. The peripheral blood neutrophil-to-lymphocyte ratio is superior to the lymphocyte-to-monocyte ratio for predicting the long-term survival of triple-negative breast cancer patients. PLoS One. 2015;10(11):e0143061.
-
Chen XY, Long ZQ, Huang HY, et al. Predicting survival of patients with nonmetastatic breast cancer based on fibrinogen-to-albumin ratio and lymphocyte-to-monocyte ratio: a nomogram-based assessment. Breast Care (Basel). 2023;18(5):374-389. doi:10.1159/000531939
-
Huang Z, Mo S, Li G, et al. Prognosticating axillary lymph node metastasis in breast cancer through integrated photoacoustic imaging, ultrasound, and clinical parameters. Breast Cancer Res. 2025;27(1):123.
-
Balbaloglu H, Tasdoven I, Karadeniz Cakmak G. Can inflammatory indices predict sentinel lymph node status in patients with early-stage breast cancer? Medicine (Baltimore). 2023;102(33):e34808.
-
Zhang H, Li Y, Liu YW, Liu YG, Chen X. Predictive value of lymphocyte subsets and lymphocyte-to-monocyte ratio in assessing the efficacy of neoadjuvant therapy in breast cancer. Sci Rep. 2024;14(1):12799.
-
Mantovani A, Sica A, Allavena P, Garlanda C, Locati M. Tumor-associated macrophages and the related myeloid-derived suppressor cells as a paradigm of the diversity of macrophage activation. Hum Immunol. 2009;70(5):325-330. doi:10.1016/j.humimm.2009.02.008
-
Watanabe S, Shimoi T, Nishikawa T, et al. Lymphocyte-to-monocyte ratio as a prognostic and potential tumor microenvironment indicator in advanced soft tissue sarcoma treated with first-line doxorubicin therapy. Sci Rep. 2023;13(1):10734. doi:10.1038/s41598-023-37616-w
-
Zhang T, Lu X. Preoperative inflammatory status as a positive prognostic factor for triple-negative breast cancer patients receiving neoadjuvant therapy. Medicine (Baltimore). 2025;104(28):e42208.
-
Goto W, Kashiwagi S, Asano Y, et al. Predictive value of lymphocyte-to-monocyte ratio in the preoperative setting for progression of patients with breast cancer. BMC Cancer. 2018;18(1):1137. doi:10.1186/s12885-018-5051-9
-
Ni XJ, Zhang XL, Ou-Yang QW, et al. An elevated peripheral blood lymphocyte-to-monocyte ratio predicts favorable response and prognosis in locally advanced breast cancer following neoadjuvant chemotherapy. PLoS One. 2014;9(11):e111886.
Figures
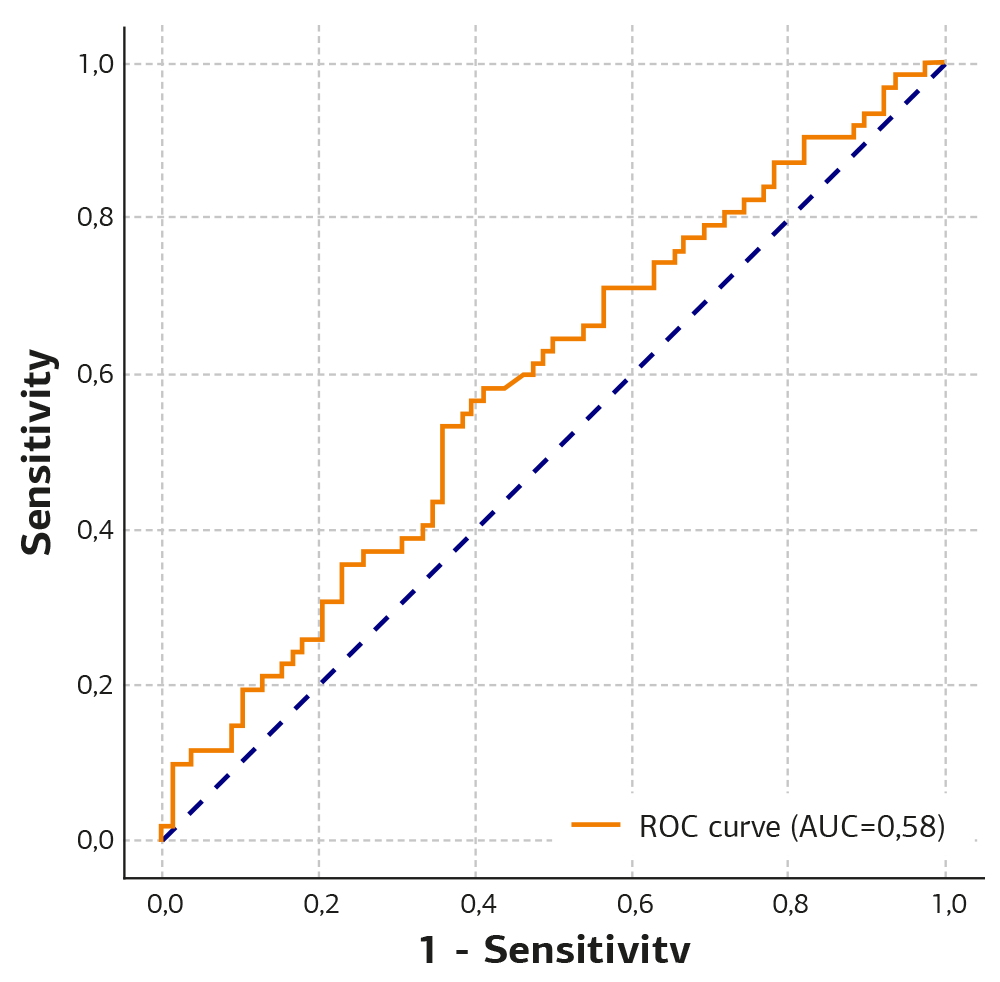
Figure 1. ROC curve analysis of LMR in predicting axillary lymph node metastasis
Tables
Table 1. Comparison of clinicopathological and hematological parameters according to axillary lymph node metastasis status

Abbreviations: LN, lymph node; LMR, lymphocyte-to-monocyte ratio; SD, standard deviation; IQR, interquartile range. *Student’s t-test; † Mann–Whitney U test.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Bahadır Öndeş, Osman Gökhan Gökdere. Prognostic value of the lymphocyte-to-monocyte ratio in predicting axillary lymph node metastasis in breast cancer. Ann Clin Anal Med 2026;17(5):468-471. doi:10.4328/ACAM.22872
- Received:
- August 30, 2025
- Accepted:
- October 6, 2025
- Published Online:
- October 14, 2025
- Printed:
- May 1, 2026