
Sarcopenia assessment in patients with acromegaly
Sarcopenia in acromegaly
Authors
Abstract
Aim Acromegaly is a hormonal disorder characterized by excessive secretion of growth hormone. This study aimed to evaluate the prevalence of sarcopenia in patients diagnosed with acromegaly.
Methods This cross-sectional study included 50 acromegaly patients (26 females, mean age: 51 years) and 30 controls (14 males, Mean age: 51.6 years). Anthropometric parameters of the patients were measured, gait speed was calculated, bioelectrical-impedance analysis (BIA), and hand grip strength measurements were performed. Fat-free mass index (FFMI), hand grip strength, gait speed, and mid-upper arm circumference were used for the diagnosis of sarcopenia.
Results The measurements revealed a low mid-upper arm circumference in one patient with acromegaly, indicative of sarcopenia (p>0.05). The hand grip test result was indicative of sarcopenia in one control patient (p>0.05). The FFMI value was indicative of sarcopenia in three patients with acromegaly (p>0.05). Gait speed was low in four patients with acromegaly, indicative of sarcopenia (p>0.05). The appendicular lean mass-to-body mass index (ALM/BMI) ratio was indicative of sarcopenia in two patients, one from the acromegaly group and one from the control group (p>0.05). Individuals meeting two of the cut-off values proposed by the European Working Group on Sarcopenia in Older People (EWGSOP2) are diagnosed with sarcopenia. There was one patient with acromegaly who was found to meet both of these criteria. Mid-upper arm circumference and FFMI were low, indicative of sarcopenia. It proportionally corresponds to 2% of patients with acromegaly.
Conclusion Although there are various risk factors for sarcopenia, advanced age remains an independent risk factor.
Keywords
Introduction
Sarcopenia is a geriatric syndrome characterized by progressive and generalized loss of skeletal muscle mass and strength, which may lead to adverse outcomes such as falls, poor quality of life, and mortality.1
In 2010, the European Working Group on Sarcopenia in Older People (EWGSOP) published a widely used definition of sarcopenia worldwide, which has spurred advances in identifying and caring for people at risk of or with sarcopenia. This definition was then revised in 2018. In these revised guidelines, muscle strength comes to the fore as it is recognized that strength is better than mass in predicting adverse outcomes.2 Many factors, such as age, chronic diseases, increased inflammation, malnutrition, and hormonal imbalance, play a role in the etiology of sarcopenia.1,3 Although sarcopenia is usually described as an age-related process in the elderly, it can also occur at earlier ages.4
Acromegaly is a chronic condition characterized by persistent hypersecretion of growth hormone (GH) and insulin-like growth factor-I (IGF-I), mainly caused by GH-secreting pituitary adenomas. This excessive hormone production leads to many systemic complications, including metabolic disorders, cardiovascular disease, respiratory diseases, osteoarthropathy, neoplasms, and distinct phenotypic changes. Excessive levels of GH/IGF-I in acromegaly lead to insulin resistance and glucose intolerance, increasing the risk of frailty and sarcopenia, especially in elderly patients. In addition, the decrease in IGF-I levels after acromegaly treatment has been shown to increase fat accumulation and decrease lean body mass.5 The aim of this study was to evaluate the prevalence of sarcopenia in patients with acromegaly.
Materials and Methods
This study is a clinical study that was conducted using the cross-sectional comparative design. The study has a descriptive design and adopted a quantitative approach. Fifty patients with acromegaly and 30 control patients who presented to the Endocrinology and Metabolic Diseases Outpatient Clinic of Pamukkale University Hospital were included in the study. An informed consent form was obtained from each patient. According to EWGSOP2, sarcopenia can be defined as the combination of decreased muscle strength and decreased muscle mass. If weakness is detected in muscle strength, muscle mass should be measured, and sarcopenia should be diagnosed. It is suggested that sarcopenia screening be performed according to the SARC-F questionnaire (Table 1), and assessment tests are recommended for patients with suspected sarcopenia based on the SARC-F questionnaire. However, our study plan was to evaluate all acromegaly patients who presented to the Endocrinology and Metabolic Diseases Outpatient Clinic of Pamukkale University Hospital for sarcopenia; therefore, assessment tests were started without applying the SARC-f questionnaire to the patients.
Assessment ScalesAssessment of Muscle MassBioimpedance analysis (BIA) was preferred because it is an inexpensive and easy-to-use method. It was ensured that the patients did not consume anything at least 4-5 hours before the test, did not do any exercise 12 hours before the test, and did not consume alcohol and caffeine-containing beverages and foods within 24 hours prior to the test. Fat-free mass calculated by BIA in kg was proportioned to the square of the height in meters, and the fat-free mass index (FFMI) was calculated. An FFMI (kg/m2) of < 17 kg/m2 in men and < 15 kg/m2 in women was defined as low muscle mass.
Assessment of Muscle-Grip StrengthA Jamar hydraulic hand dynamometer was used to measure grip strength. The participants were asked to squeeze the dynamometer three times with their dominant hand with maximal voluntary effort, and the average of these three values was taken. According to the diagnostic algorithm of EWGSOP2, a grip strength of less than 16.0 kg in women and 27.0 kg in men was considered ‘decreased grip strength’.
Assessment of Physical PerformanceAny of the short physical performance battery tests, including usual gait speed, timed get-up-and-go test, and stair-climb power, can be used to determine physical performance. The gait speed test was preferred because of its ease of use. The participant’s time to walk 4.0 meters was recorded in seconds. According to the diagnostic algorithm of EWGSOP, a walking speed of ≤ 0.8 m/s was considered a ‘low gait speed’. Gait speed was measured twice against the possibility of lower or higher measurement values than the actual gait speed, and no significant difference was found between the measurements.
Ethical ApprovalThis study was approved by the Ethics Committee of Pamukkale University (Date: 08.06.2021, Decision No: 60116787-020/60998).
Statistical AnalysisStatistical analyses of the results from the study were carried out using SPSS [Statistical Package for the Social Sciences) Version 26 statistical software package. Descriptive statistics were expressed as mean ± standard deviation, minimum and maximum values for continuous variables, while categorical variables were expressed as numbers and percentages. Moreover, the Chi-square test was used for the analysis of categorical variables [age, gender, body mass index (BMI), gait speed, hand grip strength, FFMI, appendicular lean mass-to-body mass index (ALM/BMI) ratio, and mid-upper arm circumference]. A p-value less than 0.05 was considered statistically significant in these tests.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The study included 50 acromegaly patients, of whom 24 were male and 26 were female, and 30 control patients, of whom 14 were male and 16 were female. In the patient group, the mean age of female patients was 51.3 years, and the mean age of male patients was 50.7 years, with a mean overall age of 51 years. In the control group, the mean age of female patients was 51 years, and the mean age of male patients was 51.7 years, with a mean overall age of 51.5 years (Figure 1). The most common chronic diseases in the study population were diabetes mellitus (DM) (46%), hypertension (27%), hypothyroidism (23%), hyperlipidemia (HL) (17%), and osteoporosis (6.2%), respectively. The measurements revealed a low mid-upper arm circumference in one patient with acromegaly, indicative of sarcopenia (p>0.05). The hand grip test result was indicative of sarcopenia in one control patient (p>0.05). The FFMI value was indicative of sarcopenia in three patients with acromegaly (p>0.05). Gait speed was low in four patients with acromegaly, indicative of sarcopenia (p>0.05). The ALM/BMI ratio was indicative of sarcopenia in two patients, one from the acromegaly group and one from the control group (p>0.05) (Figure 2). Individuals meeting two of the cut-off values proposed by the European Working Group on Sarcopenia in Older People (EWGSOP2) are diagnosed with sarcopenia. There was one patient with acromegaly who was found to meet both of these criteria. Mid-upper arm circumference and FFMI were low, indicative of sarcopenia (Table 2). It proportionally corresponds to 2% of patients with acromegaly (Figure 2).
Five of the 50 patients with acromegaly (3 patients<130 ug/L, 2 patients<100 ug/L) included in the study had suppressed IGF- 1 levels, while no findings indicative of sarcopenia were noted in the measurements of these 5 patients. Vitamin D levels were low in 86% of the patients, which was not significant in terms of sarcopenia (Table 3).
Discussion
Sarcopenia is defined as age-related loss of muscle mass and muscle function that occurs after the fourth decade of life.6 This syndrome is characterized by decreased muscle strength, decreased physical performance, and low muscle mass, with an increasing prevalence, especially with aging.2 While age- related sarcopenia is defined as primary sarcopenia, sarcopenia is considered secondary when it develops due to reasons such as organ failure, inflammatory processes, endocrinological disorders, nutritional deficiencies, and decreased physical activity.7,8,9,10
There is considerable variability in the reported prevalence of sarcopenia. A recent study of community-dwelling older adults [with a mean age of 67 years) in the United Kingdom found the prevalence of sarcopenia was found to be 4.6% in the prevalence of sarcopenia. For example, a study by Bayraktar et al. evaluating sarcopenia with hand grip strength, BIA, and anthropometric measurements found a sarcopenia prevalence of 14% (7.7% in women, 20.8% in men).11 On the other hand, in their study evaluating sarcopenia using hand grip strength, gait speed, and calf circumference, Şimşek et al. reported a sarcopenia prevalence of 5.2%.12 Another study found the prevalence of sarcopenia as 31.9% using BIA, gait speed, timed up-and-go test, and hand grip strength test.13 In our study, sarcopenia was evaluated by measuring fat-free mass index (FFMI) and ALM/BMI ratio, hand grip strength test, gait speed, and mid-upper arm circumference using BIA. The difference between the studies may be due to the different criteria used for the diagnosis of sarcopenia.3
Individuals meeting two of the cut-off values proposed by the European Working Group on Sarcopenia in Older People (EWGSOP2) are diagnosed with sarcopenia.14 In our study, there was one male patient with acromegaly who met two of these criteria, while there was no patient in the control group. Mid-upper arm circumference and FFMI were low, indicative of sarcopenia. It proportionally corresponds to 2% of patients with acromegaly. The patient had no comorbidity other than acromegaly. The patient’s BMI was 17.5 kg/m2, which was considered to be associated with sarcopenia. The reason for this result was the low mid-upper arm circumference and fat-free mass index (FFMI) values from the muscle mass parameters. Serum GH and IGF-I levels decrease with increasing age, which has been associated with decreased lean body mass and increased adiposity. Several studies suggest IGF-1 as an important modulator of muscle mass, muscle strength, and function not only during development but also throughout life. 12 The situation regarding serum GH and IGF-I levels in patients with acromegaly is the opposite; however, with treatments, GH and IGF-I levels are reduced to normal limits, sometimes below normal limits. Our study showed suppressed IGF-1 levels in 5 patients with acromegaly (3 patients<130 ug/L, 2 patients<100 ug/L), while there was no finding indicative of sarcopenia in the measurements of these 5 patients. In addition, there was no difference between controls and patients with acromegaly in terms of laboratory parameters. However, large-scale prospective studies are needed to confirm this result.
Studies on sarcopenia, both in our country and in the world, have been conducted in populations aged 65 and over. Our study, on the other hand, included all acromegaly patients, regardless of age. The mean age of the acromegaly patients included in the study was 51 (range, 25-70) years. The analyses revealed a sarcopenia prevalence of 2% in patients with acromegaly. The reason for such a low prevalence of sarcopenia in our study compared to previous studies was considered to be due to the fact that a significant proportion of the patients (82% of the patients) included in the study were under 65 years of age.
Limitations
Our study has two major limitations. The first is the cross- sectional design of the study. Based on the results of this study, it can be concluded that there is only a relationship beyond causality. The second limitation is the small number of patients included in the study.
Conclusion
Although our study demonstrated a sarcopenia prevalence of 2%, no statistically significant correlation was found between laboratory parameters. However, large-scale prospective studies are needed to confirm the relationship between these parameters and sarcopenia.
Declarations
Animal and Human Rights Statement
This study was conducted in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki and its later amendments.
Informed Consent
Written informed consent was obtained from all participants included in the study.
Data Availability
The data supporting the findings of this study are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: R.C., Ş.T.
Methodology: R.C., Ş.T.
Investigation: R.C.
Data Curation: R.C.
Formal Analysis: R.C., Ş.T.
Writing – original draft preparation: R.C.
Writing – review & editing: Ş.T.
Supervision: Ş.T.
AI Usage Disclosure
The authors declare that no AI-assisted technologies were used.
Abbreviations
ALM/BMI: Appendicular lean mass-to-body mass index
BIA: Bioelectrical impedance analysis
BMI: Body mass index
DM: Diabetes mellitus
EWGSOP: European Working Group on Sarcopenia in Older People
FFMI: Fat-free mass index
GH: Growth hormone
HL: Hyperlipidemia
IGF-I: Insulin-like growth factor-I
SPSS: Statistical Package for the Social Sciences
References
-
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39(4):412-423. doi:10.1093/ageing/afq034
-
Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16-31. doi:10.1093/ageing/afy169
-
Dhillon RJ, Hasni S. Pathogenesis and management of sarcopenia. Clin Geriatr Med. 2017;33(1):17-26. doi:10.1016/j.cger.2016.08.002
-
Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636-2646. doi:10.1016/S0140-6736(19)31138-9
-
Yamamoto N, Urai S, Fukuoka H, et al. The effect of aging on quality of life in acromegaly patients under treatment. Front Endocrinol (Lausanne). 2022;13:819330. doi:10.3389/fendo.2022.819330
-
Razaq S, Kara M, Özçakar L. Sarcopenia in pediatrics? To be reconsidered. Liver Transpl. 2021;27(7):1071-1072. doi:10.1002/lt.26044
-
Meza-Valderrama D, Marco E, Dávalos-Yerovi V, et al. Sarcopenia, malnutrition, and cachexia: adapting definitions and terminology of nutritional disorders in older people with cancer. Nutrients. 2021;13(3):1-10. doi:10.3390/nu13030761
-
Bauer J, Morley JE, Schols AMWJ, et al. Sarcopenia: a time for action. An SCWD position paper. J Cachexia Sarcopenia Muscle. 2019;10(5):956-691. doi:10.1002/jcsm.12483
-
Cannataro R, Cione E, Bonanni L, et al. Sarcopenia: etiology, nutritional approaches, and miRNAs. Int J Mol Sci. 2021;22(18):9724. doi:10.3390/ijms22189724
-
Santilli V, Bernetti A, Mangone M, Paoloni M. Clinical definition of sarcopenia. Clin Cases Miner Bone Metab. 2014;11(3):177-180. doi:10.11138/ccmbm/2014.11.3.177
-
Hannon AM, Thompson CJ, Sherlock M. Diabetes in patients with acromegaly. Curr Diab Rep. 2017;17(2):8. doi:10.1007/s11892-017-0838-7
-
Ferraù F, Albani A, Ciresi A, Giordano C, Cannavò S. Diabetes secondary to acromegaly: physiopathology, clinical features and effects of treatment. Front Endocrinol (Lausanne). 2018;9:358. doi:10.3389/fendo.2018.00358
-
Keskin K, Çiftçi S, Öncü J, et al. Orthostatic hypotension and age-related sarcopenia. Turk J Phys Med Rehabil. 2021;67(1):25-31. doi:10.5606/tftrd.2021.5461
-
Trussardi Fayh AP, de Sousa IM. Comparison of revised EWGSOP2 criteria of sarcopenia in patients with cancer using different parameters of muscle mass. PLoS One. 2021;16(9):e0257446. doi:10.1371/journal.pone.0257446
Figures
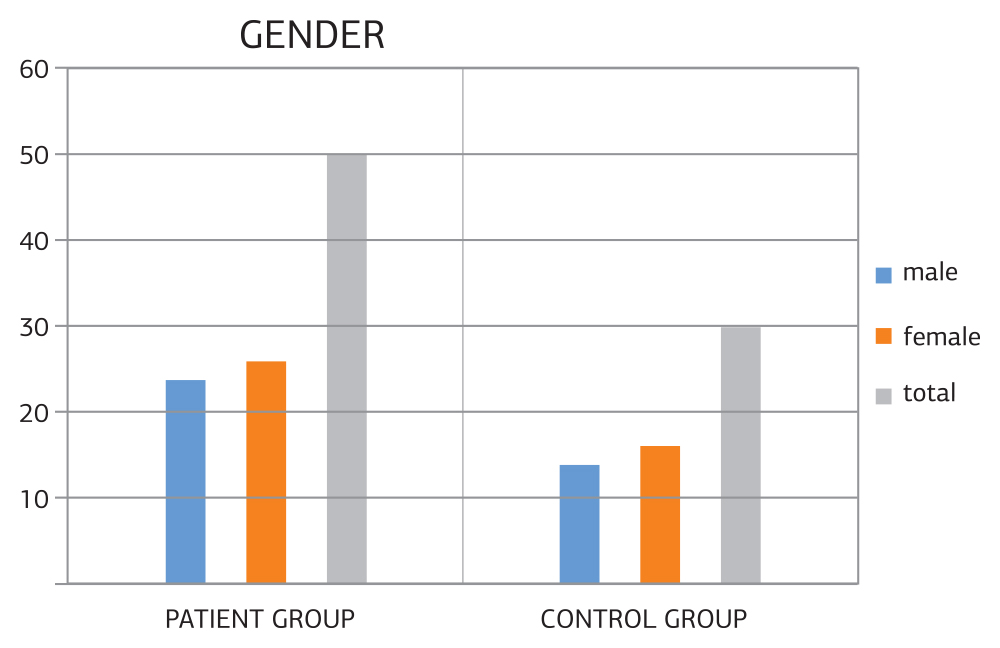
Figure 1. Distribution of patients by gender
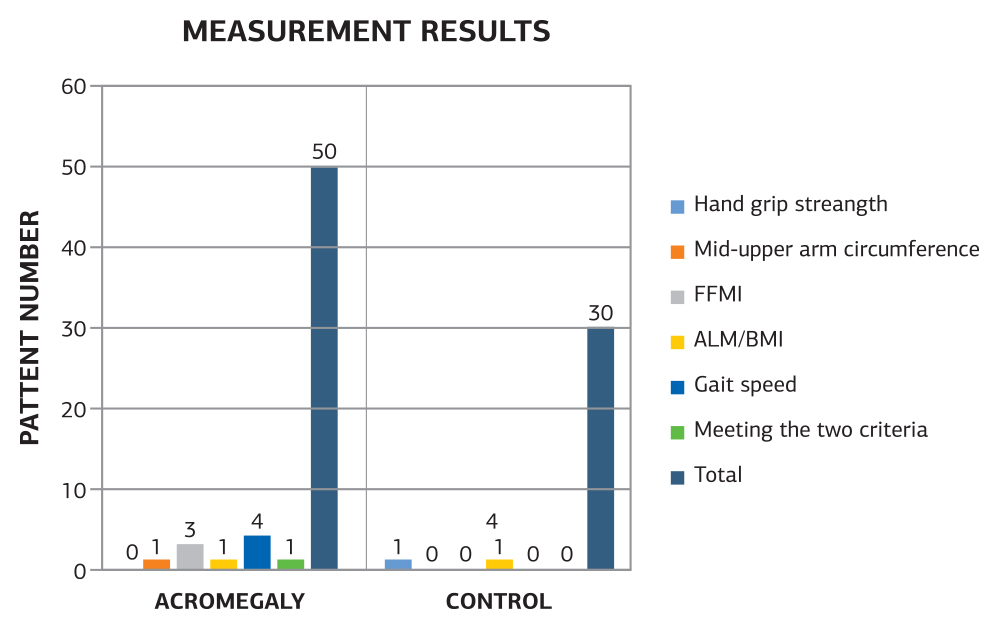
Figure 2. Measurement results of the patient and control groups
Tables
Table 1. SARC-F sarcopenia screening
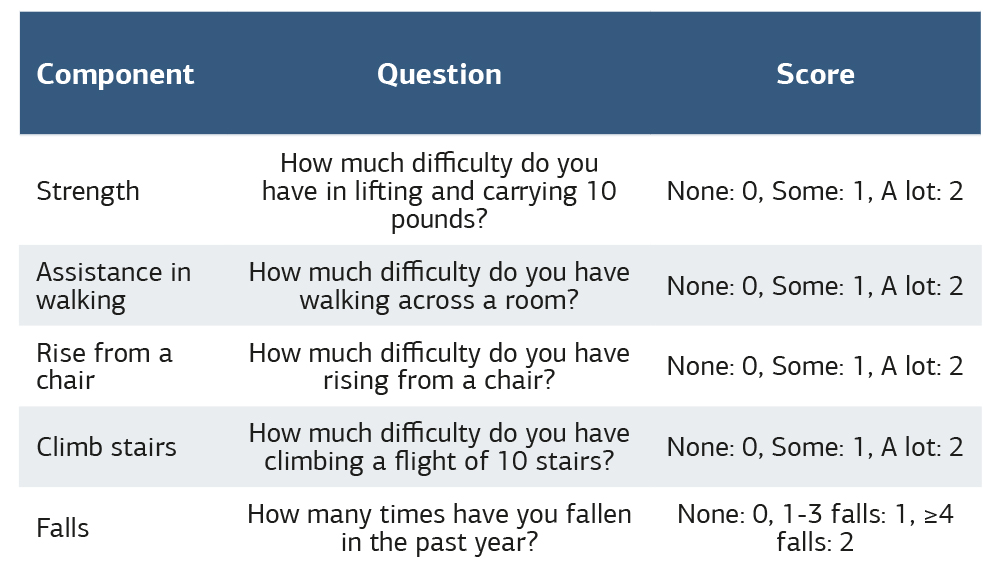
Table 2. Measurement results

FFMI: fat-free mass index, BMI: Body mass index, p<0.05, statistically significant.
Table 3. Comparison of parameters of the acromegaly and control groups
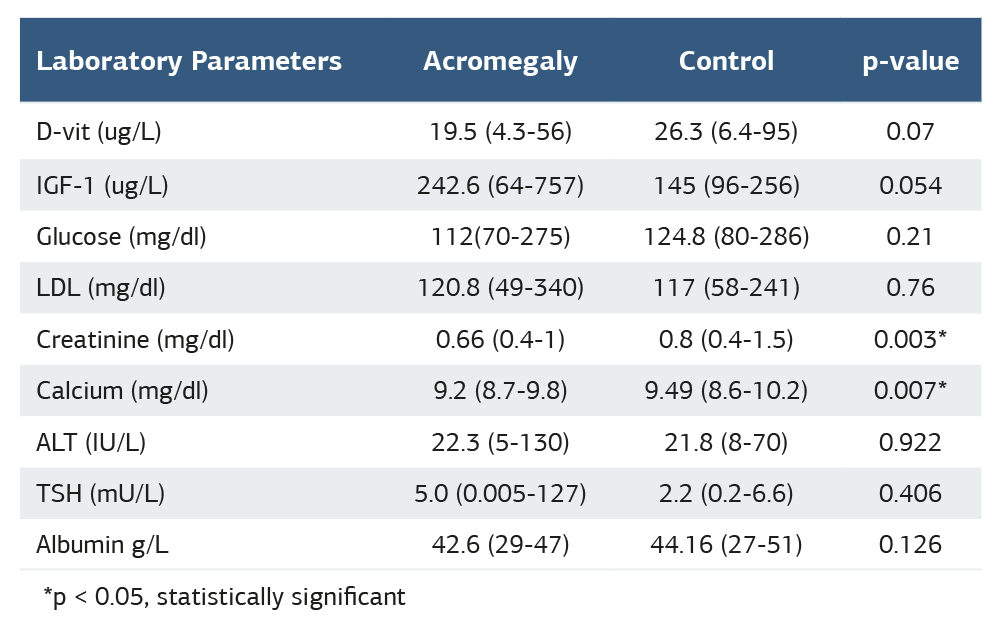
*p<0.05, statistically significant
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Rutbettin Can, Şenay Topsakal. Sarcopenia assessment in patients with acromegaly. Ann Clin Anal Med 2026;17(2):111-114. doi:10.4328/ACAM.22649
- Received:
- March 12, 2025
- Accepted:
- June 23, 2025
- Published Online:
- July 14, 2025
- Printed:
- February 1, 2026