
Abstract
Aim We aimed to determine whether the percentage of pneumothorax affects right ventricular function.Methods This study was conducted between January 1, 2022, and November 1, 2022. A group of 45 patients who applied to our emergency department and were diagnosed with pneumothorax was defined as the study group. A control group was formed of healthy people with a similar gender and age distribution as well as that number of patients. Pneumothorax volume was measured from the thorax computed tomography of the patients, and their echocardiographic evaluations were performed.Results The patients’ mean age was 31.8 ± 8.6 years, and 87 (95.6%) of them were male. In our patient group, basal diameter of right ventricle, mid diameter of right ventricle, right ventricular end systolic area, right ventricular isovolumetric relaxation time, right ventricular isovolumetric contraction time, tricuspid regurgitation velocity, and the inferior vena cava’s diameter (respectively p<0.001, p<0.001, p=0.007, p<0.001, p<0.001, p<0.001, p=0.005) values were high, right ventricular fractional area change and right ventricular rate of pressure change (dP/dT) during isovolumetric contraction values were lower compared with the control group (p<0.001, p<0.001, respectively).Conclusion Pneumothorax affects right ventricular function. Therefore, patients may need cardiological follow-up during and after admission.
Keywords
Introduction
Pneumothorax occurs when air accumulates between the layers of the visceral pleura and the parietal pleura, resulting from various causes. Although pleural air can have multiple origins, the most common cause is the rupture of the visceral pleura, leading to air leakage into the pleural space from the lung parenchyma. Under normal conditions, the parietal and visceral pleura function harmoniously. The pressure in the pleural space (the space between the parietal and visceral pleura) is typically 5 mmHg. During inspiration, this pressure increases to 6–8 mmHg, thus facilitating expiration. When the normal negative pressure in the pleural space disappears, the affected lung collapses. Primary spontaneous pneumothorax involves the accumulation of intrapleural air in patients without trauma or pre-existing lung disease, both clinically and radiologically.1,2,3,4 Secondary spontaneous pneumothorax may occur due to underlying lung diseases or the effect of systemic conditions. Chronic obstructive pulmonary disease (COPD) is a well known cause of secondary spontaneous pneumothorax, while other contributing factors include pulmonary tuberculosis, sarcoidosis, lung malignancies, and cystic fibrosis. Acquired pneumothoraxes can be categorized into three groups: traumatic pneumothorax, barotrauma-induced pneumothorax, and iatrogenic pneumothorax.2,4,5,6
Diagnostic methods for pneumothorax include chest radiography, thoracic computed tomography (CT), and ultrasonography. While the standard technique for stable patients is posteroanterior chest X-ray, its sensitivity is approximately 86%.7 CT is considered the gold standard for diagnosis and estimation of the pneumothorax area, especially as direct X-rays underestimate the actual size due to their two-dimensional nature.8,9,10 CT imaging provides the most accurate calculation of the pneumothorax area.11
Pneumothorax can be progressive and can cause a mediastinal shift and turn into tension pneumothorax, which is a life-threatening emergency. In the presence of tension pneumothorax, patients may experience obstructive shock due to pressure on the cava-atrial junction. Tube thoracostomy has shown dramatic clinical improvement in such cases.
We started this study based on the hypothesis that right ventricular dysfunction and clinical deterioration may be associated with increased intrathoracic pressure in patients with pneumothorax. During our literature review, we found no studies that had investigated the effects of pneumothorax percentage on the right ventricle (RV) in patients with pneumothorax. We thought that the detection of right ventricular dysfunction using echocardiography could be a useful marker for diagnosis and prediction of the clinical course in patients with pneumothorax. In our study, we aimed to determine whether pneumothorax volume affects right ventricular measurements in adult patients diagnosed with pneumothorax by thorax computed tomography in the ED and hospitalized.
Materials and Methods
Study Design and Collection of DataOur study was designed as a prospective cohort. Using the G-Power program with α = 0.05, power (1 − β) = 0.85, a 1:1 case intervention group ratio, and a moderate effect size, it was determined that 45 patients diagnosed with pneumothorax, applying to the Emergency Department (ED), would constitute the study group. A control group, consisting of healthy individuals matched in both number and gender and age distribution, was also formed. Group 1 comprised patients with pneumothorax, while Group 2 comprised healthy individuals. The study commenced on January 1, 2022, after the approval of the ethics committee, and concluded on November 1, 2022, upon reaching the target number of subjects. In total, our study included 90 individuals, with 45 healthy volunteers and 45 diagnosed with pneumothorax, all of whom were admitted to the ED.Inclusion Criteria-Individuals presenting to the ED with a diagnosis of pneumothorax.
-Patients aged 18–65.
-Those who consented to participate in the study and provided informed consent.Exclusion Criteria-Involuntary participants.
-Patients below 18 or above 65 years old.
-Individuals with tension pneumothorax.
-Patients with cardiac comorbidities, including diabetes mellitus, hypertension, malignancy, arrhythmia, cardiomyopathy, chronic heart failure, chronic ischemic heart disease, and asthma/ COPD, patients with multiple trauma, and patients using cardiac medications.Laboratory and Clinical EvaluationIndividuals presenting to the ED with a preliminary diagnosis of pneumothorax were transferred to the critical care unit during their initial admission. Patient files were updated with their dates of birth, gender, and any additional medical conditions. Vital signs during the first admission were systematically recorded through continuous monitoring. Vascular access was established via the antecubital vein. Simultaneously, 10 mL of venous blood was drawn from the patients using a 10-mL syringe. The collected venous blood samples were sent to the central laboratory of our hospital for analysis of hemogram and biochemical parameters. The hemogram results, including hemoglobin value and platelet count, along with lactate dehydrogenase (LDH), glucose, albumin, protein, urea, creatinine, sodium, potassium, alanine aminotransferase (ALT), aspartate aminotransferase (AST), Creatine kinase-Myocardial band (CK-MB), Troponin-I, and B-type natriuretic peptide (BNP) levels, were studied.Computed Tomography Evaluation of the ThoraxThoracic CT images of the patients were obtained without the administration of intravenous contrast agents. Images were acquired using the 128-detector, Multi Detector CT System. The assessment was evaluated by a radiology specialist with at least five years of experience. The tumor tracking method was used in the evaluation.Echocardiographic EvaluationBefore the tube thoracostomy procedure, 2D transthoracic echocardiography and M-mode assessments were conducted on the patients by a cardiologist. Since their vital functions were stable, echocardiographic measurements were made in the Echocardiography Laboratory using the EPIQ 7C (Philips Healthcare, 3000 Minuteman Road, Andover, MA) echocardiography device. All measurements adhered to the guidelines set forth by the European Society of Cardiovascular Imaging and the American Society of Echocardiography.12 The measurements included various parameters of the RV, such as RV basal diameter, RV mid-diameter, RV end-systolic area, RV end-diastolic area, RV fractional area change, RV isovolumetric relaxation time, RV isovolumetric contraction time, RV dP/dT (the rate of pressure change with time during isovolumetric contraction of cardiac ventricles), tricuspid regurgitation velocity, inferior vena cava (IVC) diameter, and changes in IVC measurements with breathing. These echocardiographic measurements were conducted and recorded by a cardiologist with a minimum of 10 years of experience in the cardiology clinic and expertise in echocardiography.Ethical ApprovalThis study was approved by the Ethics Committee of Adana City Training and Research Hospital (Date: 2021-12-30, No: 96/1705).Statistical AnalysisThe SPSS (Statistical Package for the Social Sciences) 25.0 package program was used for statistical analysis. Categorical measurements were presented as percentages and numbers, and continuous measurements were expressed as standard deviation and mean ± standard deviation (median and minimum/maximum where appropriate). While comparing categorical expressions, Fisher’s exact tests and Chi-square tests were used. The Shapiro–Wilk test was utilized to assess normal distribution for study parameters. For parameters not demonstrating normal distribution, the Mann–Whitney U test was used. To explore the relationship between right and left pneumothorax volume values on thorax CT and echocardiographic findings, Spearman’s rho correlation test was used. The statistical significance level for all tests was set at p<0.05.Reporting GuidelinesThis study is reported in accordance with the STROBE guideline.
Results
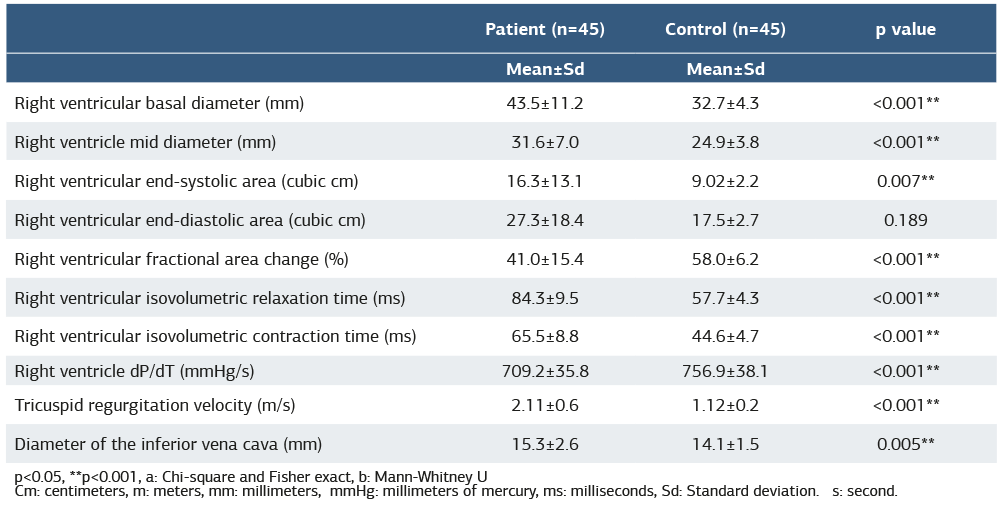
The study comprised 90 patients with a mean age of 31.8 ± 8.6 years, and 87 (95.6%) of the patients were male. In terms of vital signs, the mean values were as follows: fever, 36.6°C ± 0.4; heart rate, 78.9±12.9/minute; systolic blood pressure, 119.9 ± 9.0 mmHg; diastolic blood pressure, 76.5 ± 6.2 mm- Hg; respiratory rate, 14.9±1.9/minute; and oxygen saturation, 97.6 ± 2.7%. It was determined that the heart rate was higher (p<0.001) and the oxygen saturation was lower in the group of patients when compared to the control group (p<0.001). Laboratory findings were found to be similar in the group of patients and the control group (p>0.05) (Table 1). No significant difference was found between the other parameters in Table 2 and the groups (p>0.05). When the side of the pneumothorax was examined on thorax CT, it was right in 15 (33.3%) patients, left in 26 (57.78%) patients, and bilateral in 4 (8.89%) patients. Air densities representing pneumothorax were stained with the tumor tracking method, and volume measurements were calculated (Figure 1). The mean right pneumothorax volume on thorax CT was 722.3 ±1137.9, and the mean left pneumothorax volume on thorax CT was 663.5 ± 1021.2 (Table 2). It was observed that 87 (95.6%) of the patients exhibited an inferior vena cava respiration rate of >50%, while 4 (4.4%) had a rate of <50%. In the patient group, compared to the control group, the RV basal diameter, RV mid-diameter, RV end- systolic area, RV isovolumetric relaxation time, RV isovolumetric contraction time, tricuspid regurgitation velocity, and diameter of the inferior vena cava (p<0.001, p<0.001, p=0.007, p<0.001, p<0.001, p<0.001, p=0.005) values were high; RV fractional area change and RV dP/dT values were found to be lower than the control group (p<0.001, p<0.001, respectively). There was no significant difference between the other parameters and the groups (p>0.05) (Table 3). There was a positive (linear) moderate correlation between the right-side pneumothorax volume on thorax CT and the findings of the right ventricular fractional area change (r=0.458, p=0.049).Discussion
In cardiopulmonary disorders, assessing the RV is crucial within the overall clinical evaluation. Our study, revealing the potential impact of increased intrathoracic pressure on right ventricular function in patients diagnosed with pneumothorax, stands as the first to demonstrate this correlation with pneumothorax volume. CT remains the gold standard for the diagnosis of pneumothorax and for the estimation of the pneumothorax volume.8,11 On the other hand, our findings suggest that echocardiographic follow-ups may be necessary when diagnosing and monitoring pneumothorax patients. In our study, we found that pneumothorax volume affects right ventricular measurements in adult patients diagnosed with pneumothorax. Evaluation of the RV is difficult due to the complex structure of the RV, dense myocardial tissue containing trabeculae, and difficulty in obtaining and evaluating the echocardiographic image due to its location in the retrosternal region, as well as load-dependent evaluation parameters.12,13 The IVC is a large, high-compliance vein that is exposed to pressure in the abdomen and acts as a reservoir. The IVC diameter varies depending on respiration, blood volume, and the functions of the right heart.14,15 The respiratory change of the diameter of the IVC in spontaneously breathing patients has been tried to be explained by a significant decrease in the pressure in the pleural space during inspiration, followed by a decrease in right heart pressures and an increase in intra-abdominal pressure.16 Kircher et al. demonstrated that the decrease in the IVC diameter at the end of inspiration and the pressure of the right atrium were correlated in spontaneously breathing individuals using the distensibility index.17 In our study, it was seen that 87 (95.6%) of the patients had an IVC change with respiration >50%, and 4 (4.4%) had <50% IVC change.
RV diameter measurements are a valuable parameter that quantitatively reveals ventricular dilatation. In the apical four- chamber view, the measurement should be taken at the most distended point. A finding above 41 mm in basal diameter and over 35 mm in mid-diameter indicates the presence of dilatation.18 In the study of Özsu et al., which aimed to show the prognostic role of right ventricular dysfunction and biomarkers in pulmonary embolism, the mean diameter of the RV was found to be 32 mm in both living and dead patients.19 In our study, in the group of patients compared to the control group, the RV basal diameter, RV mid-diameter, RV end- systolic area, RV isovolumetric relaxation time, RV isovolumetric contraction time, tricuspid regurgitation velocity, and inferior vena cava diameter values were high; RV fractional area change and RV dP/dT values were found to be lower than the control group. These findings indicate deterioration in right ventricular function. The RV fractional area change is the ratio of the diastolic and systolic area difference to the area of the diastolic RV. It is used to evaluate right ventricular systolic function. It is calculated by subtracting the systolic area from the right ventricular diastolic area, dividing by the diastolic area, and multiplying by 100. The limit for right ventricular systolic dysfunction is below 35%.20 Some studies have shown a strong correlation between the RV fractional area change and the ejection fraction of the RV in end-stage lung diseases.21 In our study, we observed a positive (linear) moderate correlation between the volume of the pneumothorax and the findings of the right ventricular fractional area change in patients with right-sided pneumothorax on thorax computed tomography. Barut et al., in their study examining the effects of acute smoking on the right and left ventricles, found that blood pressure and heart rate increased in smokers. Right ventricular isovolumetric relaxation and isovolumetric contraction times decrease after smoking.22 In our study, we found high values of right ventricular isovolumetric relaxation time and right ventricular isovolumetric contraction time. We believe that this is due to the negative effects on right ventricular function.
Limitations
This study has a few limitations. It is based on a single-center experience. Control echocardiography measurements were not repeated after the patients were discharged. Therefore, it could not be determined whether the changes in the right ventricular measurements we obtained were reversible.
Conclusion
Our findings indicate a positive correlation, emphasizing the importance of assessing right ventricular function through echocardiography in pneumothorax cases. This approach proves significant for monitoring changes in right ventricular function within this patient group. While we hypothesize that the impact of intrathoracic pressure on the cavaatrial junction may contribute to these findings, further research is necessary for a clearer understanding.
Declarations
Author Contributions (CRediT Taxonomy)
Conceptualization: Y.S., O.S.
Methodology: A.A., Y.K.I.
Data collection: O.E., A.S.
Formal analysis: C.P.
Investigation: H.C., A.T.
Writing – original draft: Y.S., B.S.A.
Writing – review & editing: A.A., Y.K.I.
Supervision: Y.S.
Abbreviations
ALT: Alanine Aminotransferase
AST: Aspartate Aminotransferase
BNP: B-type Natriuretic Peptide
CK-MB: Creatine Kinase–Myocardial Band
CT: Computed Tomography
DBP: Diastolic Blood Pressure
ED: Emergency Department
IVC: Inferior Vena Cava
LDH: Lactate Dehydrogenase
RV: Right Ventricle
SBP: Systolic Blood Pressure
References
- Fry WA, Paape K. Pneumothorax. In: Shields TW, LoCicero J III, Ponn RB, Rusch VW, editors. General thoracic surgery. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2005.p.794–805.
- Jantz MA, Antony VB. Pathophysiology of the pleura. Respiration. 2008;75(2):121-133. doi: 10.1159/000113629
- Strange C, Huggins JT. PNEUMOTHORAX. In: Laurent GJ, Shapiro SD, editors. Encyclopedia of Respiratory Medicine, Oxford: Academic Press Oxford; 2006.p.474-479.
- Choi WI. Pneumothorax. Tuberc Respir Dis (Seoul). 2014;76(3):99-104.
- Ioannidis G, Lazaridis G, Baka S, et al. Barotrauma and pneumothorax. J Thorac Dis. 2015;7(Suppl 1):S38-43.
- Huan NC, Sidhu C, Thomas R. Pneumothorax: Classification and Etiology. Clin Chest Med. 2021; 42(4):711-727. doi:10.1016/j.ccm.2021.08.007
- Thomsen L, Natho O, Feigen U, Schulz U, Kivelitz D. Value of digital radiography in expiration in detection of pneumothorax. Rofo. 2014;186(3):267-273. doi:10.1055/s-0033-1350566
- Kelly AM, Weldon D, Tsang AY, Graham CA. Comparison between two methods for estimating pneumothorax size from chest X-rays. Respir Med. 2006;100(8):1356-1359. doi:10.1016/j.rmed.2005.11.022
- Kelly AM, Druda D. Comparison of size classification of primary spontaneous pneumothorax by three international guidelines: a case for international consensus? Respir Med. 2008;102(12):1830-1832. doi:10.1016/j.rmed.2008.07.026
- Kanne JP, Rother MDM. Pneumothorax: Imaging Diagnosis and Etiology. Semin Roentgenol. 2023;58(4):440-453. doi:10.1053/j.ro.2023.06.004
- Henry M, Arnold T, Harvey J. BTS guidelines for the management of spontaneous pneumothorax. Thorax. 2010;65(2):18-31.
- Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.e14.
- Horton KD, Meece RW, Hill JC. Assessment of the right ventricle by echocardiography: a primer for cardiac sonographers. J Am Soc Echocardiogr. 2009;22(7):776-792.
- Ciozda W, Kedan I, Kehl DW, Zimmer R, Khandwalla R, Kimchi A. The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure. Cardiovasc Ultrasound. 2016;14(1):33.
- Lee SL, Daimon M, Kawata T, et al. Estimation of right atrial pressure on inferior vena cava ultrasound in Asian patients. Circ J. 2014;78(4):962-966.
- Oweis J, Leamon A, Al-Tarbsheh AH, et al. Influence of right ventricular structure and function on hospital outcomes in COVID-19 patients. Heart Lung. 2023;57:19-24.
- Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol. 1990;66(4):493-496.
- Ling LF, Obuchowski NA, Rodriguez L, Popovic Z, Kwon D, Marwick TH. Accuracy and interobserver concordance of echocardiographic assessment of right ventricular size and systolic function: a quality control exercise. J Am Soc Echocardiogr. 2012;25(7):709-713.
- Özsu S, Özlü T. Prognostic role of biomarkers and right ventricular dysfunction in pulmonary embolism. Tuberk Toraks. 2012;60(1):86-91.
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685-713.
- Schenk P, Globits S, Koller J, et al. Accuracy of echocardiographic right ventricular parameters in patients with different end-stage lung diseases prior to lung transplantation. J Heart Lung Transplant.2000;19(2):145-154.
- Barutcu I, Esen AM, Kaya D, et al. Effect of acute cigarette smoking on left and right ventricular filling parameters: a conventional and tissue Doppler echocardiographic study in healthy participants. Angiology. 2008;59(3):312-316.
Tables
Table 1. Analysis of vital signs and laboratory values
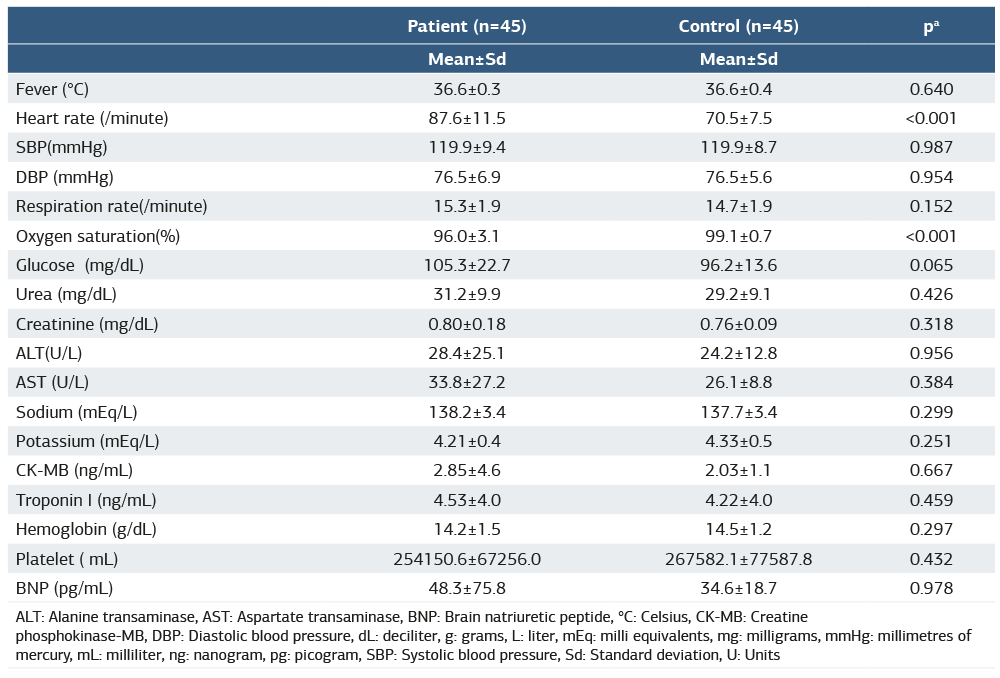
ALT: Alanine transaminase, AST: Aspartate transaminase, BNP: Brain natriuretic peptide, °C: Celsius, CK-MB: Creatine phosphokinase-MB, DBP: Diastolic blood pressure, dL: deciliter, g: grams, L: liter, mEq: milli equivalents, mg: milligrams, mmHg: millimetres of mercury, mL: milliliter, ng: nanogram, pg: picogram, SBP: Systolic blood pressure, Sd: Standard deviation, U: Units
Table 2. Pneumothorax volume on thorax CT
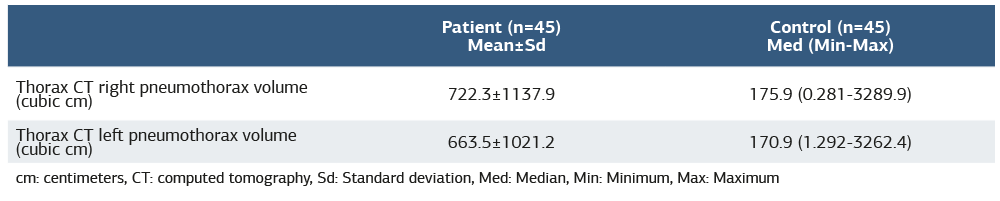
cm: centimeters, CT: computed tomography, Sd: Standard deviation, Med: Median, Min: Minimum, Max: Maximum
Figures
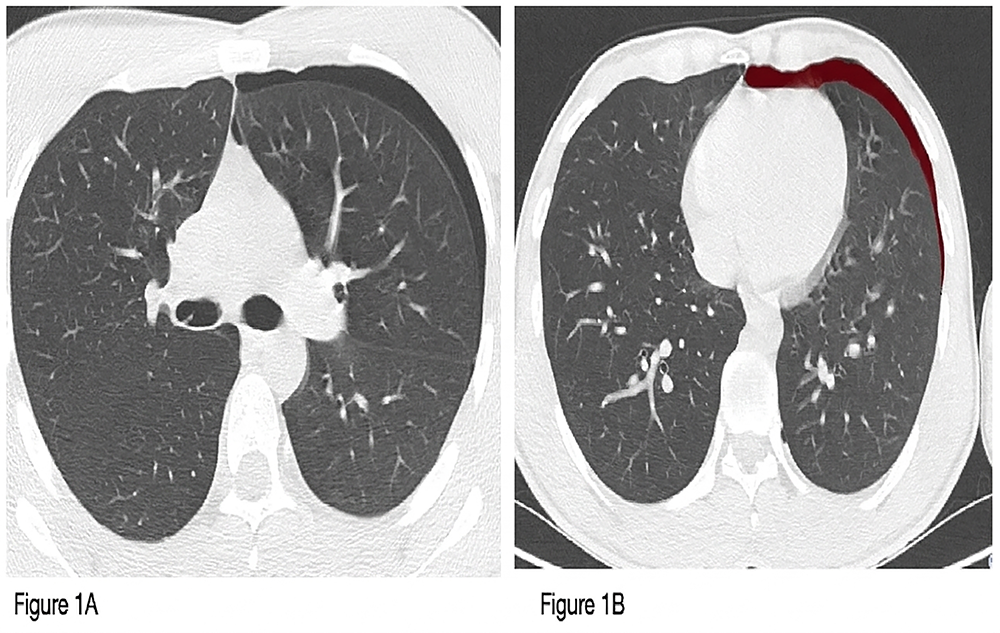
Figure 1. Pneumothorax volume measurement with the tumor tracking method. (A)Pneumothorax image on thorax tomography. (B) Measurement with the tumor tracking method
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozge Sahan, Akkan Avci, Yahya Kemal Icen, Yeliz Simsek, Osman Eroglu, Aysun Sahin, Cenk Parlatan, Hayri Cinar, Alpay Tuncar, Begum Seyda Avci. Does the percentage of pneumothorax affect right ventricular function?. doi:10.4328/ACAM.22735
Publication History
- Received:
- 12.05.2025
- Accepted:
- 16.06.2025
- Published Online:
- 29.06.2025
- Printed:
- 20.03.2026