
Short term ocular effects of dialysis type and the contribution of metabolic parameters
Short-term ocular effects of dialysis type
Authors
Abstract
AimAlthough various mechanisms have been proposed to explain the effects of dialysis on ocular parameters, no consensus has been reached. This study aimed to evaluate changes in intraocular pressure (IOP), central corneal thickness (CCT), anterior chamber depth (ACD), and vitreal cavity length (VCL) before and after hemodialysis (HD) and peritoneal dialysis (PD).
MethodsThis prospective study included 40 HD and 32 continuous ambulatory PD patients. For HD patients, pre-dialysis measurements were taken 30 minutes before dialysis at rest, and post-dialysis measurements were taken 30 minutes after dialysis at rest. For PD patients, pre-dialysis measurements were taken 15 minutes after dialysate drainage at rest, and post-dialysis measurements were recorded 2 hours after dialysate filling at rest.
ResultsA significant decrease in IOP (from 14.8 ± 3.6 mmHg to 14.1 ± 3.4 mmHg, p=0.01) was observed following dialysis treatment, independent of the dialysis type. However, no significant changes were found in CCT, ACD, or VCL. In HD patients, IOP significantly decreased pre- to post-dialysis (p=0.045). However, no significant correlations were identified between IOP changes and parameters such as ultrafiltration volume, Kt/V, albumin, hemoglobin, osmolarity, systolic blood pressure (SBP) and diastolic blood pressure (DBP), urea, or creatinine levels.
Conclusion Regarding the outcomes of this research, the IOP evaluated after dialysis in hemodialysis patients was determined to be statistically significantly decreased, but has not been defined at the depth of the camera anterior bulbi or the length of the vitreal cavity.
Keywords
Introduction
Chronic Kidney Disease (CKD) is a significant public health problem with increasing prevalence in our country and the World, with high morbidity and mortality. CKD is defined as kidney damage lasting 3 months or longer or an estimated glomerular filtration rate (eGFR) of less than 60 ml/min/1.73 m2.1 According to the eGFR level in the Kidney Disease Outcomes Quality Initiative (KDOQI) guide, CKD has five stages. Stage 5 CKD is the end-stage renal failure stage with an eGFR below 15 ml/min/1.73 m2.1 In patients with end-stage renal failure, renal replacement therapies (RRT) may also be required along with medical treatment. Three renal replacement therapies can be applied: hemodialysis, peritoneal dialysis, and renal transplantation.2 CKD is a systemic disease that can affect many organs and systems. These are the central nervous, cardiovascular, hematological, endocrine, gastrointestinal, and musculoskeletal systems. The eye is also one of the organs most affected by chronic kidney damage in patients. Underlying diseases such as diabetes mellitus and hypertension can also affect the eye by causing diseases such as diabetic retinopathy and hypertensive retinopathy.3
Peritoneal dialysis can often be performed as continuous ambulatory peritoneal dialysis (CAPD) or instrumented peritoneal dialysis (APD). CAPD involves multiple daily exchanges (usually three or four) followed by an overnight wait. APD uses a cycling device to perform various overnight exchanges, resulting in short waits.4 Many acute and chronic complications occur during peritoneal dialysis and hemodialysis. Patients are withdrawn from the fluid, the potassium and phosphorus load is reduced, and acidosis is tried to be prevented.5
Although different findings and mechanisms have been suggested in studies investigating the effect of dialysis on ocular parameters in the past, none of them are entirely accepted.6 Within the scope of this research, we aimed to elucidate changes in intraocular pressure (IOP), central corneal thickness (CCT), anterior chamber depth (ACD), and vitreal cavity length (VCL) before and after hemodialysis and peritoneal dialysis treatment and to investigate the differences of these changes between the two types of dialysis (hemodialysis and peritoneal dialysis).
Materials and Methods
This prospective study included 40 hemodialysis and 32 peritoneal dialysis patients over 18 years old, followed at Adana City Training and Research Hospital, who were oriented, cooperative, and undergoing regular dialysis. HD patients received dialysis three times weekly, and PD patients four exchanges daily. Detailed histories and physical exams were recorded, including demographics, comorbidities, and CKD etiologies. Pre and post-dialysis weight and height were measured to calculate body mass index (BMI). Routine labs (urine, creatinine, electrolytes, glucose, blood gas) and ophthalmologic parameters (IOP, CCT, ACD, VCL) were evaluated before and after dialysis.
DialysisIn our study, hemodialysis (HD) patients underwent pre-dialysis measurements 30 minutes before the session at rest, and post- dialysis measurements 30 minutes after the session, also at rest. Peritoneal dialysis (PD) patients were evaluated 15 minutes after draining the dialysate and 2 hours after refilling, both at rest. Systolic and diastolic blood pressure (SBP, DBP) were measured manually, and pulse rates were calculated from radial artery tracings. HD patients were assessed during morning (08:00) and afternoon (12:00) sessions, while PD patients were evaluated before noon (10:30) and in the afternoon (13:00). HD was administered using NovaHF B-18F capillaries and Fresenius 4008S machines, three times a week for four hours, whereas PD patients used Baxter or Fresenius solutions (2000 ml) with standard exchange sets.
Ocular ExaminationIn our study, pre-dialysis ocular measurements for HD patients were taken 30 minutes before and post-dialysis measurements 30 minutes after the session, both at rest. For PD patients, measurements were performed 15 minutes after draining and 2 hours after refilling the dialysate, also at rest. IOP was measured in a sitting position using the Canon TX-20P (Full Auto Tonometer), and biometry—including CCT, ACD, and Axial Length—was performed with the IOL Master 500. Vitreous cavity length was calculated by subtracting ACD from axial length. All measurements were performed by the same examiner. A total of 72 eyes from 72 patients were evaluated, with the right eye selected via randomization.
Laboratory MeasurementsIn our study, pre-dialysis blood samples were used to measure parameters routinely monitored in follow-up, including PTH, calcium, albumin, total protein, triglycerides, HDL, LDL, TSH, CRP, uric acid, HbA1c (in diabetic patients), ferritin, hemogram, urea, creatinine, sodium, potassium, phosphorus, glucose, pH, and HCO₃, using an automatic chemistry analyzer (Abbott Aeroset, MN, USA) and commercial kits (Abbott). Post-dialysis, urea, creatinine, sodium, potassium, phosphorus, glucose, and blood gas values were re-evaluated. For PD patients, peritoneal Kt/V was calculated by collecting 24-hour dialysate before study inclusion and measuring dialysate and plasma urea levels. Residual renal Kt/V was determined similarly from 24-hour urine. Total Kt was the sum of peritoneal and renal Kt values. V (total body water) was estimated via Watson’s formula, and daily Kt/V was obtained by dividing Kt by V, with weekly Kt/V calculated by multiplying the result by seven.
Ethical ApprovalThis study was approved by The Ethics Committee of Çukurova University (Date: 22.01.2021, Decision No: 72)
Statistical AnalysisPatient data collected within the scope of the study were analyzed with the IBM Statistical Package for the Social Sciences (SPSS) for Windows 26.0 (IBM Corp., Armonk, NY) package program. Frequency and percentage for categorical data and mean and standard deviation for continuous data were given as descriptive values. For comparisons between groups, the “independent samples t test” was used for two groups, and the “chi-square test” was used to compare categorical variables. The results were considered statistically significant when the p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
This prospective research enrolled 40 hemodialysis and 32 continuous ambulatory peritoneal dialysis patients, and the right eyes of the participants (n=72) were evaluated. There was no statistically significant difference between the hemodialysis and peritoneal dialysis groups in terms of age (p=0.692), gender (p=0.316), DM (p=0.304), coronary artery disease (p=0.769), hyperlipidemia prevalence (p=0.869), or alcohol use (p=0.08). Hypertension (HT) (p=0.007) and BMI (p=0.008) values of PD patients were statistically significantly higher than those of HD patients (p<0.05). The etiology of CKD in hemodialysis patients could be elaborated as Type 2 DM in 7 patients (17.5%), HT in 19 (47.5%), Obstructive Nephropathy in 6 (15%), Autosomal Dominant Polycystic Kidney Disease (ADPKD) in 4 (10%), Wegener Granulomatosis in 1 (2.5%), drug-related Toxic Nephropathy in 2 (5%), and Systemic Lupus Erythematosus (SLE) in 1 patient (2.5%). The etiology of CKD in hemodialysis patients was Type 2 DM in 7 patients (21.9%), HT in 23 (71.9%), Wegener Granulomatosis in 1 (3.1%), and Type 1 DM in 1 patient (3.1%).
When comparing the metabolic parameters of HD and PD patients, albumin, total protein, triglyceride, uric acid, ferritin, and ultrafiltration volume were significantly higher in the HD group, whereas HDL, LDL, platelet count, and Kt/V were significantly higher in the PD group. In HD patients, post- dialysis measurements showed significant decreases in urea, creatinine, potassium, phosphorus, and osmolarity, and significant increases in glucose, pH, and HCO₃ levels. In PD patients, only creatinine levels decreased significantly after dialysis. SBP, DBP, and body weight significantly decreased after dialysis in HD patients, while a significant increase in weight was observed in PD patients (Table 1 and Table 2).
Dialysis led to a significant reduction in IOP overall (p=0.01), with a notable decrease specifically in hemodialysis patients (p=0.045). However, no significant changes were observed in CCT, ACD, or VCL in either dialysis group. Additionally, no correlation was found between ultrafiltration volume and IOP change (Table 3).
There was no significant effect of hemoglobin, albumin, and ultrafiltration amount on the pre-dialysis and post-dialysis differences in the IOP of hemodialysis patients (R=0.934, p>0.05). No correlation was achieved between IOP change and hemodialysis patients’ ultrafiltration amount, Kt/V, albumin, and hemoglobin values. There was also no significant correlation between IOP change and osmolarity change, SBP change, DBP change, urea change, or creatinine change in hemodialysis patients.
Discussion
This study hypothesized that dialysis-related changes in IOP, CCT, ACD, and VCL would vary by modality due to differences in fluid and electrolyte shifts. Overall, only IOP significantly decreased post-dialysis. When assessed separately, hemodialysis patients showed a significant IOP reduction, while no ocular changes were observed in peritoneal dialysis patients. Although ultrafiltration volume was significantly higher in HD, no correlation was found between ultrafiltration and IOP change.
In previous literature, the outcomes of hemodialysis on ocular pressure are controversial. A study by Sarr et al. 7 determined that no significant change occurred in the IOPs before and after dialysis. They stated that IOP was maintained thanks to the autoregulation mechanisms in the patients. Saavedra- Fuentes et al. 8 investigated 15 HD or hemodiafiltration (HDF) patients were compared. While there was no change in IOP in hemodialysis patients, a decrease in IOP was detected in hemodiafiltration patients. HDF treatment provides convection and diffusion that allows the extraction of molecules of median weight not removed by conventional HD, allowing better removal of toxins and inflammatory molecules, and also provides improved hemodynamic stability in some patients, which is thought to increase the reduction in IOP with higher ultrafiltration rates.9
In a study conducted by Kilavuzoglu et al.,10 a significant decrease in IOP was detected after dialysis in hemodialysis patients. A positive correlation was detected between IOP, mOsm, and BUN. They reported that the decrease in IOP observed during HD was related to the change in colloid osmotic pressure, osmolarity, and ocular perfusion pressure. IOP was effectively controlled with hemodialysis. Ismayilov et al. 11 investigated the short-term effects of hemodialysis treatment on the eye and found a decrease in IOP after dialysis, as in our study. They found that this decrease was mainly correlated with changes in serum albumin levels and weight. Hence, they associated the reduction of IOP with fluid loss and found a statistically significant increase in the patient’s ACD and axial length. They assumed this might be due to the expansion of the vitreal axis due to the displacement of the fluid towards the vitreous after the decrease in plasma oncotic pressure.12 Our study showed no change in the ACD in HD patients while the IOP decreased. We found that the decrease in IOP was not correlated with BUN, creatinine, SBP and DBP changes, osmolarity changes, and ultrafiltration amount.
During PD, proteins are displaced from the peritoneum to the dialysate according to the concentration gradient. The albumin level of PD patients is often lower than that of HD patients.12 Our study found that the PD group’s albumin and total protein values were significantly lower than those of the HD group. The fact that the albumin value of peritoneal dialysis patients is lower than that of hemodialysis patients suggests that plasma oncotic pressure may be lower in PD patients. This difference’s effect on IOP may be less in PD patients.
Yakut et al. compared ocular blood flow parameters of HD and PD patients before and after dialysis with color Doppler USG. After a single HD session, the patient’s ocular blood flow returned to normal. Still, PD patients showed higher systolic and diastolic ocular blood flow than healthy controls, suggesting HD is more effective than PD in providing normal ocular blood flow.13 We believe that the more significant effect of HD on ocular blood flow supports the finding that intraocular changes in our study were more remarkable in HD patients. The considerable decrease in IOP in HD patients in our study, while no significant change in IOP in PD, may be related to changes in ocular blood flow.
The correlation of the decrease in IOP with parameters such as osmolarity, creatinine, SBP, and DBP values has been evaluated in many studies. Kalaycı et al. 14 showed that the mean IOP decreased from 12.2±3.5 mmHg to 10.8±2.2 mmHg, and this decrease was statistically significant. The mean axial length was found to decrease from 23.1±0.8 mm to 22.9±0.8 mm, and the decrease in axial length was found to be significant with a mean value of 0.26±0.15 mm. The change in HD patients’ DO and DS mean arterial blood pressure was substantial, with a decrease of 11.8±5 mmHg. A significant correlation was found between the change in axial length and the change in IOP. No correlation was found between the CCT change and the IOP change. Serum osmolarity, mean arterial pressure, and body weight were found to have statistically significant decreases, but these decreases were not correlated with IOP. They stated that the increased oncotic pressure caused by ultrafiltration caused a decrease in IOP after dialysis and that the intraocular fluid moved from the eye to the plasma, which decreased the IOP.14 In a study by Afshar et al.,15 IOP in HD patients decreased significantly from 12.32 mmHg to 11.83 mmHg after dialysis. They found no significant relationship between IOP changes before and after hemodialysis, serum sodium and potassium, blood pressure, urea, Kt/V, and weight. Akiyama et al. 16 found a decrease in osmolarity of 12.4 ± 1.4 mOsm/kg after HD.. Changes in IOP and osmolarity were not correlated.17 Previous studies showed no correlation between IOP and systolic pressure, diastolic pressure, and bicarbonate.18 IOP decreases as aqueous humor moves towards serum via the Schlemm canal as fluid is withdrawn from the patient during hemodialysis.
The low IOP level after a hemodialysis session indicates that a careful eye examination should be performed on the same day.19,20 We believe that the eye findings of peritoneal dialysis patients are more stable, and the dialysis session does not affect the eye examination time. In conclusion, eye examination findings after HD and PD differ in studies, and the effects of dialysis type on the eye can be better understood with more patients and repeated measurements.
The strength of our study is that, to our knowledge, it is the first study to investigate ocular findings during continuous ambulatory peritoneal dialysis. It is also the first study to compare ocular findings during a hemodialysis session and continuous ambulatory peritoneal dialysis.
Limitations
The limitations of our study are that ocular measurements were not taken during the hemodialysis session, and there was no control group. Another limitation is that we separately included hemodialysis patients in the study as morning and afternoon sessions instead of taking them simultaneously.
Conclusion
Regarding the outcomes of this research, the IOP evaluated after dialysis in hemodialysis patients was determined to be statistically significantly decreased, but has not been defined at the depth of the camera anterior bulbi or the VCL. In peritoneal dialysis patients, no significant change was determined at IOP, central cornea diameter, camera anterior bulbi depth, or VCL. Additionally, no significant correlation was detected between IOP change and ultrafiltration quantity, Kt/V, Albumin, change of osmolarity, change of SBP and DBP, urine value, and creatinine. While IOP decreased in hemodialysis patients, no change was determined in peritoneal dialysis patients. Central cornea diameter, depth of camera anterior bulbi, and length of vitreal cavity parameters have not changed in both groups.
Declarations
Ethics Declarations
The study protocol was reviewed and approved by the institutional ethics committee, and all procedures complied with the Declaration of Helsinki.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The data are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.A.
Methodology: B.A.A., T.A.
Formal Analysis: T.A.
Investigation: A.A., E.S.
Data Curation: B.A.A.
Writing – Original Draft Preparation: A.A.
Writing – Review & Editing: A.A., T.S.
Supervision: T.S.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing,
and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
ACD: Anterior Chamber Depth
BMI: Body Mass Index
CCT: Central Corneal Thickness
CKD: Chronic Kidney Disease
CRP: C-reactive Protein
DBP: Diastolic Blood Pressure
HD: Hemodialysis
IOP: Intraocular Pressure
Kt/V: Dialysis Adequacy Index
PD: Peritoneal Dialysis
SBP: Systolic Blood Pressure
SPSS: Statistical Package for the Social Sciences
VCL: Vitreous Cavity Length
References
-
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2024;105(4 Suppl):S117-S314.
-
Patel PP, Egodage T. Failing kidneys: renal replacement therapies in the ICU. Trauma Surg Acute Care Open. 2024;9(Suppl 2):e001381.
-
Goodbred AJ, Langan RC. Chronic kidney disease: prevention, diagnosis, and treatment. Am Fam Physician. 2023;108(6):554-561.
-
Zhang Y, Yu C, Li X. Kidney aging and chronic kidney disease. Int J Mol Sci. 2024;25(12):6585.
-
Spasiano A, Benedetti C, Gambaro G, et al. Predictive models in chronic kidney disease: essential tools in clinical practice. Curr Opin Nephrol Hypertens. 2024;33(2):238-246.
-
Levin A, Ahmed SB, Carrero JJ, et al. Executive summary of the KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease: known knowns and known unknowns. Kidney Int. 2024;105(4):684-701.
-
Sarr IL, Sakho B, Guisse EHCD, et al. Effects of hemodialysis on intraocular pressure and ocular perfusion pressure. Cureus. 2024;16(4):e59138.
-
Saavedra-Fuentes N, Pérez-Grovas H, Navarrete R, Lerma C. Intraocular pressure changes during hemodialysis or hemodiafiltration in end-stage renal disease patients. Ther Apher Dial. 2018;22(6):624-629.
-
Roskal-Wałek J, Gołębiewska J, Mackiewicz J, et al. The haemodialysis session effect on the choroidal thickness and retinal and choroidal microcirculation: a literature review. J Clin Med. 2023;12(24):7729.
-
Kilavuzoglu AEB, Yurteri G, Guven N, et al. The effect of hemodialysis on intraocular pressure. Adv Clin Exp Med. 2018;27(1):105-110.
-
Sariyeva Ismayılov A, Aydin Guclu O, Erol HA. Ocular manifestations in hemodialysis patients and short-term changes in ophthalmologic findings. Ther Apher Dial. 2021;25(2):204-210.
-
Cheng L, Hu N, Song D, Chen Y. Mortality of peritoneal dialysis versus hemodialysis in older adults: an updated systematic review and meta-analysis. Gerontology. 2024;70(5):461-478.
-
Yakut ZI, Karadag R, Akcay A, et al. Effect of dialysis type on orbital vascular flow in patients with end-stage renal disease. Ren Fail. 2012;34(6):691-696.
-
Kalayci M, Hassan IA, Keinan IA, et al. The effect of hemodialysis on axial length, ocular surface, and intraocular pressure in patients with end-stage renal failure. Int J Gen Med. 2020;13:1035-1042.
-
Afshar R, Ghasemi H, Shabpiray H, et al. Monitoring of intraocular pressure and its correlation with systemic parameters before and after hemodialysis. Iran J Kidney Dis. 2013;7(1):53-59.
-
Akiyama Y, Matsuoka R, Masuda T, et al. Comparative impact of isolated ultrafiltration and hemodialysis on fluid distribution: a bioimpedance study. Blood Purif. 2022;51(6):492-502.
-
Liakopoulos V, Demirtzi P, Mikropoulos DG, et al. Intraocular pressure changes during hemodialysis. Int Urol Nephrol. 2015;47(10):1685-1690.
-
Jung JW, Yoon MH, Lee SW, Chin HS. Effect of hemodialysis on intraocular pressure, ocular surface, and macular change in patients with chronic renal failure. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):153-162.
-
Samsudin A, Mimiwati Z, Soong T, et al. Effect of haemodialysis on intraocular pressure. Eye (Lond). 2010;24(1):70-73.
-
Lee KM, Park CY, Kim M. A case report of hemodialysis graft-induced increased intraocular pressure. Korean J Ophthalmol. 2021;35(4):328-329.
Tables
Table 1. Metabolic parameters of HD and PD patients

HD: Hemodialysis, PD: Peritoneal Dialysis, SD: Standard deviation, PTH: Parathormone, Ca: Calcium, ALB: Albumin, T Prot: Total protein, Trigl: Triglyceride, HDL: High-density lipoprotein, LDL: Low-density lipoprotein, TSH: Thyroid Stimulating Hormone, CRP: C reactive Protein, AST: Aspartate aminotransferase, ALT: Alanine aminotransferase, GGT: Gamma-glutamyl transferase, ALP: Alkaline phosphatase, LDH: Lactate dehydrogenase, WBC: White blood cell,, HGB: Hemoglobin, HCT: Hematocrit, PLT: Platelet, Kt/V: dialyzer clearance of urea.dialysis time/ volume of distribution of urea, UF: Ultrafiltration
Table 2. Comparison of pre- and post-dialysis laboratory tests and physical examinations of HD and PD patients
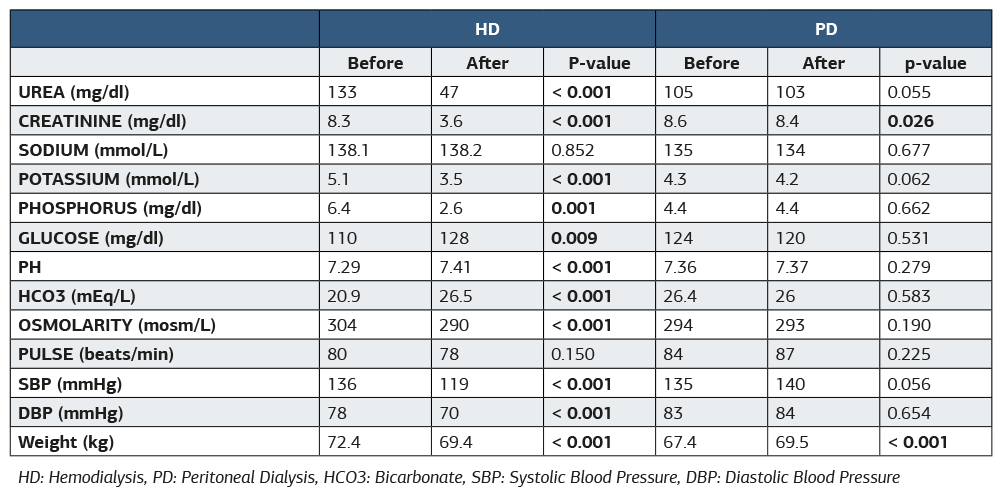
HD: Hemodialysis, PD: Peritoneal Dialysis, HCO3: Bicarbonate, SBP: Systolic Blood Pressure, DBP: Diastolic Blood Pressure
Table 3. Comparison of IOP, CCT, ACD, and VCL before and after renal replacement therapy, hemodialysis, and peritoneal dialysis
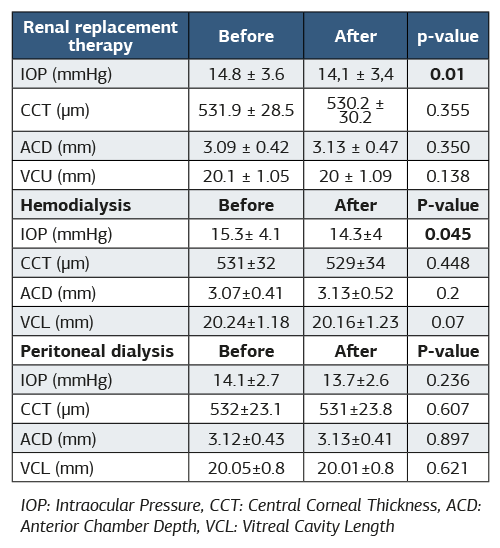
IOP: Intraocular Pressure, CCT: Central Corneal Thickness, ACD: Anterior Chamber Depth, VCL: Vitreal Cavity Length
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ahmet Altıntas, Binhan Aslan Akbulut, Tunahan Ates, Emine Sukgen, Tayyibe Saler. Short term ocular effects of dialysis type and the contribution of metabolic parameters. Ann Clin Anal Med 2026;17(5):00. doi:10.4328/ACAM.22715
- Received:
- April 18, 2025
- Accepted:
- July 21, 2025
- Published Online:
- October 18, 2025
- Printed:
- May 1, 2026