
Percutaneous endoscopic gastrostomy: a single center experience
PEG: A single center experience
Authors
Abstract
Aim Percutaneous endoscopic gastrostomy (PEG) is a frequently preferred method for patients with swallowing disorders who are unable to take oral food for more than one month. PEG has many minor and major complications. 30-day mortality rate after PEG is variable.
Methods All data from patients with PEG application at the endoscopy unit of Antalya Serik State Hospital, between October 2019 and September 2022, were retrospectively analyzed.
Results Median age of 83 patients was 81. Majority of the patients (97.6%) were hospitalised at palliative care or intensive care units before PEG, most having multiple concomitant diseases. Dementia and cerebrovascular problems were major indications. All of the procedures were successful.
Minor complication rate was 20.4% while major was 2.4%. There was no mortality related to the interventions. 30-day mortality rate was 18.2% whereas mean survival time was 10 (%95 CI: 7.7-13.1) months.
Conclusion PEG procedure is an easily tolerated, effective, and safe method, with a low rate of major complications. For maintenance of enteral nutrition due to swallowing dysfunction, PEG should be considered. Great attention to the patient’s present conditions and 30-day life expectancy should be given while patient selection for PEG. A surgical perspective, proper education of the patients’ relatives, and a regular home care service are needed for accurate evaluation of complications.
Keywords
Introduction
Percutaneous endoscopic gastrostomy (PEG) is among the most commonly used methods to provide enteral nutrition in patients whose gastrointestinal system (GIS) integrity is preserved but oral food intake cannot be provided due to impaired or no swallowing function 1,2. Gauderer et al. 3 were the first to describe and apply PEG in 1980. PEG is an effective method that can be applied under local anesthesia and sedation, does not require operating room conditions, and can be applied quickly and safely at endoscopy units and the bedside of hospitalised patients 4,5. It is recommended to apply PEG procedure to all patients who could not have been fed via oral route for more than one month 1,6. The most common causes of dysphagia in patients undergoing PEG are cerebrovascular diseases, motor neuron diseases, cancer, head, and neck trauma 7. PEG procedure is a minimally invasive option which has lower cost and is less risky in comparison to surgical gastrostomy, and education of relatives of the patients about nutrition via PEG is easy 1,5. Perforation of colon, liver injury, gastric wall necrosis, gastrocolic fistula, bleeding, and peritonitis are among the most dramatic major complications of PEG 5,8. Among the minor PEG complications, occlusion of the catheter, leakage from the catheter insertion site, and infection around the catheter insertion site are the most common 8. 30-day mortality rate following the PEG procedure was reported as 3.3-23.9% previously 9. In this research, we primarily aimed to analyse indications and complications of PEG and 30-day mortality after the intervention by evaluating the PEG procedures in our hospital.
Materials and Methods
All data of the patients who underwent PEG application at the endoscopy unit of Antalya Serik State Hospital between October 2019 and September 2022 were retrospectively analysed and evaluated. Age and gender of the patients, primary pathology causing dysphagia, comorbidities, clinics at which patients were followed up, complications related to the procedures, morbidity, and mortality in the post-procedure period were recorded. Before the procedure, detailed blood tests of the patients, including bleeding and coagulation times, were examined. Also, PCR tests for COVID-19 infection were done in the last 24 hours before PEG application after the onset of the pandemic. Procedure decision was not made for four inpatients with dysphagia, for whom consultation was requested for PEG insertion, as it was observed that enteral feeding periods via nasogastric tube were less than one month. The patients were fasted eight hours before the procedure, and routine prophylactic antibiotic administration was not applied to the patients. Sedation was administered by anesthesiologists during the interventions (0.05 mg/kg intravenous midazolam), and continuous monitoring had been maintained by recording oxygen saturation, blood pressure, and pulse rate throughout the procedures. All interventions were performed by the same general surgeon with experience of more than five years in GIS endoscopy. Fujinon EG-530WR brand video endoscopy system and 20 French PEG kits were used in all of the procedures in which pull method had been preferred. Enteral nutrition was started two hours after PEG procedures. Current practices were taken as a basis when evaluating indications and complications in PEG 9,10,11,12.
Ethical ApprovalThis study was approved by the Ethics Committee of Akdeniz University Faculty of Medicine Hospital (Date: 2022-12-07, No: 749).
Statistical AnalysisContinuous variables are reported as medians (min-max), and categorical variables as counts and percentages. Time of survival was calculated between the date of PEG application and last examination of the patient or date of exitus. The values used in the survival analysis and the survival graph were analysed by Kaplan-Meier method. P values lower than 0.05 (p<0.05) were considered statistically significant. All statistical analyses were performed by using IBM SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, N.Y., USA).
Reporting GuidelinesThis observational retrospective study was reported in accordance with the STROBE guidelines.
Results
Of the 83 patients who underwent PEG, 41 (49.4%) were male and 42 (50.6%) were female; the median age was 81 (29-98) (Table 1). Eight (9.6%) of the patients had previous abdominal surgery. Before the intervention, 45 (54.2%) of the patients were being followed up in the palliative care unit of our hospital, 36 (43.4%) were being followed up in our intensive care unit, while two (2.4%) patients had been treated with a day hospitalization (Table 1). Within the concomitant systemic diseases of the patients, the most common were hypertension, diabetes mellitus, stroke, and cardiac problems (Table 1).
All of the PCR test results of the patients for COVID-19 infection before the PEG procedure were negative. PEG procedures were successfully applied to all of the patients. When the primary diseases of the patients leading to dysphagia were evaluated, dementia came first with 60.3% (50 patients), being followed by cerebrovascular diseases with 27.7% (23 patients) (Table 2). Sixteen (19.3%) out of 83 patients had previous PEG placements at an external center, but their current catheters were not functioning (due to, for example, tube blockage or rupture of the tube) and PEG replacements had been performed on them.
Since most of the patients who underwent PEG procedure were in hospitalized status, daily follow-ups could be done regularly. Our patients who had day-to-day procedures were also evaluated by the home care unit starting from the week after the procedure.
Periostomal leakage was observed in five (6.0%) patients, periostomal infection in four (4.8%) patients, rupture of the tube in two (2.4%) patients, and tubal blockage and bleeding from the granulation tissue at the site of tube entry, each in one (1.2%) patient (Table 3). Also buried bumper syndrome had been observed in two (2.4%) patients during the follow- up period after the procedure (Table 3). The catheters of four (4.8%) patients with Alzheimer’s disease and cerebrovascular disorder happened to be removed due to self-pulling while they were at home or in the palliative care unit (Table 3). Within the mentioned complications, leakage from the catheter insertion site and infection around the catheter were detected in the early period, whereas all of the other complications were encountered in the late period (Table 3). Our complication rate was 10.8% in the early period and 12.0% in the late period, and all complications except for two cases with buried bumper syndrome were minor complications (Table 3). Our minor complication rate was 20.4% while major was 2.4% (Table 3). The problems of patients with periostomal leakage and infection were resolved by conservative treatment methods. PEG procedures were performed again in the other 10 patients with described problems (Table 3). No mortality associated with PEG application was observed in any patient.
30-day mortality rate was 18.2% and 15 patients died in the first month following PEG procedure due to causes related to their primary health problem. Median follow-up period was 3 (0.3-28) months. Mortality was observed in 52 (62.7%) patients throughout the whole follow-up period. Mean time for survival was 10 (%95 CI: 7.7-13.1) months (Figure 1).
Discussion
In our research, PEG procedure was applied mainly to patients with chronic neurological disorders who were mostly hospitalised at the palliative care unit of our hospital and fed through a nasogastric tube. Although in many previous studies, the most common cause of dysphagia in patients who underwent PEG was found to be cerebrovascular diseases, followed by dementia dominated neurological problems 10,13, similar to what Saka et al. 12 documented, in our data, the opposite was observed. The fact that the capacity of palliative care unit of our hospital, where most of the patients were having treatment due to chronic neurological disorders, was higher than that of our intensive care unit, the effective use of our palliative care unit and the fact that our intensive care unit beds were being predominantly used by covid 19 infected patients due to the pandemic, can explain the difference about this issue with many other researches.
Different approaches have been identified in different studies on the use of prophylactic antibiotics before the PEG procedure 5,9. A systematic review by Lipp and Lusardi demonstrated that prophylactic antibiotic administration significantly reduces the risk of peristomal wound infection following PEG placement 14 . According to the ESPEN guideline 11 on clinical nutrition in the intensive care unit, routine antibiotic prophylaxis before PEG is not universally recommended and should be individualized based on center experience and patient condition. However, ESPEN guideline recommends antibiotic use in doubtful cases and in centers with limited experience. In our practice, we did not administer prophylactic antibiotics to any patient, except for the patients who were receiving antibiotherapy in the inpatient service, and we did not administer antibiotics after the procedure, since we did not have any cases in doubt.
According to a Cochrane systematic review by Gomes et al. 15, PEG placement is associated with a higher success rate, improved long-term nutritional outcomes, and lower complication rates compared to nasogastric tube feeding in adults with swallowing disturbances. whereas Yuruker et al. 16 determined a successful application rate of 98%. There are also other studies in which success rate is significantly lower 4,17. In our study, the successful procedure rate was found to be 100%.
There is no standard practice regarding the timing of initiation of enteral feeding in patients undergoing PEG 5,18,19. In previous research, approaches ranging from 1 hour to 24 hours have been encountered about the same issue 4,5,11,18,20. We routinely switched to enteral feeding two hours after the PEG procedure, and we did not observe any significant problem.
In the literature, mortality related to PEG intervention is generally defined as close to zero in patients who had undergone PEG 1,5. Ozguc et al. 5 evaluated total complication rate of PEG procedures as 8-30% and serious complication rates as 1-4% whereas Stenberg et al. 21 and Vujasinoviç et al. 22 defined minor and major complications due to PEG as 18-38% and 2-4% respectively. Although the majority of complications are local problems, serious complications such as colon perforation and peritonitis can also develop 5,8,12. In our study, neither mortality nor life-threatening serious complications associated with the PEG procedure occurred, and our complication rates are compatible with the literature.
Almost all of our patients had advanced age, and they were either having treatment at the palliative care unit or were hospitalised at the intensive care unit (except for the two patients with a day hospitalisation). Besides, a significant portion of them had several important systemic diseases. Probably due to these reasons, our 30-day mortality rate appeared to be high in comparison to some of the research established previously 12,13. When choosing a patient for PEG application, an evaluation should be made taking into account the patient’s age, current health problems, and 30-day life expectancy 9,12,21,23,24.
In our study, it was determined that the catheters removed in the late period were withdrawn by the patients themselves, all of whom had the diagnosis of either Alzheimer’s disease or stroke. We think that the role of these conditions was quite important in the problem that occurred in the follow-up of these patients. In order to prevent inadvertent PEG removals due to self-pulling (especially when the patient is at home), educating the relatives of the patients and providing a regular home care service may be beneficial.
Limitations
Our limitations were that our research was a single-center low low-volume study with retrospective design. By means of prospective multicenter studies having a larger number of patients, especially involving determinative criteria in patient selection for PEG more meaningful results might be obtained.
Conclusion
PEG procedure is an effective and safe method, with a low rate of major complications, easily tolerated by the patients. In cases in which long-term enteral nutrition should be established due to swallowing dysfunction, PEG should be considered.
However, great attention should be given regarding patients’ present conditions and 30-day life expectancy while patient selection for PEG. A surgical perspective, together with the proper education of the relatives of the patients and a regular home care service, would be more appropriate for accurate evaluation of minor and major complications.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Akdeniz University Faculty of Medicine Hospital (Date: 2022-12-07, No: 749) and was conducted in accordance with the Declaration of Helsinki.
Animal and Human Rights Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.G., D.S.Ü.
Methodology: G.G., D.S.Ü.
Formal Analysis: G.G.
Investigation: G.G., D.S.Ü., A.Ö., S.Ç.
Data Curation: G.G.
Writing – Original Draft Preparation: G.G.
Writing – Review & Editing: D.S.Ü., A.Ö., S.Ç.
Supervision: S.Ç.
Abbreviations
CI: Confidence Interval
COVID-19: Coronavirus Disease 2019
ESPEN: European Society for Clinical Nutrition and Metabolism
GIS: Gastrointestinal System
PEG: Percutaneous Endoscopic Gastrostomy
PCR: Polymerase Chain Reaction
References
-
Şenlikçi A, Kuzu UB, Dede F, Yüce K. İkinci basamak hastanede perkütan endoskopik gastrostomi deneyimlerimiz [Percutaneous endoscopic gastrostomy: experience in a secondary level hospital]. Endoskopi Gastrointestinal. 2018;26(3):95-98.
-
Wesley S, Samuels N, Williams K, et al. Early versus late tube feeding initiation after PEG tube placement: does time to feeding matter? Injury. 2021;52(5):1198- 203.
-
Gauderer MW, Ponsky JL, Izant RJ Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980;15(6):872-875.
-
Lang K, ElShafie RA, Akbaba S, et al. Endoscopic gastrostomy tube placement in patients with head and neck cancer treated with radiotherapy. Cancer Manag Res. 2020;12:127-136.
-
Ozgüc H, Gökce E, Altınel Y, Kırdak T. Percutaneous endoscopic gastrostomy experience in a general surgery clinic. Turk J Surg. 2011;27(3):145-148.
-
Boylan C, Barrett D, Li V, Merrick S, Steed H. Longitudinal complications associated with PEG: rate and severity of 30-day and 1-year complications experienced by patients after primary PEG insertion. Clin Nutr ESPEN. 2021;43:514-521.
-
Gundogan K, Yurci A, Coskun R, et al. Outcomes of percutaneous endoscopic gastrostomy in hospitalized patients at a tertiary care center in Turkey. Eur J Clin Nutr. 2014;68(4):437-440.
-
Boeykens K, Duysburgh I, Verlinden W. Prevention and management of minor complications in percutaneous endoscopic gastrostomy. BMJ Open Gastroenterol. 2022;9(1):e000975.
-
Ergenç E, Derici ST, Uprak TK. Percutaneous endoscopic gastrostomy: a secondary care hospital experience. Laparosc Endosc Surg Sci. 2021;28(4):210-214.
-
Rahnemai-Azar AA, Rahnemaiazar AA, Naghshizadian R, Kurtz A, Farkas DT. Percutaneous endoscopic gastrostomy: indications, technique, complications and management. World J Gastroenterol. 2014;20(24):7739-7751.
-
Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48-79.
-
Saka B, Zirtil C, Erten SN, et al. Indications, effectiveness and safety of percutaneous endoscopic gastrostomy: a single center experience and literature review. Asia Pac J Clin Nutr. 2021;30(1):42-50.
-
Schneider AS, Schettler A, Markowski A, et al. Complication and mortality rate after percutaneous endoscopic gastrostomy are low and indication-dependent. Scand J Gastroenterol. 2014;49(7):891-898.
-
Lipp A, Lusardi G. A systematic review of prophylactic antimicrobials in PEG placement. J Clin Nurs. 2009;18(7):938-948.
-
Gomes CA Jr, Andriolo RB, Bennett C, et al. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2015;2015(5):CD008096.
-
Yuruker S, Koca B, Karabicak I, Kuru B, Ozen N. Percutaneous endoscopic gastrostomy: technical problems, complications, and management. Indian J Surg. 2015;77(Suppl 3):1159-1164.
-
Coşkun O, Arı D. Results of percutaneous endoscopic gastrostomy: evaluation of 58 cases. Endoscopy Gastrointestinal. 2019;27(3):93-96
-
Ali T, Le V, Sharma T, et al. Post-PEG feeding time: a web-based national survey amongst gastroenterologists. Dig Liver Dis. 2011;43(10):768-771.
-
Garner SM, Reparaz L, Justice J, et al. Percutaneous endoscopic gastrostomy placement in trauma patients: early vs delayed initiation of enteral feeding. Am Surg. 2023;89(7):3336-3338.
-
Shahmanyan D, Lawrence JC, Lollar DI, et al. Early feeding after percutaneous endoscopic gastrostomy tube placement in patients who require trauma and surgical intensive care: a retrospective cohort study. JPEN J Parenter Enteral Nutr. 2022;46(5):1160-1166.
-
Stenberg K, Eriksson A, Odensten C, Darehed D. Mortality and complications after percutaneous endoscopic gastrostomy: a retrospective multicentre study. BMC Gastroenterol. 2022;22(1):361.
-
Vujasinovic M, Ingre C, Baldaque Silva F, Frederiksen F, Yu J, Elbe P. Complications and outcome of percutaneous endoscopic gastrostomy in a high- volume centre. Scand J Gastroenterol. 2019;54(4):513-518.
-
Farrag K, Shastri YM, Beilenhoff U, Aksan A, Stein J. Percutaneous endoscopic gastrostomy (PEG): a practical approach for long-term management. BMJ. 2019;364:k5311.
-
Strijbos D, Keszthelyi D, Gilissen LPL, et al. Percutaneous endoscopic versus radiologic gastrostomy for enteral feeding: a retrospective analysis on outcomes and complications. Endosc Int Open. 2019;7(11):E1487-E1495.
Figures
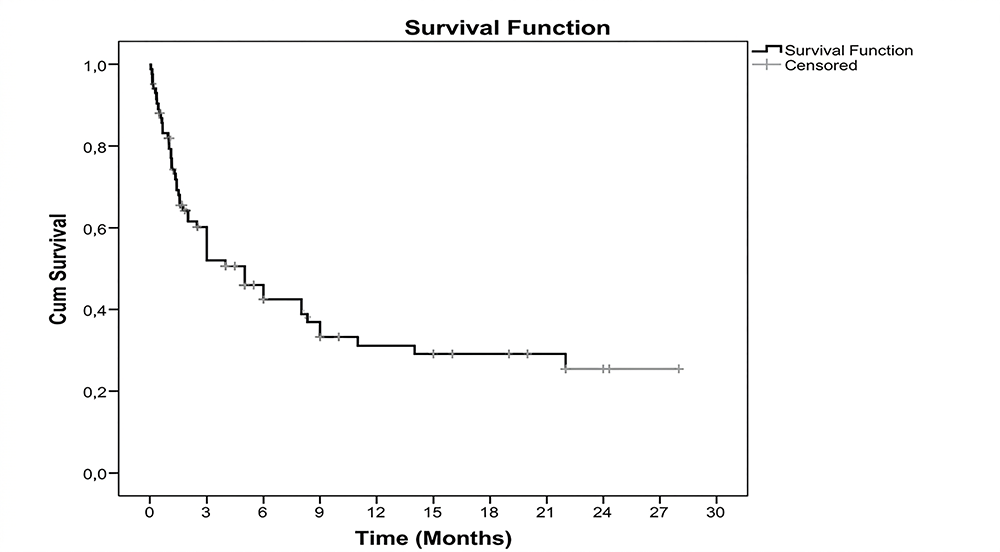
Figure 1. Overall survival curve of the patients
Tables
Table 1. Demographics and concomitant systemic diseases of patients, clinics where patients were followed up
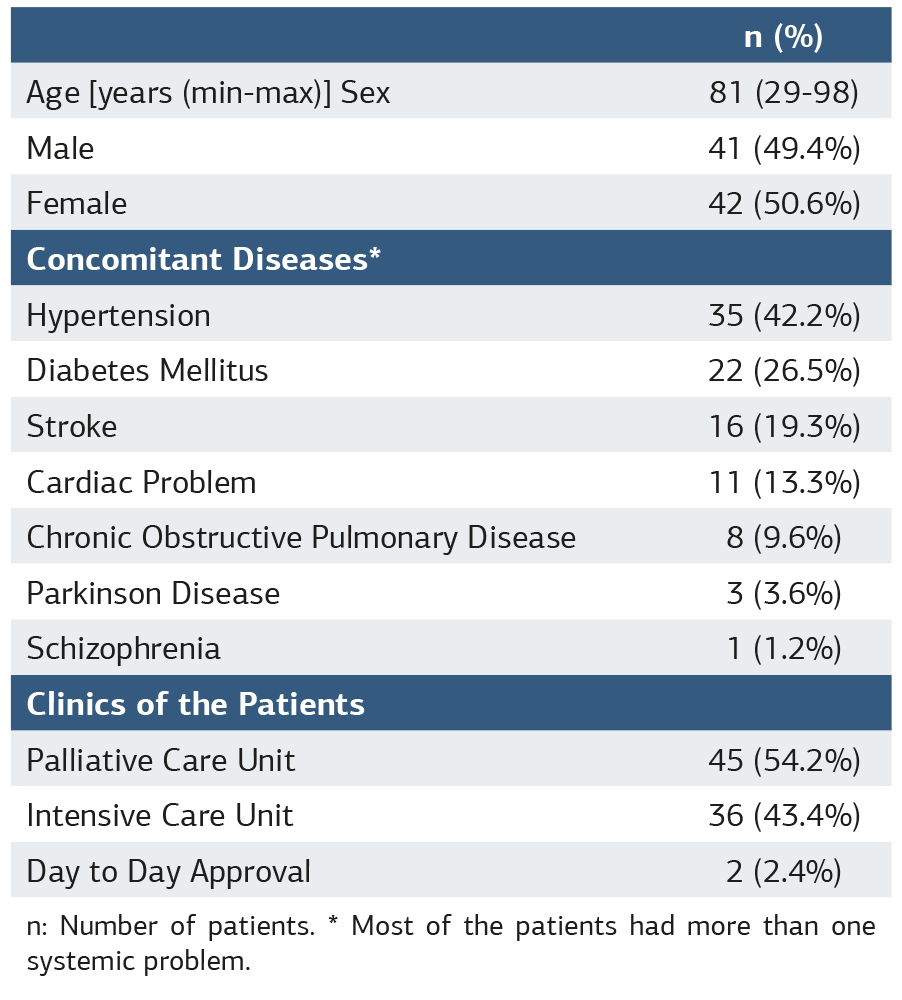
n: Number of patients. * Most of the patients had more than one systemic problem.
Table 2. Indications of percutaneous endoscopic gastrostomy
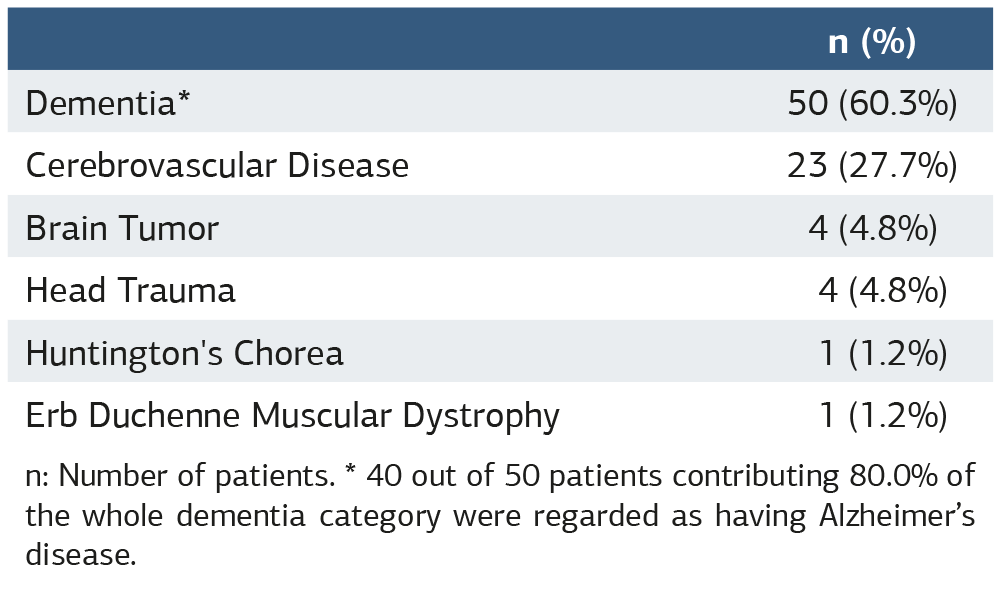
n: Number of patients. * 40 out of 50 patients contributing 80.0% of the whole dementia category were regarded as having Alzheimer’s disease.
Table 3. Complications of percutaneous endoscopic gastrostomy
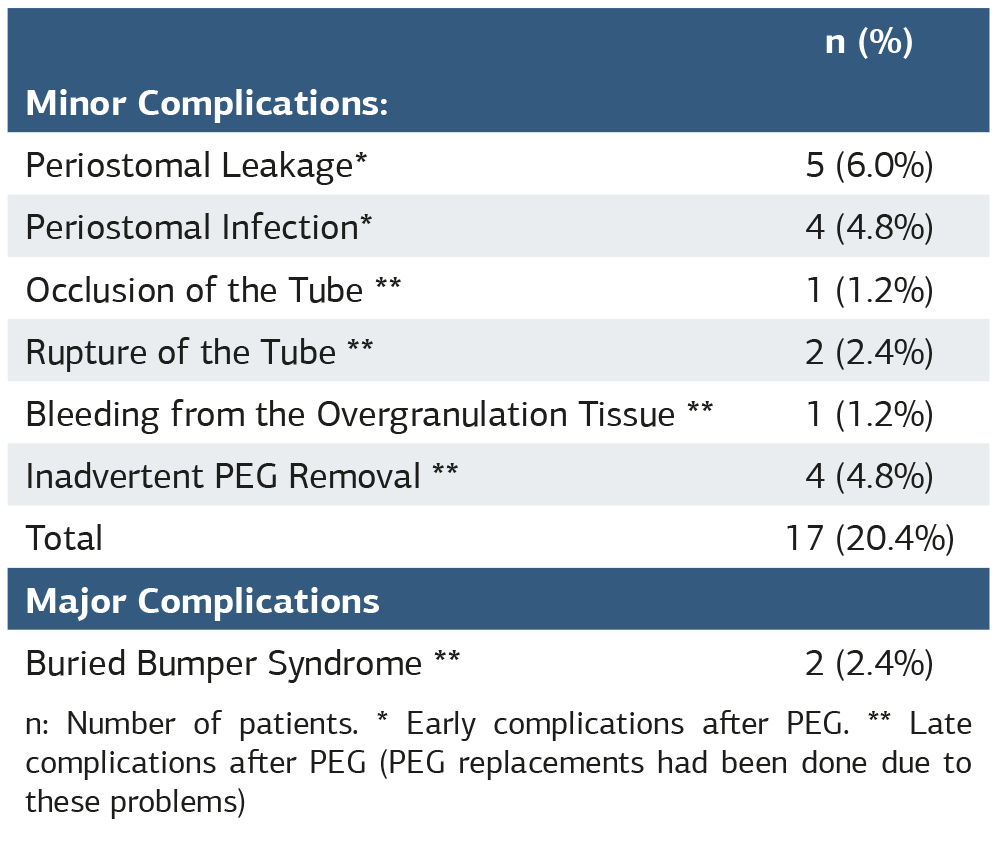
n: Number of patients. * Early complications after PEG. ** Late complications after PEG (PEG replacements had been done due to these problems)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gökmen Güzel, Demet Sarıdemir Ünal, Anıl Özen, Sinan Çetin. Percutaneous endoscopic gastrostomy: a single center experience. Ann Clin Anal Med 2026;17(4):313-317. doi:10.4328/ACAM.22713
- Received:
- April 17, 2025
- Accepted:
- July 28, 2025
- Published Online:
- August 7, 2025
- Printed:
- April 1, 2026