
The role of ERCP in the diagnosis of ampullary tumors in patients with absent mass on radiological findings
Ampullary tumour diagnosis by ERCP
Authors
Abstract
Aim The present study investigates the role of ERCP procedure in diagnosing ampullary tumors in patients who could only be diagnosed with ERCP.
Methods Forty-four patients diagnosed with ampullary tumors were divided into two groups: Group 1 (n = 28) includes the patients with radiological masses, whereas Group 2 (n = 16) comprises those without detectable masses who were diagnosed with ERCP. The results of these two groups were compared in terms of demographic features, tumor size, endoscopic tumor resectability, bilirubin values, and surgical outcomes.
Results A total of forty-four patients were admitted to our centre with the diagnosis of ampullary tumor; five of them were treated with endoscopic ampullectomy, whereas 39 of them were treated with the Whipple procedure. The mean age of the groups was 67.85 ± 13.04 years in group 1 and 62.00 ± 8.43 years in group 2 (p < 0.05). There was no gender difference, but overall, it was observed that ampullary tumors were more common in men than women (26 (59.1%) vs 18 (40.9 %)). The tumor size was bigger in group 1 (2.58 ± 1.30 cm vs 1.21 ± 0.66 cm), and this difference was statistically significant (p < 0.05). The bilirubin values were significantly higher in group 1 as compared to group 2 (6.67 ± 5.34 mg/dl vs 3.09 ± 4.57 mg/dl, p < 0.05). A total of one EA was performed in Group 1 and four patients in Group 2.
Conclusion The present study supports the early use of ERCP to diagnose ampullary tumors in patients with tapering or blunt termination of the bile duct without any mass on radiological images.
Keywords
Introduction
The ampulla of Vater is a convergence point where the bile duct and pancreatic channel converge. It is surrounded by the Oddi sphincter and is located at the descending part of the duodenum, where the mucosal layer covers it 1. Several neoplasms can occur in this region, mainly adenomas and adenocarcinomas. They are rare tumors, accounting for 0.5% of gastrointestinal tumors and 7% of periampullary tumors, and display different clinical and radiological features than other periampullary tumors 2,3. The differential diagnosis between ampullary tumors and other periampullary tumors may sometimes be challenging. The final pathological result and tissue origin may not be possible until the histopathological evaluation of the surgical specimen 4.
There are different methods available for diagnosing ampullary neoplasms, such as ultrasonography (USG), Computed Tomography (CT), Magnetic Resonance Imaging/ Cholangiopancreatography (MRI/MRCP), and Endoscopic Retrograde Cholangiopancreatography (ERCP), depending on the institutional resources. Nodular appearance, erosion, lobular structure, ulceration, and bleeding are endoscopic findings consistent with ampullary cancer. Ampullary cancer differs from other periampullary cancers with an earlier presentation, better survival, and favourable resection rates 2. Since the prognosis is better than other periampullary cancers, early diagnosis is more important. Local endoscopic resection and pancreaticoduodenectomy (Whipple procedure) are recommended treatments for early and invasive cases, respectively. Curative resection can be achieved in about 50% of cases, whereas it is less than 10% for pancreatic cancer 2. Given the rarity of ampullary cancer, strong algorithms for both diagnosis and treatment are lacking. Diagnostic work-up in suspicion of ampullary tumor begins with USG. Although the diagnostic sensitivity of USG is around 90% for pancreatic cancer, it has a limited value for ampullary tumors due to bowel gas and the operator nature of the procedure. However, if there are obvious hepatic metastases, it precludes the further intentions of endoscopic and/or surgical resective treatments 5. CT and MRI are used for the evaluation of distant metastasis, but they have limited value for the detection of primary tumors6. Although MRCP has evolved as a diagnostic method for hepatobiliary and pancreatic pathologies, the small but complex structure of this region limits its accuracy. There may be marked pancreatic duct dilatation and the appearance of a filling defect within the duodenal lumen on MRCP images 4. For patients with suspicious or insufficient CT and MRI imaging findings, there is a strong indication for ERCP. Even if CT and MRI reveal a normal ampullary or periampullary region, ERCP should be persistently considered in case of a suspected ampullary tumor 5. Ideally, as previously reported, EUS and ERCP combined reveal the most accurate information about the ampullary tumor and are unquestionably the most specific endoscopic methods 7,8. However, EUS is not widely available and requires a high level of personal skill and experience 7. The principal benefit of ERCP is that it visualizes the tumor and its characteristics and obtains a biopsy 9. Nowadays, due to the technological development of imaging methods, ERCP is used almost exclusively for therapeutic purposes 8.
The endoscopic features of ampullary tumors are intramural or luminal protrusion, neoplastic appearing ulcerative lesions, irregular borders, and laterally spreading lesions 10. In the case of endoscopic resection, further treatment, if needed, is decided according to the biopsy result and the surgical margins. So, the current study was designed to underline the effect of early use of ERCP to diagnose ampullary tumors in patients with tapering or blunt termination of the bile duct without any mass on radiological images.
Materials and Methods
PatientsThe data of the forty-four patients (26 males and 18 females, with a mean age of 65.45±11.63 years) diagnosed with ampullary tumors between January 2014 to December 2023, were included in this study. Group 1 included patients diagnosed primarily with the presence of an ampullary mass on radiological images (USG, CT, or MRI), and Group 2 included patients with no obvious findings of radiological mass other than indirect radiological findings. These patients were diagnosed primarily with ERCP.
The results of the two groups were compared in terms of demographic features, tumor size, endoscopic tumor resectability, biochemical assays, and surgical outcomes.
The data included relevant demographics, biochemical assays, surgical procedures, tumor size, and final pathological results. The admission symptoms of the patients were jaundice, abdominal pain, weight loss, and cholangitis.
Twenty-six patients (18 males and 8 females with a mean age of 67.85 ± 13.04 years) were diagnosed with the presence of an ampullary mass on radiological images in group 1. The diagnosis was confirmed using ERCP for these patients. Endoscopic ampullectomy was performed in suitable cases; otherwise, the procedure was completed by taking a biopsy.
Eighteen patients (8 males and 10 females with a mean age of 62.00 ± 8.43 years) did not have any obvious findings of radiological mass. These patients had only indirect radiological findings, such as mild to moderate dilatation, tapering, or blunt termination of the bile ducts, and they were included in group 2. Diagnostic ERCP was performed for these patients, and in the case of tumor detection, endoscopic ampullectomy or tissue biopsy was performed depending on the appearance of the tumor.
In patients who had undergone endoscopic ampullectomy, biopsies were taken from the tumor bed, and if the tumor still existed at the tumor bed, then the Whipple procedure was performed.
The demographical features, tumor size, endoscopic tumor resectability, biochemical assays, and surgical outcomes were compared between the two groups.
Ethical ApprovalThis study was approved by the Ethics Committee of Afyonkarahisar Health Sciences University (Date: 2022-04-02, No: 2011-KAEK-2).
Statistical AnalysisNormal continuous and categorical variables were compared using Student’s t-test, Mann-Whitney U test, Chi-square test, and William’s Correction Chi-square test. A p-value <0.05 was considered to be statistically significant. Data analyses were performed using SPSS v20 statistical software (Chicago, IL).
Reporting GuidelinesThis observational retrospective study was reported in accordance with the STROBE guidelines.
Results
A total of forty-four patients were admitted to our centre with the diagnosis of ampullary tumor; one patient from group 1 and four from group 2 (a total of five patients) were treated with endoscopic ampullectomy, whereas 39 of them had a Whipple procedure between January 2014 to December 2023. None of the patients treated with endoscopic ampullectomy required further treatment for inadequate tumor clearance, and they were under follow-up for six months (Figure 1). Patients were evaluated using USG, CT, MRI/MRCP, and ERCP according to our clinical algorithm (Figure 2).
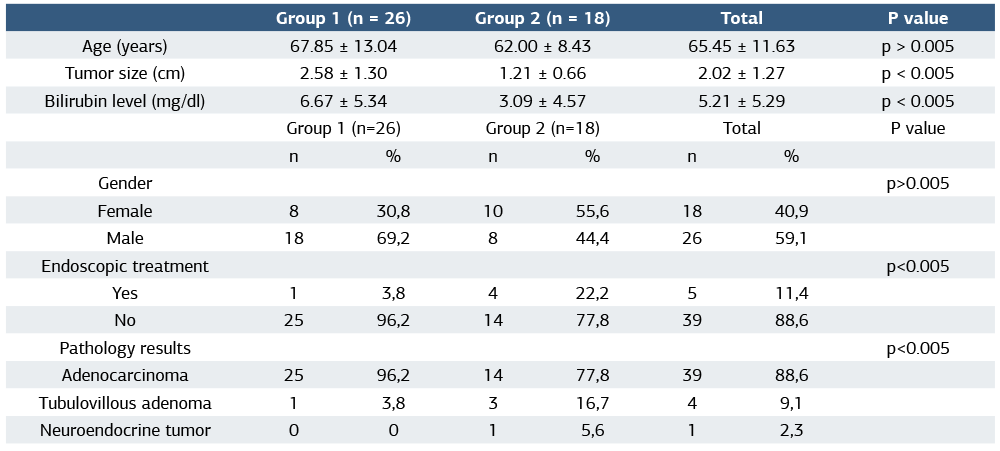
The patients were divided into two groups according to the method by which the diagnosis was made. The patients diagnosed with the presence of an ampullary mass on radiological images of USG, CT, and MRI/MRCP were included in group 1 (n = 26). The diagnosis of the ampullary tumor was confirmed with ERCP in this group, and endoscopic ampullectomy was performed for the patients whose lesion met the criteria defined previously (10), otherwise, biopsy was performed. The second group (Group 2) was patients in whom no mass was detected in imaging methods (n = 18). They had only slight to moderate dilatation, tapering, or blunt termination of bile ducts. The diagnosis could be ensured with ERCP in this group. Following the description of the tumor, biopsy or endoscopic ampullectomy was decided according to the criteria described previously (Table 1). When the mean age of the two groups was compared, it was 67.85 ± 13.04 years in group 1 and 62.00 ± 8.43 years in Group 2 (p > 0.05). Although there was no statistical significance, the patients diagnosed with ERCP were five years younger than the other group on average.
There was no gender difference, but overall, it was observed that ampullary tumors were more common in men than women (26 (59.1 %) vs 18 (40.9 %)) (Table 1).
The mean size of the tumor in group 1 was bigger than that of group 2 (2.58 ± 1.30 cm vs 1.21 ± 0.66 cm), and this difference was statistically significant (p < 0.05).
The bilirubin values were significantly higher in group 1 as compared to Group 2 (6.67 ± 5.34 mg/dl vs 3.09 ± 4.57 mg/dl, p < 0.05) (Table 1).
Additionally, a total of five EAs were performed on one patient from group 1 and four patients from Group 2. Since the surgical margins were free of tumors in all patients who underwent endoscopic ampullectomy, no additional surgical procedure (Whipple’s procedure) was required.
According to Fisher’s exact test and chi-square test, no significant difference was found in EA rates between the two groups. However, when William’s correction of chi-square was performed, the difference was significant; therefore, we were able to perform local resection in more patients of Group 2.
When the pathology results were evaluated, in group 1, 25 patients had adenocarcinoma (96.2 %), and one patient had tubulovillous adenoma (3.8%). In group 2, we found adenocarcinoma in 14 patients (77.8%), tubulovillous adenoma in 3 patients (16.7 %), and neuroendocrine tumor in one patient (5.6%) (Table 1).
Discussion
Ampullary neoplasms are rare tumors with earlier clinical presentation compared to pancreatic or cholangiocellular carcinomas. Although there is no definite consensus for the treatment, accurate diagnosis and staging are crucial for optimal therapy. A wide array of radiological procedures, such as USG initially and CT and MRI, are concurrently utilized for diagnosis to provide a guide for surgical decisions 11. The dilatation of intrahepatic and extrahepatic bile ducts is less than other periampullary tumors 12. CT is additionally valuable in detecting peripheral lymphadenopathy, but its diagnostic accuracy in assessing the lymph node in the extra-regional area is poor 13. Zhao et al. reported that out of the 26 patients with ampullary tumors, the average tumor size was 2.5 ± 0.6 cm, and 4 cases had peripheral lymphadenopathy 12. In our study, the means of the tumor size were 2.58 ± 1.30 cm and 1.21 ± 0.66 cm in groups 1 and 2, respectively. The detection of a mass (with a tumor size of 1.21 ± 0.66 cm) during pathological evaluation in Group 2, despite the absence of any mass on radiological images, is one of the most significant findings of this study.
CT allows the visualization of the ampullary region, and high- resolution images can be obtained for ampullary tumors 14. Angthong et al. reported that 13 out of 31 patients with ampullary carcinoma had no ampullary mass on CT 14. The bulging appearance was suggestive of malignancy. Abrupt narrowing of the bile duct and moderate to severe dilation were found to have a higher diagnostic value than the presence of mass alone on CT.
The present study was conducted on 44 patients with ampullary tumors, ranging in age from 44 to 76 years, between 2014 and 2023. It was found that 26 of them were diagnosed with radiological images (i.e., USG, CT, and MRI/MRCP), whereas 18 of them underwent diagnostic ERCP.
Considering that ampullary tumors do not usually dilate the bile and pancreatic ducts enough to be detected with MRI, it is probably required to use complementary invasive procedures, such as ERCP, to make the diagnosis. ERCP is an endoscopic procedure for the treatment of hepatobiliary and pancreatic diseases and is actually used for therapeutic purposes 15,16,17 rather than diagnosis due to its well-documented morbidity and mortality rates 18. However, in experienced hands, it can also be used for diagnostic purposes even in older ages; the most obvious one is the patients with ampullary tumors that do not display any radiological signs of a mass 18,19. In our study, there was no evidence of a mass compatible with an ampullary tumor on radiological images in 18 patients, and the diagnosis of ampullary tumor was made by ERCP in all of these patients. Patients diagnosed with ERCP were associated with more favorable outcomes than patients in other groups in terms of endoscopic resectability and earlier stage. While endoscopic ampullectomy could be achieved in one patient in Group 1, this could be ensured in four patients in Group 2.
Currently, specific guidelines on how to diagnose and stage ampullary tumors are lacking, and there is also no article comparing the results of ERCP and EUS in patients with ampullary tumors. Actually, they are not comparable but complementary to each other 20,21. But combining EUS with ERCP in the same session has been shown to be effective and safe for the patients 22. However, despite a lack of clear evidence, some endoscopists, especially when an EUS was not performed, recommend ERCP for some reasons: Side- viewing duodenoscopy is much preferred to evaluate ampullary tumors and has an opportunity for endoscopic resection and increases the accuracy of biopsies 22. Because the sensitivity and specificity of biopsy with side-viewing duodenoscopy are 63% and 100%, respectively. It also provides better information about the intraductal component of the tumor 23. However, it is strongly recommended that this procedure should be performed in centres led by endoscopists skilled in ERCP procedure and endoscopic resection methods, able to manage any adverse event 21.
While EUS offers promising results, its limited availability necessitates alternative strategies, such as ERCP. EUS has a high accuracy rate for the transmural depth of the tumor within the pancreas and bile duct, as well as the extension to peripheral lymph nodes 9. Despite these advancements in diagnostic imaging, challenges in managing patients with ampullary tumors still exist. In the absence of EUS availability, the use of ERCP ensures less invasive resections in treating patients with ampullary tumors. Since EUS is not available at our facility, we used ERCP in a diagnostic manner for the differential diagnosis of patients with tapering or blunt termination of the bile duct. Our high number of cases compared to other publications may be due to the fact that we are a center that performs around 500 ERCP procedures annually and over 15000 total. We do not have any mortality related to ERCP. So, ERCP offers a more minimal surgical treatment opportunity for small-sized ampullary neoplasms. However, due to well-known complications of the ERCP procedure, some of which can be very serious, we consider that this algorithm should only be applied in high-volume centres (˃200 procedures annually) and by experienced endoscopists (˃200 procedures annually) as described British Society of Gastroenterology. So the benefit of the patient should be balanced with considering the adverse events.
Local resection is decided with a duodenoscope if the tumor appears less than 3 cm, pedunculated, laterally spread not more than one cm, has regular margins, and can be removed completely. After resection, biopsies are taken with forceps from the tumor bed, and if the tumor still exists at the surgical margin, then radical resection (Whipple procedure) is planned. In summary, the present study suggests that early use of ERCP in diagnosing ampullary cancer is associated with better outcomes in terms of early diagnosis and endoscopic resection. It identifies the important role of ERCP for ampullary tumors to diagnose at an earlier stage and to treat more conservatively. Furthermore, it is also noteworthy to mention that we observed a mass relevant to ampullary tumors, even in patients with only mild to moderate dilatation, tapering, or abrupt termination of the bile duct.
Limitations
This study has some limitations. It was performed in a single center with a relatively small number of patients. More importantly, we could not precisely compare our results as no similar study was found in the literature on this topic. However, given that this is the first in this respect, our findings could be a guide for more comprehensive studies.
Conclusion
Although ERCP is an advanced interventional technique, has been developed for different therapeutic purposes, the Complementary use of it with the patient’s clinical and radiological findings provides the best results for diagnosing and treating ampullary tumors. It has potential advantages as providing endoscopic resection, obtaining more accurate biopsies, determining the tumor more precisely, evaluating the intraductal component of the tumor, and diagnosing the early stage. So, in centres where EUS is not available, ERCP can ensure a favourable outcome.
Declarations
Ethics Declarations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Afyonkarahisar Health Sciences University (Date: 02.04.2022, No: 2011-KAEK-2). The authors declare that they take full responsibility for the integrity of the study, including study design, data collection, analysis, interpretation, and manuscript preparation. There is no conflict of interest. No external funding was received.
Animal and Human Rights Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: M.B.K., S.Y.
Methodology: M.B.K., E.B.
Formal Analysis: E.B.
Investigation: M.B.K., C.O., K.E.
Data Curation: K.E.
Writing – Original Draft Preparation: M.B.K.
Writing – Review & Editing: E.B., E.T.U., S.Y.
Supervision: S.Y.
Abbreviations
CT: Computed Tomography
EA: Endoscopic Ampullectomy
ERCP: Endoscopic Retrograde Cholangiopancreatography
EUS: Endoscopic Ultrasound
MRI: Magnetic Resonance Imaging
MRCP: Magnetic Resonance Cholangiopancreatography
USG: Ultrasonography
References
-
Ito K, Fujita N, Noda Y, Kobayashi G, Horaguchi J. Diagnosis of ampullary cancer. Dig Surg. 2010;27(2):115-118.
-
Shin DW. Diagnostic approach for ampullary lesions. Korean J Gastroenterol. 2023;82(4):159-170.
-
Dubois M, Labgaa I, Dorta G, Halkic N. Endoscopic and surgical ampullectomy for non-invasive ampullary tumors: short-term outcomes. Biosci Trends. 2017;10(6):507-511.
-
Hennedige TP, Neo WT, Venkatesh SK. Imaging of malignancies of the biliary tract: an update. Cancer Imaging. 2014;14(1):14.
-
Brambs HJ, Claussen CD. Pancreatic and ampullary carcinoma. Ultrasound, computed tomography, magnetic resonance imaging, and angiography. Endoscopy. 1993;25(1):58-68.
-
Kim JH, Kim MJ, Chung JJ, Lee WJ, Yoo HS, Lee JT. Differential diagnosis of periampullary carcinomas at MR imaging. Radiographics. 2002;22(6):1335-1352.
-
Shrikhande SV, Barreto SG, Goel M, Arya S. Multimodality imaging of pancreatic ductal adenocarcinoma: a review of the literature. HPB (Oxford). 2012;14(10):658-68.
-
Gornals JB, Esteban JM, Guarner-Argente C, et al. Endoscopic ultrasound and endoscopic retrograde cholangiopancreatography: can they be successfully combined? Gastroenterol Hepatol. 2016;39(9):627-642.
-
Sauvanet A, Chapuis O, Hammel P, et al. Are endoscopic procedures able to predict the benignity of ampullary tumors?. Am J Surg. 1997;174(3):355-358.
-
Poley JW, Campos S. Methods and outcome of the endoscopic treatment of ampullary tumors. Ther Adv Gastrointest Endosc. 2020,13:1–13.
-
Patel VB, Musa RK, Patel N, Patel SD. Role of MRCP to determine the etiological spectrum, level and degree of biliary obstruction in obstructive jaundice. J Family Med Prim Care. 2022;11(7):3436-3441.
-
Zhao DZ, Guo Y, Sun YP, et al. Multi-detector spiral CT diagnosis of common bile duct ampullary carcinoma. Eur Rev Med Pharmacol Sci. 2017;21(16):3549- 3553.
-
Tseng DS, van Santvoort HC, Fegrachi S, et al. Diagnostic accuracy of CT in assessing extra-regional lymphadenopathy in pancreatic and peri-ampullary cancer: a systematic review and meta-analysis. Surg Oncol. 2014;23(4):229-235.
-
Angthong W, Jiarakoop K, Tangtiang K. Differentiation of benign and malignant ampullary obstruction by multi-row detector CT. Jpn J Radiol. 2018;36(8):477-488.
-
Yılmaz S, Akıcı M, Şimşek M, Okur N, Erşen O, Tuncer AA. Endoscopic retrograde cholangiopancreatography for biliary system parasites. Turk J Surg. 2018;34(4):306-310.
-
Emre B, Mehlika BK, Metehan A, Taylan UE, Sezgin Y. The effect of previous endoscopic retrograde cholangiopancreatography on subsequent laparoscopic cholecystectomy: The retrospective analysis of 1500 patients. J Minim Access Surg. 2024;20(4):414-419.
-
Bilgi Kırmacı M, Akay T, Özgül E, Yılmaz S. Cholecysto-hydatid cyst fistula: a rare cause of cholangitis. Am J Case Rep. 2020;21:e921914.
-
Ugurlu ET, Yilmaz S. Diagnosis and Management of ERCP complications: the results of 15000 cases from two centres. Ulutas Med J. 2023;9(1):51-57.
-
Ademoglu S, Ademoglu Z, Yilmaz S, Arikan Y. Is endoscopic retrograde cholangiopancreatography safe in elder patients: a single center experience. EJMI. 2021;5(1):51-56.
-
Maselli R, de Sire R, Fugazza A, et al. Updates on the management of ampullary neoplastic lesions. Diagnostics (Basel). 2023;13(19):3138.
-
de Wilde AJ, de Jong EJM, Gurusamy KS, et al. Diagnostic accuracy of cross- sectional and endoscopic imaging in ampullary tumours: systematic review. Br J Surg. 2024;111(1):znad432.
-
Campos ST, Bruno MJ. Endoscopic papillectomy. Gastrointest Endosc Clin N Am. 2022;32(3):545-562.
-
Stornello C, Cristofori C, Checchin D, et al. The role of endoscopic ultrasound in ampullary lesion management. Diagnostics (Basel). 2024;14(17):1855.
Figures
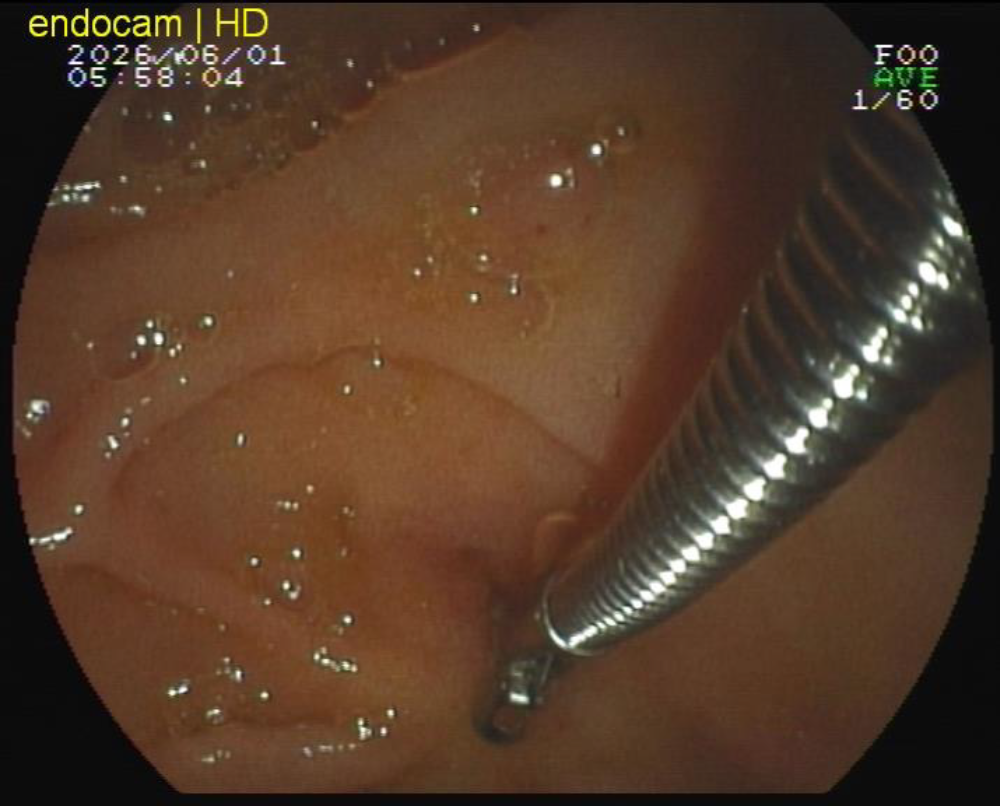
Figure 1. An endoscopic view six months after the endoscopic resection of the ampullary tumor
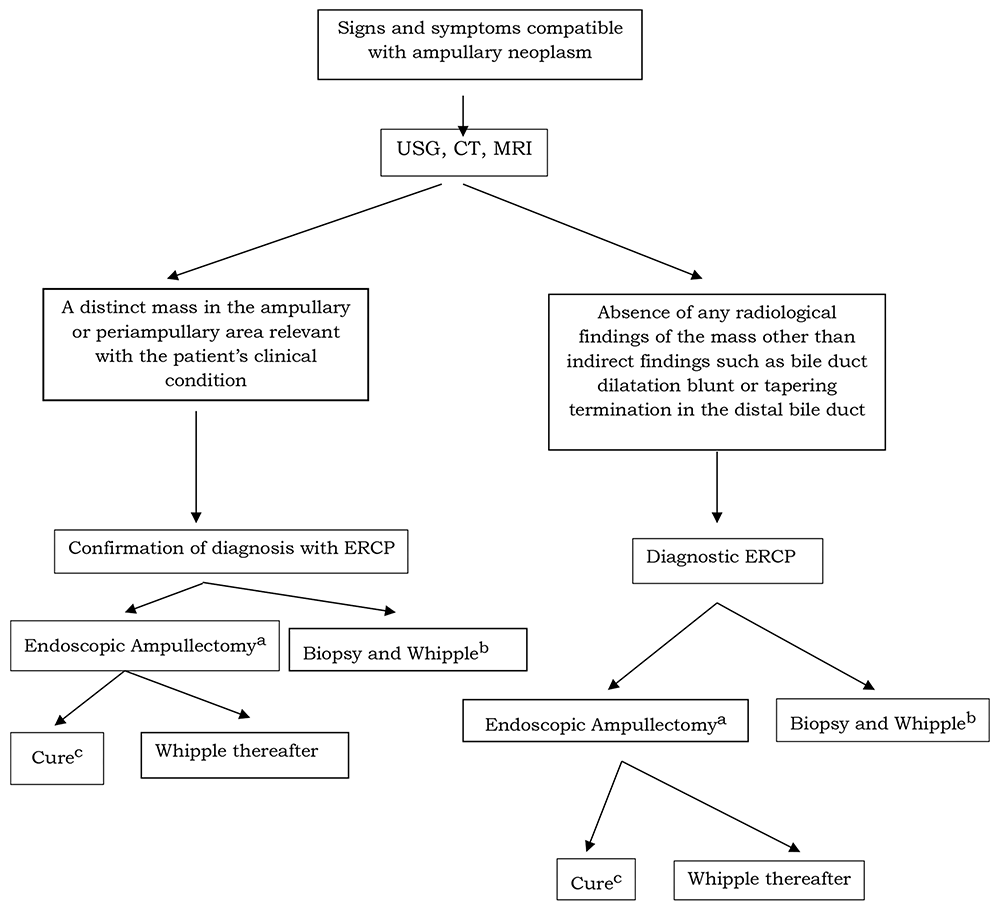
Figure 2. An algorithm for patients suspected of ampullary neoplasm for diagnosis and treatment a. Endoscopic ampullectomy was decided if the lesion was less than 3 cm in size, had a pedunculated shape, spread laterally by no more than 1 cm, exhibited a regular margin, and was deemed removable entirely b. The lesions are not suitable for Endoscopic Ampullectomy. The confirmation of diagnosis with biopsy and then definitive surgical (Whipple) procedure c. Biopsies were taken from the tumor bed after Endoscopic Ampullectomy. If the result is negative, the patient is accepted as cured; if the tumor still exists, then the Whipple procedure is performed
Tables
Table 1. Comparison of the data between groups of patients treated for ampullary neoplasm with and without tumoral mass on radiological images
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mehlika Bilgi Kirmaci, Emre Balli, Cigdem Ozdemir, Kubra Ertekin, Esat Taylan Ugurlu, Sezgin Yilmaz. The role of ERCP in the diagnosis of ampullary tumors in patients with absent mass on radiological findings. Ann Clin Anal Med 2026;17(4):308-312. doi:10.4328/ACAM.22694
- Received:
- April 8, 2025
- Accepted:
- May 12, 2025
- Published Online:
- July 30, 2025
- Printed:
- April 1, 2026