
Anatomical analysis of the hypoglossal canal in dry skulls
Hypoglossal canal anatomy
Authors
Abstract
Aim In the occipital bone, located at the lower back of the skull, the foramen magnum is adjacent to the occipital condyle, and the hypoglossal canal is located at the base of the occipital condyle. Measurements and morphological evaluations were conducted on bones from the Anatolian population to raise awareness of variations and contribute to clinical practice.
Methods Thirty-two dry skull bones of unknown age and gender were examined in the anatomy laboratory. Measurements were made with a digital caliper. Morphometry and type characteristics of the hypoglossal canal in the occipital bone were evaluated. The presence of accessory canals was examined.
Results When the 64 hypoglossal canals examined (right 32, left 32) were evaluated based on the presence of septum and notch, the number of Type 1 canals was found to be 33, and the number of Type 2 canals was 12. The location of the internal and external openings of the hypoglossal canal was found in the middle third of the condyle in 94% of cases.
Conclusion The septum of the canal is clinically important because it affects the hypoglossal nerve. While there are studies that are consistent with the anteroposterior length values of the hypoglossal canal, there are also studies that are dissimilar depending on the measurement technique and age. A thorough understanding of anatomical variation and morphometry at the skull base is crucial for accurate diagnosis and treatment. Measurements and awareness of the adjacent relationships are also beneficial for clinicians when considering surgical approaches.
Keywords
Introduction
Posteriorinferior skull contains the occipital bone. The foramen magnum, the largest skull aperture, connects the posterior cranial cavity to the spinal canal at the core of the occipital bone. The basion and opisthion are the midpoints of the anterior and posterior foramen magnum margins. The hypoglossal canal (HC) runs from the posterior cranial fossa at the base of the occipital condyle.1,2 A branch of the ascending pharyngeal artery, an emissary vein, a rare vertebrobasillar system member, and the nerve’s venous plexus are also in the HC. The jugular tubercle surrounds the HC from above, which is usually single or divided into two by a thin bone spicule.3 Clinically, canal morphology can impact the hypoglossal nerve.4 Modern humans’ greater speech abilities have caused the hypoglossal nerve, which has richer motor fibers, to grow the canal.5 Due to its proximity and features, the canal is prone to fractures, congenital abnormalities, schwannomas, glomus tumors, aneurysms, meningiomas, and cancer metastases.6 Understanding the anatomical and morphometric properties of these structures may help clinicians avoid difficulties in microsurgical procedures, such as the transcondylar approach (TCA), suboccipital subtonsillar approach (STA), and infratemporal approach (ITA).4 We employed a holistic approach to investigate how the morphometric and morphological properties of the HC in the skull base may impact clinical scenarios. In addition to prior studies, our study of the Anatolian population aimed to expand awareness and expertise in skull base surgery, thereby aiding surgeons in treating patients in the region.
Materials and Methods
After obtaining ethics approval, 32 skull bones of unknown age and gender, except for those with severe deformities and fractures, were examined. The measurements were carried out twice by the same researcher with a 15-day gap and evaluated based on their means. The intraclass correlation coefficient (ICC) was calculated to assess intra-observer reliability. We found exceptional reliability, with values above 0.9 across all parameters. Anatomical structures were measured with a digital caliper (Insize 1108/Suzhou, PRC), including a measuring range of 0–150 millimeters (mm) and a sensitivity of 0.03 mm.
The obtained data were recorded as mean ± standard deviation and percentages. The chi-square test was used to compare categorical data. For comparisons between two groups, the Student t-test (t-test for independent group) was applied when parametric conditions were met, and the Mann-Whitney U test was applied using IBM SPSS when parametric conditions were not met. p<0.05 was considered statistically significant.
In our study, the morphological evaluation of the HC based on the presence of septum and notch was performed using the classification proposed by Hauser and Stefano.4
Morphometric values examined were as follows (Figure 1):
- The width of the internal opening (anterior-posterior border) of the HC (HCIW)
- The height of the internal opening (upper-lower border) of the HC (HCIH)
- The width of the external opening of the HC (HCEW)
- The height of the external opening of the HC (HCEH)
- The anterior wall length of the HC (HCAL)
- The posterior wall length of the HC (HCPL)
- The distance of the internal opening of the HC to the basion (HCIB)
- The distance of the internal opening of the HC to the opisthion (HCIO)
- Septum length (SL)
- The width of the internal opening of the accessory canal (ACIW)
- The height of the internal opening of the accessory canal (ACIH)
- The width of the external opening of the accessory canal (ACEW)
- The height of the external opening of the accessory canal (ACEH)
- The anterior wall length of the accessory canal (ACAL)
- The posterior wall length of the accessory canal (ACPL)
Ethical ApprovalThis study was approved by the Local Ethics Committee of Selcuk University Faculty of Medicine (Date: 01.08.2023, Decision No: 2023/371).
Statistical AnalysisAll measurements were performed twice by the same researcher at a 15-day interval, and the mean values were used for analysis. Intra-observer reliability was evaluated using the intraclass correlation coefficient (ICC). Descriptive data were expressed as mean ± standard deviation and percentage. The chi-square test was used for categorical variables. The Student t-test was applied for normally distributed data, and the Mann-Whitney U test was used for non-normally distributed data. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). A p value <0.05 was considered statistically significant.
Reporting GuidelinesSpecific reporting guideline checklists were not considered necessary due to the descriptive anatomical design of the study based on dry skull specimens.
Results
Morphological ResultsWhen the 64 HCs (32 right, 32 left) were evaluated based on the presence of septum and notch, 33 canals were identified as Type 1, 12 as Type 2, four as Type 3, 14 as Type 4, and one as Type 5 (Figure 2). Type 1 was the most common canal type on both sides, with 56.3% on the right and 46.9% on the left. Only one Type 5 canal was present on the right side. No Type 3 canal was observed on the right side, while four (6.25%) Type 3 canals were observed on the left. There was a difference between the right and left canals in 20 of the 32 skulls. The chi-square test revealed no statistically significant difference between the right and left sides. When the canals were reclassified according to the presence of a septum (Types 1, 2, 3 = no septum; Types 4, 5 = septum present), a septum was observed in five (7.81%) canals on the right and six (9.3%) canals on the left.
The location of the internal (IHC) and external (DHC) openings of 59 HCs was defined relative to the condyle (Figure 3). Accordingly, all but three of the internal openings were located in the middle third of the condyle (n=56, 94.9%). One internal opening was located in the anterior third, and two in the posterior third. There was no difference between the right and left sides, except that in one skull, the left opening was anterior, while the right canal was located in the middle third of the condyle.
The external openings of the canals were located in the anterior third of the condyle in 52 (88%), except for seven. The other seven opened into the middle third. Except for three skulls, no differences were observed between the right and left sides. In Types 4 and 5, the location of the major (main) canal was evaluated.
Morphometric ResultsThe mean measurements of the 64 HCs are given in Table 1. No significant difference was found between the right and left sides (p>0.05).
The mean values of 49 HCs without a septum (Types 1, 2, 3) and 15 HCs with a septum (Types 4 and 5) are shown in Table 2. The measurements of the accessory (minor) canal in types 4 and 5 are given in Table 3.
The HCIW and HCIHa values of the accessory canal in types 4 and 5 were significantly lower than those of the main canals. The HCIW and HCIHa values of the main canal in Type 4 were significantly lower than those in Types 1 and 2, while HCALa was significantly higher than that in Type 1 (p<0.05). The type 5 canal was not tested due to insufficient samples. There was no significant difference between the other canal types and between the right and left sides.
When comparing the sides of the HC types, type 1 (n=33) was observed in 46.9% on the left and 56.3% on the right. Type 2 (n=12) was found in 15.6% on the left and 21.9% on the right. Type 3 (n=4) was present in 12.5% on the left and absent on the right. Type 4 (n=14) was detected in 25% on the left and 18.8% on the right. Type 5 (n=1) was absent on the left and present in 3.1% on the right. No statistically significant difference was found between the right and left sides (p=0.207).
The mean values of the shortest distance from the HC to the basion (HCIB) and to the opisthion (HCIO) were 15.29 ± 1.42 mm and 29.87 ± 2.20 mm, respectively. A strong positive correlation was found between HCIB and HCIO, but no significant difference was found between the right and left sides (p>0.05).
Discussion
Variations in the HC may influence the nerve clinically. Modern humans have more motor nerves in the HC, which has grown due to their improved speech ability. It can be impacted by fractures, congenital abnormalities, schwannomas, glomus tumors, aneurysms, and meningiomas due to its proximity to other structures. Understanding the anatomy and variations of the HC is essential for planning and preventing complications during other microsurgical procedures in this region, such as TCA, STA, and ITA (8-11).
The HC is located beneath the occipital condyle and extends from the posterior cranial fossa toward the nasopharyngeal cavity. In our study, consistent with other studies, the HC was found to be a canal opening into the middle 1/3 of the condyle in 94% of cases and into the anterior 1/3 of the condyle in 88% of cases. In the study by Kalthur et al., the external opening of the canal was found to be anterior in 99% of males and 93% of females, while the internal opening was located in the middle 1/3 of the condyle in both males and females.7 Similarly, Naderi et al., in their study on the Turkish population, classified the internal and external openings by dividing the condyle into seven parts.8 As a result, the internal opening was mostly detected in locations 3 (12%), 4 (56.8%), and 5 (25.8%) on the right, corresponding to the middle 1/3 of the condyle, and in locations 3 (19.2%), 4 (55.8%), and 5 (15.7%) on the left. The external opening was observed in locations 1 (77.1%), 2 (20.3%) on the right, corresponding to the anterior 1/3, and in locations 1 (50.7%) and 2 (40.1%) on the left.
Verma et al., in their study on 100 skulls, did not classify the location of the internal and external openings of the HC separately.9 They observed that the canal was located anteriorly in 85% of the cases.
The HC may be partially or completely separated into two parts by a bony septum. This supports the notion that the occipital base is formed by the fusion of three or four vertebrae, and the HC by the fusion of intervertebral foramina.10 Bergman et al. thought the HC separation was a sign of an occipital vertebra fusing around the FM.11 In the fetal study by Dodo et al., the earliest finding of a bony septum in the HC at 28 weeks may reflect genetic rather than physical septation.12 Right- left differences may indicate the effectiveness of epigenetics. The septum or notch has been reported to be located between the two bundles of the hypoglossal nerve or along the dural septum of the venous plexus.13 Kalthur et al. stated that the septum extends between the ascending pharyngeal artery and the nerve.7
When the canal was divided into two groups according to the presence of a septum (Type 1, 2, 3 = absence and Type 4, 5 = presence), it was observed that there was no septum in 72.8% of the 118 canals examined by Kızılkanat et al., in 82% of the 100 canals in the study of Ari, in 83.7% of the 110 canals examined in men by Kalthur et al., in 79.45% of the 232 canals in the study of Paraskevas et al., and in 76.4% of the 282 canals in the study of Lyrtzis et al..7,14,15,16,17 In our study, there was no septum in 76.6% of the 64 canals. HC was classified into five types based on its septum and notch.10 In their study on male skulls, Kalthur et al. found Type 1 at 43.6%, Type 2 at 36.3%, Type 3 at 3.6%, and Type 4 at 16.3%.7 Similar to our study, Type 1 canal was the most common, while Type 3 was the least common. In contrast, they found Type 2 canal to be the second most common type. Ari et al. found Type 2 as the most common (42%), Type 1 as the second most common (38%), and Type 3 as the least common (2%).15 Similar to the literature, Paraskevas et al. found Type 1 to be 59.49%, Type 2 to be 18.10%, Type 3 to be 0.86%, Type 4 to be 19.83%, and Type 5 to be 1.72% in 232 canals, respectively. In our study, similar to the studies by Ari et al. and Kalthur et al., we found that Type 1 was more prevalent on the right side and Type 4 was more prevalent on the left side compared to the other side.7,15,16
The mean length of the HC was recorded with only one parameter in previous studies. Kalthur et al. found it as 9±0.18 mm, Kızılkanat et al. as 9.9±1.9 mm, Hadley and Shelton as 11.2±1.52 mm, Berlis et al. as 7.78 mm, Shimaa et al. as 11.84±2.56 mm (R), 11.8±2.4 mm (L). Lyrtzis et al. found the length of the right canal as 8.89±1.50 mm and the length of the left canal as 9.03±1.53 mm.6,7,17,18,19 Also, contrary to previous studies and our study, they found a significant difference between the right and left. The most different results were found by Karasu et al., who measured the longest axis of the canal as 21±1.29 mm.20 In our study, similar to the studies conducted by Katsuta et al. and Paraskevas et al., anterior and posterior wall lengths were measured separately.13,16 Since a statistically significant difference was observed between HCAL and HCPL, we suggest that evaluating canal length using two parameters provides a more accurate assessment. Unlike other studies, to obtain more detailed data, we measured AL, PL, IHC, HCIW, HCEH, and HCEW separately in the main and accessory canals of Types 4 and 5 (Table 3).
Paraskevas et al. reported mean values for HCs without septum (Types 1, 2, 3) as follows: HCAL, 8.93 ± 1.74 mm; HCPL, 10.22 ± 1.81 mm; HCIH, 4.42 ± 0.93 mm; HCIW, 7.44 ± 1.4 mm; HCEH, 3.91 ± 1.12 mm; and HCEW, 6.15 ± 1.32 mm. Similarly, Katsuta et al. measured HCAL as 7.3 ± 1.3 mm, HCPL as 10.6 ± 1.5 mm, HCIH as 4.2 ± 0.7 mm, HCIW as 7.1 ± 1.1 mm, HCEH as 4.4 ± 0.8 mm, and HCEW as 5.9 ± 0.9 mm.13,16 In our study, HCAL and HCPL were found to be smaller, whereas HCIH, HCIW, HCEH, and HCEW were consistent with the values reported in previous studies (Table 1 and Table 2).
In previous studies, HCIB and HCIO were found to be 16.2±1.5 mm (m) and 15.7±1.5 mm (f), and 30.7±2.7 mm (M) and 30.8±2.5 mm (F), similar to our study.7 Kızılkanat et al. found these measurements to be 16.4±1.6 mm vs. 29.1±2.4 mm in their study.18
The similarities and differences may be due to measurement techniques, race, age, clinical conditions, and gender.
Limitations
The sample size was smaller compared to previous studies; additionally, information regarding age, sex, and clinical conditions was unknown.
Conclusion
The findings obtained in our study, supported by morphometric measurements, are consistent with those reported in the literature. A thorough understanding of the variation and morphometry of the anatomical features of the skull base is crucial for accurate diagnosis and treatment, and is a fundamental anatomical component of surgery. Our study, focusing on morphological features, will be beneficial to clinical fields such as neurosurgery and neurology.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
This study did not involve human participants or animals.
Informed Consent
Informed consent was not required because the study was performed on dry skull specimens.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: M.C.T., Z.F.
Methodology: M.C.T., A.S.A.
Investigation: M.C.T., A.S.A., E.S.
Data curation: M.C.T.
Formal analysis: M.C.T., E.S.
Writing – original draft: M.C.T.
Writing – review & editing: Z.F., E.S.
Supervision: Z.F.
Abbreviations
AC: Accessory canal
ACAL: Anterior wall length of the accessory canal
ACEH: Height of the external opening of the accessory canal
ACEW: Width of the external opening of the accessory canal
ACIH: Height of the internal opening of the accessory canal
ACIW: Width of the internal opening of the accessory canal
ACPL: Posterior wall length of the accessory canal
FM: Foramen magnum
HC: Hypoglossal canal
HCAL: Anterior wall length of the hypoglossal canal
HCEH: Height of the external opening of the hypoglossal canal
HCEW: Width of the external opening of the hypoglossal canal
HCIH: Height of the internal opening of the hypoglossal canal
HCIB: Distance of the internal opening of the hypoglossal canal to the basion
HCIO: Distance of the internal opening of the hypoglossal canal to the opisthion
HCIW: Width of the internal opening of the hypoglossal canal
HCPL: Posterior wall length of the hypoglossal canal
ICC: Intraclass correlation coefficient
ITA: Infratemporal approach
STA: Suboccipital subtonsillar approach
TCA: Transcondylar approach
References
-
Waschke J, Böckers TM, Paulsen F, editors. Sobotta’s anatomy textbook. Elsevier Health Sciences; 2015:414-423.
-
Standring S, editor. Gray’s anatomy: the anatomical basis of clinical practice. Churchill Livingstone; 2008:409-434.
-
More R, Singh R, Shende N, Pandey S. Bilateral internal triplication of hypoglossal canal. Int J Health Sci Res. 2015;5(7):445-447.
-
Nayak SB. Unilateral, double hypoglossal nerves leaving the cranial cavity through two hypoglossal foramina: a case report. Neuroanatomy. 2008;7(1):6-7.
-
Kay RF, Cartmill M, Balow M. The hypoglossal canal and the origin of human vocal behavior. Proc Natl Acad Sci U S A. 1998;95(9):5417-5419. doi:10.1073/pnas.95.9.5417
-
Hadley KS, Shelton C. Infratemporal fossa approach to the hypoglossal canal: practical landmarks for elusive anatomy. Laryngoscope. 2004;114(9):1648-1651. doi:10.1097/00005537-200409000-00027
-
Kalthur SG, Padmashali S, Bhattarai C, Gupta C. Surgical anatomy of hypoglossal canal for various skull base surgeries. Surg Radiol Anat. 2023;45(5):537-543. doi:10.1007/s00276-023-03126-7
-
Naderi S, Korman E, Çıtak G, et al. Morphometric analysis of human occipital condyle. Clin Neurol Neurosurg. 2005;107(3):191-199. doi:10.1016/j.clineuro.2004.07.014
-
Verma R, Kumar S, Rai AM, Mansoor I, Mehra RD. The anatomical perspective of human occipital condyle in relation to the hypoglossal canal, condylar canal, and jugular foramen and its surgical significance. J Craniovertebr Junction Spine. 2016;7(4):243-249. doi:10.4103/0974-8237.193258
-
Hauser G, De Stefano GF. Variations in form of the hypoglossal canal. Am J Phys Anthropol. 1985;67(1):7-11. doi:10.1002/ajpa.1330670103
-
Bergman RA, Afifi AK, Miyauchi R. Illustrated encyclopedia of human anatomic variation. Opus V: skeletal systems: cranium. Published 1996. Accessed September 29, 2025. Available from: https://www.anatomyatlases.org/AnatomicVariants/SkeletalSystem/Text/Cranium.shtml
-
Dodo Y. Appearance of bony bridging of the hypoglossal canal during the fetal period. Anthropol Sci. 1980;88(3):229-238. doi:10.1537/ase1911.88.229
-
Katsuta T, Matsushima T, Wen HT, Rhoton AL Jr. Trajectory of the hypoglossal nerve in the hypoglossal canal: significance for the transcondylar approach. Neurol Med Chir (Tokyo). 2000;40(4):206-209. doi:10.2176/nmc.40.206
-
Kizilkanat E, Boyan N, Soames R, Oğuz Ö. Morphometry of the hypoglossal canal, occipital condyle, and foramen magnum. Neurosurg Q. 2006;16(3):121-125. doi:10.1097/01.wnq.0000214018.49915.49
-
Ari I, Kurt MA, Oygucu IH, Sendemir E. Variations in the bridging trait of the hypoglossal canal in 13th century Byzantine skulls. Int J Osteoarchaeol. 2005;15(2):140-145. doi:10.1002/oa.738
-
Paraskevas GK, Tsitsopoulos PP, Papaziogas B, et al. Osseous variations of the hypoglossal canal area. Med Sci Monit. 2009;15(3):BR75-BR83.
-
Lyrtzis C, Piagkou M, Gkioka A, et al. Foramen magnum, occipital condyles and hypoglossal canals morphometry: anatomical study with clinical implications. Folia Morphol (Warsz). 2017;76(3):446-457. doi:10.5603/fm.a2017.0002
-
Berlis A, Putz R, Schumacher M. Direct and CT measurements of canals and foramina of the skull base. Br J Radiol. 1992;65(776):653-661. doi:10.1259/0007-1285-65-776-653
-
Farid SA, Fattah IOA. Morphometric study of human adult occipital condyle, hypoglossal canal foramen magnum in dry skull of modern Egyptians. Int J Clin Dev Anat. 2018;4(1):19-26.
-
Karasu A, Cansever T, Batay F, Sabanci PA, Al-Mefty O. The microsurgical anatomy of the hypoglossal canal. Surg Radiol Anat. 2009;31(5):363-367. doi:10.1007/s00276-008-0455-x
Figures
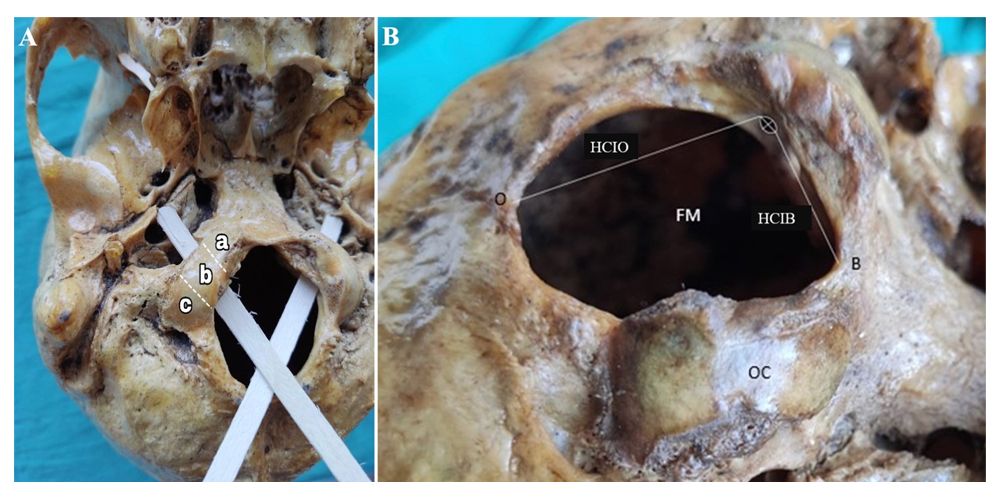
Figure 1. A. Location of the internal and external openings of the hypoglossal canal (HC). a: Anterior 1/3, b: Middle 1/3, c: Posterior 1/3. Wooden stick: course of HC. B. OC: Occipital condyle, O: Opisthion, B: Basion, FM: Foramen magnum, Lines within HC: HCIW: The width of the internal opening (anterior- posterior border) of the HC, HCIH: The height of the internal opening (upper-lower border) of the HC. Dashed white line: HCIB: Distance of the internal opening of the HC to the B, HCIO: Distance of the internal opening of the HC to the O
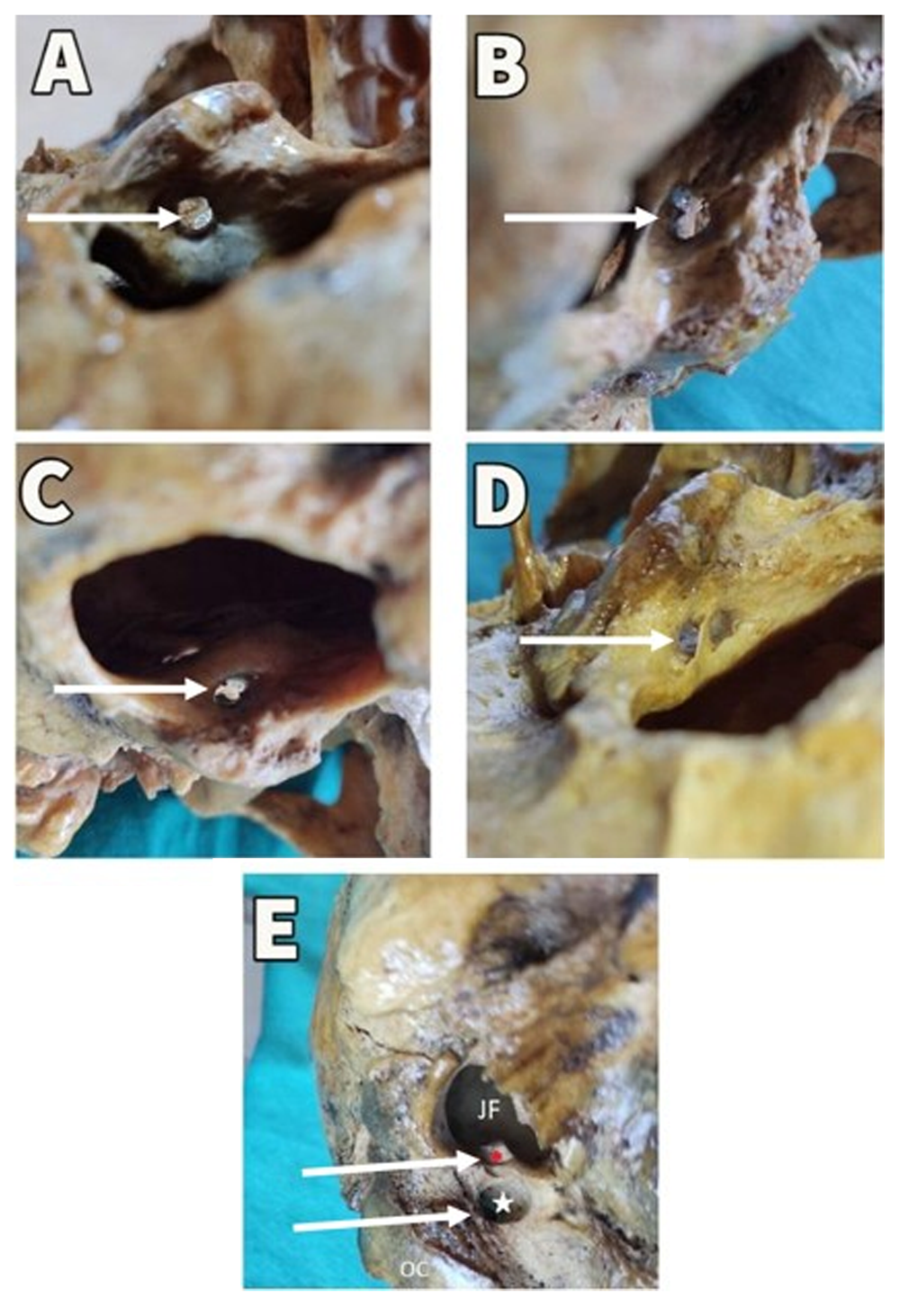
Figure 2. Hypoglossal canal (HC) types. A: Type 1 simple straight canal, B: Type 2 single bony process, C: Type 3 two bony processes, D: Type 4 inner opening divided into two by a bony septum, external opening still single, E: Type 5, septum along the canal and double, white star and red star HC have two separate external openings. (JF: Jugular foramen, OC: Occipital condyle)
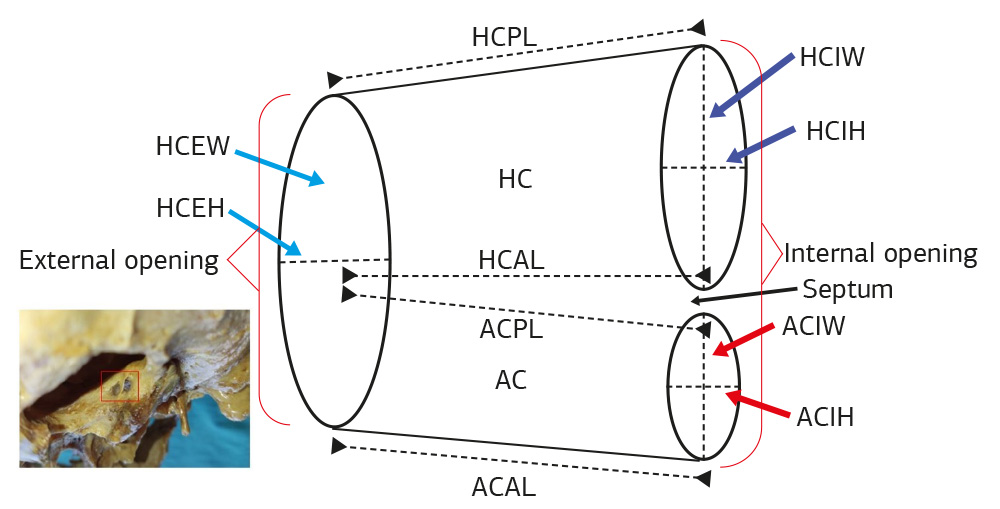
Figure 3. Type 4 hypoglossal canal (HC), accessory canal (AC). Dotted and arrowed lines: HCAL: anterior wall length of the HC, HCPL: posterior wall length of the HC, ACAL: Anterior wall length of the AC, ACPL: Posterior wall length of the AC. Dashed lines: HCIW: Width of the internal opening (anterior-posterior border) of the HC, HCIH: Height of the internal opening (upper- lower border) of the HC, HCEW: Width of the external opening of the HC, HCEH: Height of the external opening of the HC. ACIW: Width of the internal opening of the AC, ACIH: Height of the internal opening of the AC
Tables
Table 1. Measurements of the hypoglossal canal (mm)
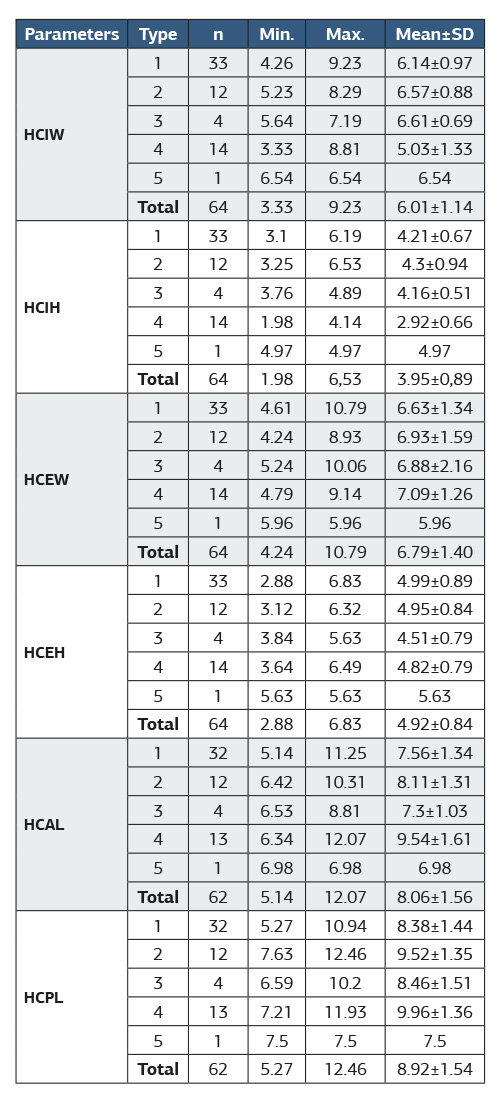
HCIW: Width of the internal opening (anterior-posterior border) of the hypoglossal canal (HC), HCIH: Height of the internal opening (upper-lower border) of the HC, HCEW: Width of the external opening of the HC, HCEH: Height of the external opening of the HC, HCAL: Anterior wall length of the HC, HCPL: Posterior wall length of the HC
Table 2. Measurements according to hypoglossal canal types (mm)
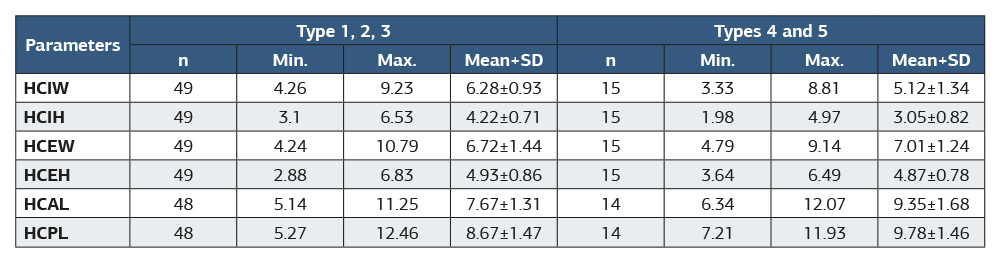
HCIW: Width of the internal opening (anterior-posterior border) of the hypoglossal canal (HC), HCIH: Height of the internal opening (upper-lower border) of the HC, HCEW: Width of the external opening of the HC, HCEH: Height of the external opening of the HC, HCAL: Anterior wall length of the HC, HCPL: Posterior wall length of the HC
Table 3. Measurements of the accessory canal of types 4 and 5 (mm)
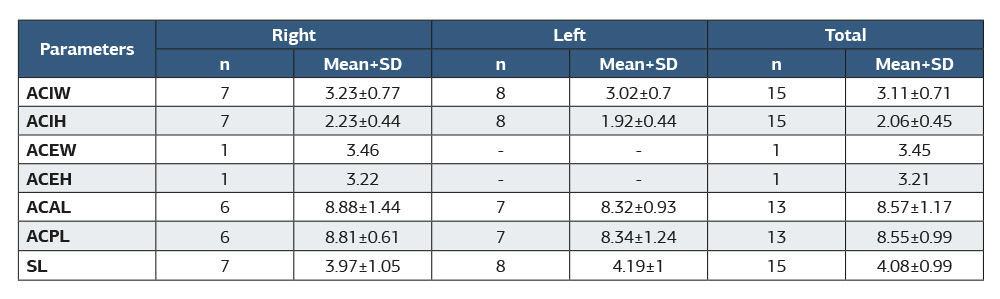
ACIW: Width of the internal opening of the accessory canal (AC), ACIH: Height of the internal opening of the AC, ACEW: Width of the external opening of the AC, ACEH: Height of the external opening of the AC, ACAL: Anterior wall length of the AC, ACPL: Posterior wall length of the AC, SL: Septum length
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mehmet Cengiz Tatar, Ahmet Selim Aygündüz, Ekrem Solmaz, Zeliha Fazliogullari. Anatomical analysis of the hypoglossal canal in dry skulls. Ann Clin Anal Med 2026;17(6):527-532. doi:10.4328/ACAM.22918
- Received:
- September 29, 2025
- Accepted:
- November 3, 2025
- Published Online:
- November 18, 2025
- Printed:
- June 1, 2026