
Conversion to open surgery in laparoscopic cholecystectomy: long term retrospective outcomes
Conversion in laparoscopic cholecystectomy
Authors
Abstract
Aim Laparoscopic cholecystectomy (LC) is considered the gold standard in the surgical treatment of gallbladder diseases. However, conversion to open surgery may be necessary in certain situations. This study aims to retrospectively evaluate cases converted to open surgery among LC procedures performed at our center over 13 years.
Methods Adult patients who were scheduled for LC but required conversion to open cholecystectomy during surgery between January 1, 2008, and January 1, 2021, were included. Demographic data, clinical features, laboratory findings, reasons for conversion, and postoperative outcomes were analyzed.
Results Out of 9580 LC cases, 49 patients (0.5%) required conversion to open surgery. The most common reason for conversion was dense adhesions in Calot’s triangle (77.6%), followed by organ injury (14.3%). A history of previous abdominal surgery was significantly more common in patients with adhesions (p < 0.001), while a history of cholecystostomy was more frequent in those converted due to severe inflammation (p = 0.016). Patients with organ injuries had significantly lower hemoglobin levels (p = 0.006) and a higher rate of reoperation (p = 0.01).
Conclusion In our study, the rate of conversion from LC to open surgery was notably lower than rates reported in the literature. Advanced age, male gender, dense adhesions, and prior abdominal surgery were identified as major risk factors for conversion. Proper patient selection, surgical experience, and appropriate technical approaches can reduce conversion rates. In cases of anatomical difficulty or high complication risk, early conversion or alternative surgical strategies, such as partial cholecystectomy, should be considered.
Keywords
Introduction
Laparoscopic cholecystectomy (LC) is widely accepted as the “gold standard” in the surgical management of gallstone disease.1 Compared with open cholecystectomy, LC results in reduced postoperative pain, improved cosmetic outcomes, and shorter hospital stays.2 Contraindications to LC are primarily related to anesthesia considerations: hemodynamic instability, uncontrolled bleeding disorders, and diffuse peritonitis.3 Suspected gallbladder carcinoma mandates open cholecystectomy.4 Depending on the surgeon’s experience, previous abdominal operations, pregnancy, obesity, cholangitis, and significant comorbidities may also warrant open approaches.5 Major complications such as vascular injury, bowel perforation, mesenteric damage, and bile duct injury frequently necessitate emergency laparotomy. Previous studies report conversion rates from LC to open surgery ranging from 0.5% to 15%; a high rate should not be interpreted as a sign of surgeon failure.6,7,8 Indications for conversion include:9
- hemorrhage,
- unidentifiable or abnormal anatomy,
- inability to proceed laparoscopically in a timely manner,
- bowel or bile duct injury,
- resectable gallbladder cancer,
- bile duct stones not removable by laparoscopic or endoscopic means (e.g., Billroth II anatomy, prior failed ERCP, or lack of experienced endoscopist)
Partial cholecystectomy in laparoscopic cases may reduce the likelihood of conversion to open surgery.10 However, the risk of postoperative complications such as bilioma or abscess is higher with partial cholecystectomy compared to standard cholecystectomy.11 Laparoscopic cholecystectomy provides numerous significant advantages for patients, surgeons, and healthcare costs.12 Therefore, performing this surgical procedure laparoscopically whenever possible is a primary goal for both surgeons and patients. For this reason, analyzing the causes of conversion is of great importance. Although many previous studies have investigated the reasons for conversion from laparoscopic to open cholecystectomy,6 a considerable number of conversions still occur. This indicates a continuing need for further research in this area. The aim of this study is to retrospectively evaluate all laparoscopic cholecystectomy cases performed in our center to determine the conversion rate, identify the cases in which conversion occurred, and analyze the reasons behind these conversions.
Materials and Methods
This study included adult patients who were scheduled for laparoscopic cholecystectomy between January 1, 2008, and January 1, 2021, but required conversion to open cholecystectomy during the procedure. Inclusion criteria: Patients over 18 years of age who underwent laparoscopic cholecystectomy that was subsequently converted to open surgery. Exclusion criteria: Patients under 18 years of age, cases that were initiated as open cholecystectomy from the beginning, and cases where laparoscopic cholecystectomy was completed without conversion. For patients who underwent conversion, the following data were recorded: age, sex, comorbidities, history of ERCP, presence of cholecystostomy, laboratory parameters (including blood glucose, WBC count, hemoglobin, total bilirubin, ALT, AST, ALP), reasons for conversion, surgical indications, history of previous abdominal surgery, duration of symptoms, radiological findings, intraoperative and postoperative complications, ICU stay duration, pathological results, and mortality. Patients were categorized into subgroups based on the reason for conversion: dense adhesions in Calot’s triangle, severe inflammation, adhesions due to previous surgeries, organ injury, and anatomical variations. These subgroups were then compared based on the aforementioned parameters to complete the study.
Ethical ApprovalThis study was approved by the Ethics Committee of the University of Health Sciences, Hamidiye Scientific Research Ethics Committee (Date: 2021-03-31, No: 23694).
Statistical AnalysisFirst, Kolmogorov-Smirnov and Shapiro-Wilk tests were used to assess the normality of the variables. Non-parametric methods were used for non-normally distributed variables. Subsequently, the Mann–Whitney U test was used to compare the variables obtained from the measurements between groups. Chi-square and Fisher’s exact tests were used to analyze the relationships or differences between groups regarding categorical variables. Multiple group comparisons were conducted using ANOVA analysis. Bonferroni and Tamhane-T2 tests were applied depending on whether the variances were homogeneous. Comparative results between groups based on demographic characteristics were presented as the ratio of qualitative variables. Quantitative variables were expressed as mean and standard deviation. Statistical Package for Social Sciences (SPSS), version 22.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. p-value <0.05 was considered significant.
Reporting GuidelinesThis study was designed and reported in accordance with the STROBE guidelines for observational studies.
Results
In this study, a retrospective analysis was performed on 49 cases converted to open surgery out of 9,580 patients who underwent laparoscopic cholecystectomy at our center between January 1, 2008, and January 1, 2021. The conversion rate in our clinic was found to be 0.5%.Thirty-eight patients (77.6%) underwent conversion to open surgery for this reason. The second most common reason was organ injury in 7 patients (14.3%). Other causes included adhesions from previous surgery (4.1%), severe inflammation (2%), and anatomic variations (2%).Of the 49 patients, 28 were male and 21 were female, with a mean age of 64.1 years. The majority of patients belonged to the ASA II risk group (55.1%). The most frequent indication for cholecystectomy was cholelithiasis (57.1%). A history of ERCP was present in 5 patients, prior abdominal surgery in 4 patients, and cholecystostomy in 4 patients (Table 1).When comparing subgroups based on reasons for conversion, no statistically significant differences were observed in terms of age, gender, ASA scores, surgical indication, or ERCP history. However, patients who were converted due to dense adhesions were significantly more likely to have a history of previous abdominal surgery (p < 0.001). Similarly, patients converted due to severe inflammation were more likely to have a history of cholecystostomy (p = 0.016) (Table 1). Ultrasonographic and laboratory findings were also compared among groups.
Hemoglobin levels were significantly lower in the group converted due to organ injury (p = 0.006). No significant differences were found in other parameters (Table 2). There were no statistically significant differences among groups regarding ICU stay, need for postoperative ERCP, or pathology results. However, the reoperation rate was significantly higher in the group converted due to organ injury (p = 0.01) (Table 3).
Discussion
According to the literature, the conversion rate from laparoscopic to open cholecystectomy ranges between 0.5% and 15%, with an average of approximately 6%.5,13 In our study, which included 9,580 patients at our clinic, the conversion rate was found to be significantly lower than the reported average, at 0.5%.Advanced age and male sex are known risk factors for conversion.14 In line with the literature, the mean age of patients in our study was 64 years, and 57% were male. Other identified risk factors for conversion include a history of acute cholecystitis, diabetes, and obesity. Among our patients, the most common indication for cholecystectomy was cholelithiasis (57%), followed by acute cholecystitis (30%) and choledocholithiasis (8%). However, since our study focused solely on converted cases, we could not establish a statistically significant relationship between acute cholecystitis and conversion. A comprehensive comparison with non-converted cholecystitis patients would be required to evaluate this. No significant association was found between ASA scores (used by anesthesiologists to evaluate comorbidities) and conversion. A history of ERCP was present in 10% of patients, but this was not statistically significant, suggesting that a prior ERCP does not pose a risk factor for conversion. Therefore, laparoscopic cholecystectomy can be safely performed in patients with a history of ERCP. In 78% of cases, the reason for conversion was dense adhesions in Calot’s triangle. Organ injury accounted for 14% of conversions. In accordance with the literature, we found that a history of previous abdominal surgery was significantly associated with conversions due to dense adhesions. Prior surgeries are likely to increase the presence of intra-abdominal adhesions, which impair visibility during laparoscopy, prolong the procedure, and consequently raise the likelihood of conversion. Similarly, the presence of a cholecystostomy catheter, often placed in critically ill patients or those with severe inflammation, was found to significantly correlate with conversions due to intense inflammation in our study. Cholecystostomy contributes to fibrosis and adhesions around the gallbladder, increasing the difficulty of laparoscopic dissection and raising the likelihood of conversion.15
Hemoglobin levels were significantly lower in patients who were converted due to organ injury. This anemia may reflect underlying chronic inflammation.16 Additionally, patients with preoperative anemia may be more adversely affected by intraoperative bleeding, especially from the liver bed. Delayed bleeding control may increase the risk of conversion to open surgery. Organ injury was also identified as a significant risk factor for reoperation. The most critical injuries during cholecystectomy involve the duodenum and common bile duct. In patients where the gallbladder is densely adherent and fibrotic to surrounding structures like the duodenum, partial cholecystectomy may be a safer alternative to conversion.10 In cases of postoperative bile leakage due to bile duct injury, if no signs of acute abdomen are present, ERCP may be considered before surgical reintervention.
Limitations
This study has some limitations. First, its retrospective and single-center design restricts the generalizability of the findings. Second, as only converted cases were analyzed, risk factors could not be compared with those of non-converted patients. Additionally, the small sample size in some subgroups may have reduced the statistical power. Finally, long-term outcomes were not assessed, limiting insight into the extended impact of conversion.
Conclusion
In this study conducted at our clinic, the evaluation of laparoscopic cholecystectomy cases revealed a conversion rate significantly lower than that reported in the literature. The most prominent risk factors for conversion to open surgery were advanced age, male gender, dense adhesions in Calot’s triangle, and a history of previous abdominal surgery. Organ injuries, while less frequent, require particular attention due to their association with both conversion and increased postoperative morbidity. Proper patient selection, surgical experience, and the application of appropriate technical strategies during laparoscopic cholecystectomy are essential in minimizing complications and reducing the likelihood of conversion to open surgery. When anatomical difficulties are encountered, an early decision to convert to open surgery should be considered, and alternative methods such as partial cholecystectomy may also be evaluated if necessary.
Declarations
Ethics Declarations
This research was conducted in accordance with internationally accepted ethical principles and standards for clinical research. All procedures adhered to institutional and national ethical requirements and were consistent with the principles outlined in the Declaration of Helsinki.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: Y.A.B.
Methodology: Y.A.B., M.E.U.
Formal Analysis: Y.A.B.
Investigation: Y.A.B., İ.H.
Data Curation: M.E.U.
Writing – Original Draft Preparation: Y.A.B.
Writing – Review & Editing: M.E.U., İ.H.
Supervision: İ.H.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
ALP: Alkaline Phosphatase
ALT: Alanine Aminotransferase
ANOVA: Analysis of Variance
ASA: American Society of Anesthesiologists
AST: Aspartate Aminotransferase
CT: Computed Tomography
ERCP: Endoscopic Retrograde Cholangiopancreatography
ICU: Intensive Care Unit
LC: Laparoscopic Cholecystectomy
SPSS: Statistical Package for the Social Sciences
WBC: White Blood Cell
References
-
Mallappa S, Soobrah R. Laparoscopic cholecystectomy: Evaluation of web- based information. Cureus. 2022;14(1):E20897.
-
Johansson M, Thune A, Nelvin L, Stiernstam M, Westman B, Lundell L. Randomized clinical trial of open versus laparoscopic cholecystectomy in the treatment of acute cholecystitis. Br J Surg. 2005;92(1):44-49.
-
Keus F, Broeders IAMJ, van Laarhoven CJHM. Gallstone disease: Surgical aspects of symptomatic cholecystolithiasis and acute cholecystitis. Best Pract Res Clin Gastroenterol. 2006;20(6):1031-1051.
-
Steinert R, Nestler G, Sagynaliev E, Müller J, Lippert H, Reymond MA. Laparoscopic cholecystectomy and gallbladder cancer. J Surg Oncol. 2006;93(8):682-689.
-
Magnano San Lio R, Barchitta M, Maugeri A, Quartarone S, Basile G, Agodi A. Preoperative risk factors for conversion from laparoscopic to open cholecystectomy: A systematic review and meta-analysis. Int J Environ Res Public Health. 2023;20(1):408.
-
Coffin SJ, Wrenn SM, Callas PW, Abu-Jaish W. Three decades later: investigating the rate of and risks for conversion from laparoscopic to open cholecystectomy. Surg Endosc. 2018;32(2):923-929.
-
Shiun A, Hu Y, Menon R, Gunnarsson R, De Costa A. Risk factors for conversion of laparoscopic cholecystectomy to open surgery - A systematic literature review of 30 studies. Am J Surg. 2017;214(5):920-930.
-
Nassar AHM, Zanati H El, Ng HJ, Khan KS, Wood C. Open conversion in laparoscopic cholecystectomy and bile duct exploration: Subspecialisation safely reduces the conversion rates. Surg Endosc. 2022;36(1):550-558.
-
Warchałowski Ł, Łuszczki E, Bartosiewicz A, et al. The analysis of risk factors in the conversion from laparoscopic to open cholecystectomy. Int J Environ Res Public Health. 2020;17(20):1-12.
-
Sabour AF, Matsushima K, Love BE, et al. Nationwide trends in the use of subtotal cholecystectomy for acute cholecystitis. Surg (United States). 2020;167(3):569-574.
-
Xu Y, Yen D, Whitehead M, Xu J, Johnson AP. Safe laparoscopic subtotal cholecystectomy in the face of severe inflammation in the cystohepatic triangle: A retrospective review and proposed management strategy for the difficult gallbladder. Can J Surg. 2019;62(6):393-401.
-
Coccolini F, Catena F, Pisano M, et al. Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int J Surg. 2015;18:196-204.
-
Chin X, Mallika Arachchige S, Orbell-Smith J, Wysocki AP. Preoperative and intraoperative risk factors for conversion of laparoscopic cholecystectomy to open cholecystectomy: A systematic review of 30 studies. Cureus. 2023;15(10): E47774.
-
Kara Y, Kalayci MU. Laparoscopic to open cholecystectomy: The risk factors and the reasons; A retrospective analysis of 1950 cases of a single tertiary center. Surg Laparosc Endosc Percutaneous Tech. 2020;30(2):192-195.
-
Bickel A, Hoffman RS, Loberant N, Weiss M, Eitan A. Timing of percutaneous cholecystostomy affects conversion rate of delayed laparoscopic cholecystectomy for severe acute cholecystitis. Surg Endosc. 2016;30(3):1028-1033.
-
Theurl I, Aigner E, Theurl M, et al. Regulation of iron homeostasis in anemia of chronic disease and iron deficiency anemia: Diagnostic and therapeutic implications. Blood. 2009;113(21):5277-5286.
Tables
Table 1. Comparison of demographic and medical histories of patient groups
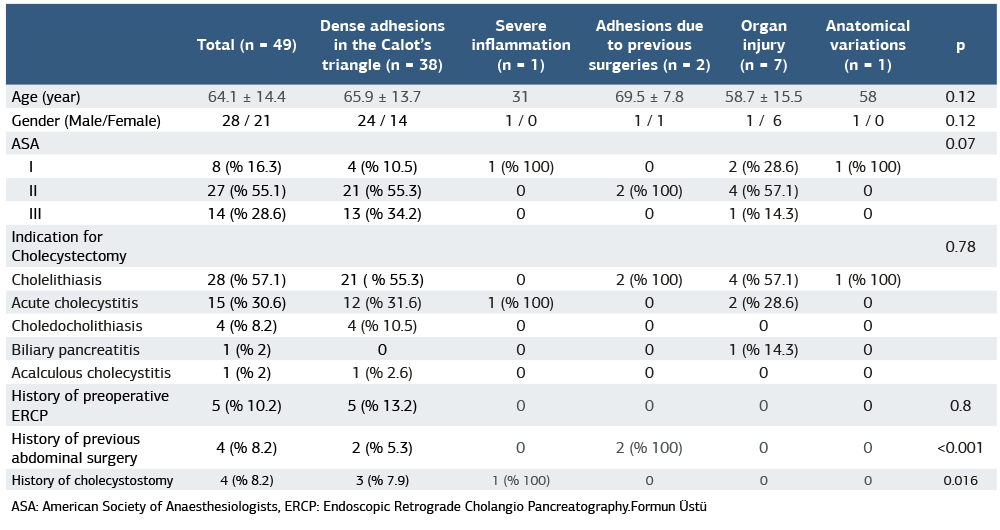
ASA: American Society of Anaesthesiologists, ERCP: Endoscopic Retrograde Cholangio Pancreatography.
Table 2. Comparison of preoperative ultrasonographic and laboratory findings between patient groups
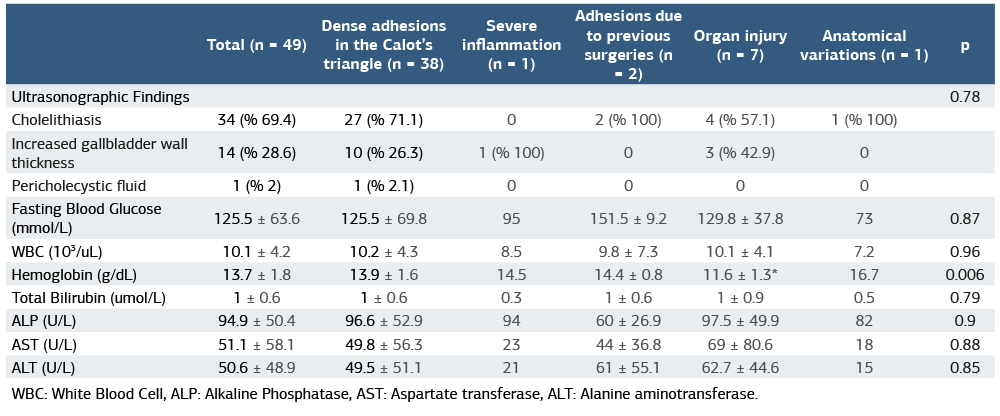
WBC: White Blood Cell, ALP: Alkaline Phosphatase, AST: Aspartate transferase, ALT: Alanine aminotransferase.
Table 3. Comparison of postoperative clinical features and pathology results among patient groups
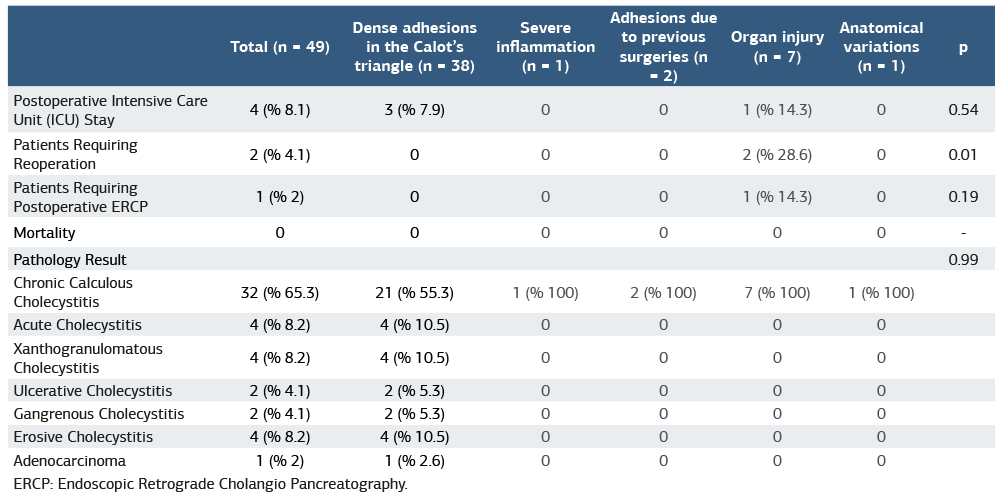
ERCP: Endoscopic Retrograde Cholangio Pancreatography.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yahya Alperen Bayraktar, Mehmet Eşref Ulutaş, İsmail Hasırcı. Conversion to open surgery in laparoscopic cholecystectomy: long term retrospective outcomes. Ann Clin Anal Med 2026;17(4):373-377. DOI: 10.4328/ACAM.22810
- Received:
- July 12, 2025
- Accepted:
- August 19, 2025
- Published Online:
- August 27, 2025
- Printed:
- April 1, 2026