
Abstract
Aim To analyze the real-life long-term outcomes of anti-vascular endothelial growth factor (anti-VEGF) agents (ranibizumab, aflibercept) for the treatment of neovascular age-related macular degeneration (nAMD) and the cost-effectiveness of anti-VEGF agents.Methods This is a retrospective comparative study of treatment-naïve patients who received intravitreal ranibizumab or aflibercept administration for nAMD for at least 36 months on pro re nata (PRN) regimen after 3-monthly loading injections. The study included a total of 369 eyes of 289 patients treated with only ranibizumab (n = 178 eyes), only aflibercept (n = 137 eyes), and switching from ranibizumab to aflibercept (n = 54 eyes) between 2010 and 2020. According to treatment outcomes, the visual acuity (VA) changes from baseline, the total number of injections, and the cost-effectiveness of the drugs were analyzed.Results VA changes from baseline (decimal to Snellen Chart) were + 0.09 for ranibizumab, +0.05 for aflibercept, and +0.06 for the switch group at 12-months (p=0.66). Final VA changes also were + 0.04 for ranibizumab, no change for aflibercept, and -0.04 for the switch group (p=0.76). The mean (± SD) number of injections was 6,00 (±2.76) for ranibizumab, 6,58 (±3.12) for aflibercept, and 10.18 (±3.78) for switch eyes in the 36-month follow-up period (p=0.002). We found that ranibizumab is a cost-effective treatment for AMD over aflibercept for years 1-3.Conclusion Ranibizumab and aflibercept are similarly effective and safe treatments for nAMD. Ranibizumab can be more cost-saving and cost-effective compared with aflibercept for the treatment of nAMD.
Keywords
Introduction
Age-related macular degeneration (AMD) is the leading cause of central vision loss in individuals aged 65 and over in developed countries. The prevalence of AMD is found to be 10% among those aged 65-74 and 25% in those over 75, making it a significant public health issue.1 AMD accounts for 8.7% of legal blindness globally. Dry AMD is detected in 85-90% of all AMD cases, causing 10-12% of severe vision loss. On the other hand, wet AMD, present in 10-15% of all patients, is responsible for 88% of severe vision loss due to AMD.2,3 Although the pathogenesis of wet AMD is not fully understood, vascular endothelial growth factor (VEGF) is thought to play a key role in the formation of neovascularization.4-5-6
The rapid development of neovascularization in wet AMD leads to quick central vision loss. However, with the introduction of anti-VEGF drugs, it has become possible to halt the natural progression of wet AMD. Ranibizumab was approved in the USA and Europe in 2006 and 2007, following phase III clinical trials MARINA7 and ANCHOR.8 The VIEW 1 and VIEW 29 phase III trials demonstrated that aflibercept achieved equivalent results to ranibizumab with fewer injections in wet AMD, leading to its approval in 2011-2012. These phase III clinical trials, with their strict inclusion and exclusion criteria, relatively small patient numbers, intensive treatment regimens, and limited durations, do not fully reflect real-world data. Therefore, real-world data is needed to identify weaknesses in daily practice and determine how to address them. Numerous real-world data studies on wet AMD have been presented and continue to be presented worldwide and in our country.9-10-11-12
In this study, we aimed to present our clinic’s three-year real-world data on intravitreal ranibizumab and aflibercept injection treatment in patients with wet AMD, focusing on visual gain and anatomical improvement, along with a cost analysis.
Materials and Methods
Patients diagnosed with wet AMD who were followed up at the Retina Unit of the Department of Ophthalmology at Dokuz Eylul University Faculty of Medicine between December 2010 and December 2020 were retrospectively reviewed. The study included treatment-naive patients who received either intravitreal 0.5 mg ranibizumab (Lucentis®, Novartis, Basel, Switzerland) or 2 mg aflibercept (Eylea®, Bayer, Leverkusen, Germany). A total of 369 eyes from 289 wet AMD patients, who had been regularly followed up for at least 36 months, were included in the study. Patients were classified into three groups: the ranibizumab group (Group I) with 178 eyes from 140 patients, the aflibercept group (Group II) with 137 eyes from 105 patients, and the switch group (Group III) where 54 eyes from 44 patients switched from ranibizumab to aflibercept due to inadequate response.
Patients with uveitis, diabetic retinopathy, macular edema secondary to retinal vein occlusion, pathological myopia, high hypermetropia (≥ ± 6 diopters), choroidal neovascularization due to other ocular diseases (inflammatory, idiopathic, dystrophic, traumatic, etc.), a history of ocular surgery (cataract, glaucoma, etc.) within the last 6 months, those who had undergone vitreoretinal surgery, patients who had received photodynamic therapy (PDT), and those who had undergone neodymium-doped yttrium aluminum garnet (Nd) laser capsulotomy within the last month were excluded from the study. All patients were diagnosed with wet AMD based on a comprehensive ophthalmologic examination that included dilated fundus examination, spectral-domain optical coherence tomography (SD-OCT) (Heidelberg Engineering®, Heidelberg, Germany), fundus fluorescein angiography (FFA) (Heidelberg Spectralis®), and, if necessary, indocyanine green angiography (ICGA) (Heidelberg Spectralis®). The demographic characteristics of the patients, including age, gender, eye involved, lens status, the anti-VEGF agent used, best-corrected visual acuity (BCVA) before and after treatment, intraocular pressure (IOP), presence of additional diseases (hypertension and coronary artery disease), the number of injections, and follow-up duration, were evaluated. BCVA was initially recorded using Snellen charts and converted to Early Treatment Diabetic Retinopathy Study (ETDRS) letter scores for statistical analysis, with counting fingers considered as a single letter.
Patients received three loading doses of either intravitreal ranibizumab or aflibercept at monthly intervals. The choice of drug was based on the preference of the retina specialist. After the loading phase, patients were asked to attend monthly check-ups, with all follow-up appointments scheduled at one-month intervals. Treatment was continued on a pro re nata (PRN) basis. Repeat intravitreal anti-VEGF treatment was planned in the presence of ongoing or newly developed subretinal hemorrhage, intraretinal or subretinal fluid with more than a 5-letter or 1-line loss of vision, expansion of the choroidal neovascularization membrane (CNVM) detected by FFA, newly developed CNVM, and/or an increase in central macular thickness (CMT) of at least 100 µm detected by SD-OCT. At each visit, BCVA, IOP, anterior and posterior segment examinations, and SD-OCT measurements were performed. Eye evaluations (monitoring, injection decision, switching treatment, etc.) were conducted by experienced retina specialists (MK, NK, and TO). BCVA and CMT measurements at the 3rd, 6th, 12th, 18th, 24th, and 36th-month visits post-treatment were compared, and the total number of visits and injections over 1, 2, and 3 years were recorded for analysis.
The cost analysis for wet AMD patients was based on the reimbursement amounts by the Social Security Institution as of February 22, 2021. Annual direct medical treatment costs were calculated for the first, second, and third years of treatment, considering the number of visits, diagnostic and advanced imaging (FFA, ICGA, OCT), and the annual number of intravitreal anti-VEGF injections. Cost calculations were based on the prices listed in the Health Implementation Communiqué Appendix 2A (Outpatient Treatment Payment List) revision dated February 22, 2021, with ranibizumab priced at 1,795.39 TL and aflibercept at 1,900.08 TL. In addition to the total direct medical costs, the cost per average line of vision gain on the Snellen chart was calculated. The average annual cost for eyes that maintained or lost vision after three years was also calculated.Ethical ApprovalThis study was approved by the Ethics Committee of Dokuz Eylul University (Date: 22.07.2024; Decision No: HRÜ/24.10.56). Due to the retrospective design and use of anonymized data, the requirement for informed consent was waived by the ethics committee.Statistical AnalysisAll statistical analyses were performed using SPSS version 22.0 software (SPSS Inc, Chicago, IL). Descriptive data of the patients were expressed as mean, standard deviation, and/or percentage of variables. The distribution of the data was analyzed using the Kolmogorov-Smirnov test, which confirmed normal distribution. A one-way ANOVA test was used to compare changes in BCVA, CMT scores, annual total number of injections, and total direct medical expenses between treatment groups. For within-group changes, the “Repeated Measures ANOVA” test was employed. Microsoft Office Excel 2010 was used to create graphical representations. A p-value of less than 0.05 was considered statistically significant.Reporting GuidelinesThis study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
Results
Demographic Findings The study included 369 eyes from 289 patients. The average age of the patients was 72.6 ± 9.8 years (range, 57-92 years), with a follow-up duration of 4.47 ± 2.18 years (range, 3-10 years). Of the patients, 148 (51.21%) were female. The eyes were classified as 257 (69.6%) type 1 CNVM, 99 (26.8%) type 2 CNVM, and 13 (3.5%) type 3 wet CNVM. Group I consisted of 178 eyes (48.2%) from 140 patients treated with intravitreal injections, Group II consisted of 137 eyes (37.1%) from 105 patients, and Group III consisted of 54 eyes (3.5%) from 44 patients who switched treatments. There was no statistically significant difference in age and gender distribution between the groups (p=0.49 and p=0.86, respectively). The average initial BCVA and CMT scores for the entire study population were 0.35±0.26 Snellen (range, 0.01-1) and 429.85 ± 219.85 μm (range, 130-1852 μm), respectively. There were no statistically significant differences in baseline BCVA and CMT scores between the groups (p=0.15 and p=0.33, respectively). The demographic characteristics and baseline ophthalmological findings of the patients are summarized in Table 1. Visual Acuity Results In all groups, a statistically significant and rapid improvement in visual acuity was observed at the 3-month visit following the three loading doses (p<0.001 for all groups). No significant differences in visual acuity were found between the groups at the 3-month mark (p=0.64). The average BCVA scores continued to increase in all three study arms up to the 6-month follow-up visit. At the 12-month follow-up, the BCVA (Snellen) scores were 0.41 ± 0.31 in Group I, 0.42 ± 0.33 in Group II, and 0.45 ± 0.33 in Group III, with no significant differences between the groups (p=0.66). However, after 12 months, particularly at the 24th and 36th months, a decline in visual gain was noted, with Groups II and III showing relatively more significant decreases. At the 36-month follow-up, the BCVA scores were 0.36 ± 0.32 in Group I, 0.37 ± 0.32 in Group II, and 0.35±0.26 in Group III. No statistically significant differences in visual acuity were found between the groups at the end of the 36 months (p>0.05). In Group III, switching from ranibizumab to aflibercept did not result in a significant visual improvement (p>0.05). The average visual gains for all three groups at the 3rd, 6th, 12th, 18th, 24th, and 36th-month visits are shown in Figure 1. Anatomical Outcomes In all three treatment groups, a statistically significant reduction in CMT was observed in all follow-up visits (3rd, 6th, 12th, 18th, 24th, and 36th months) compared to pre-injection CMT values, with the most significant reductions noted after the three loading doses (all p<0.05). During the first 12 months, Groups II and III showed more pronounced reductions in CMT compared to Group I, but these differences were not statistically significant (p>0.05). In Group III, a decrease in CMT was observed upon switching from ranibizumab to aflibercept treatment, but this decrease was not statistically significant (p>0.05). By the end of the 36th month, the changes in CMT in Group III were greater than those in Groups II and I; however, this difference was not statistically significant (36th month: -86 µm in Group I, -86 µm in Group II, and -127 µm in Group III; p>0.05). Figure 2 illustrates the mean changes in CMT before injection and at 3, 6, 12, 18, 24, and 36 months in all three treatment groups. Treatment and Visit Outcomes Cumulatively, Group I eyes received 3.69 ± 1 ranibizumab injections at 12 months, 4.98 ± 1.88 at 24 months, and 6 ± 2.76 at 36 months. Group II eyes received 3.97 ± 1.04 aflibercept injections at 12 months, 5.6 ± 2.15 at 24 months, and 6.58 ± 3.12 at 36 months. Group III eyes received 4.85 ± 1.75 injections (4.59 ± 1.63 ranibizumab and 2.60 ± 2.07 aflibercept) at 12 months, 7.71 ± 2.82 injections (6.12 ± 2.57 ranibizumab and 2.69 ± 1.89 aflibercept) at 24 months, and 10.18 ± 3.78 injections (6.55 ± 2.85 ranibizumab and 3.63±2.62 aflibercept) at 36 months. In Group III, the switch to aflibercept occurred after an average of 4.63 ranibizumab injections (range: 4-14) and the average transition period was 13.1 ± 3.4 months. While no significant differences were found in the average number of injections between the ranibizumab and aflibercept monotherapy groups in the 1st and 3rd years, fewer injections were administered in Group II in the 2nd year (1st year p=0.08; 2nd year p=0.03; 3rd year p=0.38). In Group III, significantly more injections were administered in all years compared to the other two groups (all p<0.05). Regarding the number of visits over 36 months of follow-up, Group I had 7.61 ± 2.19 visits at 12 months, 13.56 ± 4.5 at 24 months, and 19.07 ± 22.18 at 36 months. Group II had 7.95±1.95 visits at 12 months, 13.62 ± 5.46 at 24 months, and 15.91 ± 10.47 at 36 months. Group III had 8.5 ± 1.74 visits at 12 months, 16.24 ± 3.25 at 24 months, and 23.44 ± 5.59 at 36 months. Similar numbers of visits were observed in Groups I and II over the years (p=0.314). In Group III, a statistically significant higher number of visits was noted compared to Group I in the 1st year, both Groups I and II in the 2nd year, and Group II in the 3rd year (all p<0.05). Cost Analysis Results (Direct Medical Expenses) Table 2 shows the annual average total cost of healthcare services received by patients. During the 3-year follow-up, the total direct medical expenses in Group I were significantly lower in all years compared to the other two groups (p<0.05 for each year). There was no statistically significant difference in costs between Group II and Group III in the first year (p=0.74). However, in the 2nd and 3rd years, medical expenses in Group III were significantly higher compared to Group II (p<0.05 for both years). Comparison of Medical Expenses with Changes in Visual Acuity When examining the cost per one-line increase in visual acuity, it was found that costs were similar among the three groups in the 1st and 3rd years (p>0.05). In the 2nd year, Group I had significantly lower costs compared to the other two groups. By the end of the 3-year period, the cost for a one-line increase in visual acuity was lowest in Group I, followed by Group II, and highest in Group III (p<0.05 for each comparison). Figure 3 illustrates the cost analysis for a one-line increase in visual acuity over the 3 years across the groups. Systemic and Ocular Side Effects During long-term follow-up, the rates of serious systemic side effects were found to be similar across the groups (p>0.05). In Group I, 1 case (0.71%) of myocardial infarction occurred, and in Group II, 1 case (0.95%) of cerebrovascular event was observed. Regarding ocular side effects/complications, one case of infectious endophthalmitis occurred in Group I, while two cases of non-infectious intraocular inflammation were observed in Group II. Over the 36-month follow-up period, secondary glaucoma developed in 9 eyes (5.1%) in Group I, 9 eyes (6.6%) in Group II, and 2 eyes (3.7%) in Group III (p=0.703).Discussion
In our study, intravitreal injections of ranibizumab and/or aflibercept were found to be effective and safe for the treatment of neovascular age-related macular degeneration (nAMD). By the 36th month of long-term treatment, functional and anatomical outcomes, including visual acuity gains and CMT results, were similar across the ranibizumab monotherapy, aflibercept monotherapy, and switch groups. When analyzing the total direct medical expenses over the 36-month period for nAMD patients, it was found that the switch group was treated more expensively compared to the other two groups. The higher treatment costs were associated with the frequency of visits and the number of injections.
In this study, clinical outcomes were observed to be lower than those reported in the MARINA,7 and ANCHOR,8 VIEW 1, and VIEW 29 trials. The lower visual gains in real-world clinical settings compared to randomized controlled trials (RCTs) can be attributed to several factors: fewer injections administered to patients, less stringent monitoring, and the inclusion of all patients receiving treatment regardless of visual acuity. The AURA real-world study14 and a broad meta-analysis by Kim et al.10 have also reported fewer injections and less significant improvements in visual acuity with ranibizumab compared to RCT results. Similarly, the RAINBOW real-world study evaluating intravitreal aflibercept injections in nAMD patients showed data on letter gain, central macular thickness changes, injection, and visit counts over 4 years.15 The LUMINOUS real-world study, one of the largest 5-year, prospective, observational, multi-center, single-arm global studies evaluating ranibizumab’s efficacy and safety for nAMD, included data from 30,138 patients across 42 countries.16 Both the RAINBOW and LUMINOUS studies, like many other observational studies reporting real-world data, showed fewer injections and lower visual gains compared to RCTs.15,16 In our study, no significant difference was found in visual gains and the number of injections between the ranibizumab and aflibercept groups. These real-world data reflect a similarity to the international and Turkish real-world data from several centers regarding injection numbers and visual gains. Significant real-world studies assessing anti-VEGF treatment in AMD have provided valuable insights into visual acuity, CMT changes, injection, and visit counts over the long term. A summary of key international and national studies, outlining visual acuity, CMT changes, and injection and visit counts for anti-VEGF treatment in AMD, is provided in Supplementary Table 1.7,9-10-11-12-13-14-15-16-17-18-19-20
In the current era, cost-effectiveness evaluation has become a critical aspect of presenting real-world data for AMD. A broad meta-analysis assessing the cost-effectiveness of intravitreal aflibercept and ranibizumab injections found that intravitreal aflibercept is a more effective treatment option compared to ranibizumab, with an incremental cost-effectiveness ratio (ICER) of €27,087 per quality-adjusted life year (QALY). The analysis indicated that aflibercept provides increased QALYs (4.918 vs. 4.880) and a better cost-effectiveness profile.21 In a study conducted in Türkiye evaluating the cost of intravitreal ranibizumab injections for AMD, the total direct medical cost per patient was found to be 9,628 TL after 2 years, with the cost of visual acuity improvement of one line being 11,911 TL in the first year. Due to vision loss, the cost for the second year could not be calculated.22 Our study’s findings on total direct medical costs indicate that, throughout all years, the ranibizumab group had lower total direct medical expenses compared to both the aflibercept and switch groups. Specifically, during the 2nd and 3rd years, the switch group incurred significantly higher costs. Furthermore, at the end of the 1st year, the cost per line of visual improvement was significantly lower in the ranibizumab group compared to the other two groups, demonstrating more cost-effective results for ranibizumab. These results align with international studies and underscore the importance of considering cost-effectiveness in treatment decisions for AMD, especially in real-world settings where treatment adherence and monitoring might differ from clinical trials.
Limitations
Our study has several limitation(a) Quality of Life Assessment: There is a lack of prospective studies assessing the quality of life in AMD patients in our country. Our study did not include a quality-of-life evaluation, which could provide valuable insights into the broader impacts of treatment.
(b) Visual Acuity Measurement: Visual acuity was recorded using the Snellen decimal system. Although we converted these values to ETDRS letter equivalents for comparison with international literature, some discrepancies may arise due to inevitable small variations in these conversions.
(c) Cost Analysis Scope: We only calculated direct treatment costs, excluding direct non-medical and indirect treatment expenses. A comprehensive cost analysis should also consider these additional costs.
(d) Study Design: The study was conducted at a single center with a limited number of patients, which may restrict the generalizability of the results. To accurately assess national direct medical treatment costs for AMD, multi-center studies with larger patient populations are necessary.
Conclusion
Our study provides potential insights into the direct cost accounting of long-term treatment effectiveness and treatment-burden in AMD. It was found that the efficacy and safety of ranibizumab and aflibercept treatments were similar over the long term, with ranibizumab showing a more cost-effective profile in terms of lower costs for equivalent outcomes. The findings are significant for evaluating licensed intravitreal anti-VEGF therapies regarding their long-term cost and effectiveness. We believe that our study can guide cost-effective treatment planning for AMD in our country.
Declarations
Author Contributions (CRediT Taxonomy)
Conceptualization: B.A.Y., M.K.
Methodology: B.A.Y., N.K.
Formal Analysis: T.O.
Investigation: B.A.Y., M.K., N.K., T.O.
Data Curation: B.A.Y.
Writing – Original Draft Preparation: B.A.Y.
Writing – Review & Editing: M.K., N.K., S.K.
Supervision: S.K.
Abbreviations
AMD: Age-related macular degeneration
ANOVA: Analysis of variance
BCVA: Best-corrected visual acuity
CMT: Central macular thickness
CNVM: Choroidal neovascular membrane
ETDRS: Early treatment diabetic retinopathy study
FFA: Fundus fluorescein angiography
ICER: Incremental cost-effectiveness ratio
ICGA: Indocyanine green angiography
IOP: Intraocular pressure
nAMD: Neovascular age-related macular degeneration
OCT: Optical coherence tomography
PRN: Pro re nata
QALY: Quality-adjusted life year
SD: Standard deviation
VEGF: Vascular endothelial growth factor
References
- Smith W, Assink J, Klein R, et al. Risk factors for age-related macular degeneration: pooled findings from three continents. Ophthalmology. 2001;108(4):697-704. doi:10.1016/S0161-6420(00)00580-7
- Klein R, Meuer SM, Myers CE, et al. Harmonizing the classification of age-related macular degeneration in the three-continent AMD consortium. Ophthalmic Epidemiol. 2014;21(1):14-23. doi:10.3109/09286586.2013.867512
- Age-Related Eye Disease Study Research Group. The Age-Related Eye Disease Study system for classifying age-related macular degeneration from stereoscopic color fundus photographs: Age-Related Eye Disease Study Report No. 6. Am J Ophthalmol. 2001;132(5):668-681. doi:10.1016/S0002-9394(01)01218-1
- Penfold PL, Madigan MC, Gillies MC, Provis JM. Immunological and aetiological aspects of macular degeneration. Prog Retin Eye Res. 2001;20(3):385-414. doi:10.1016/S1350-9462(00)00025-2
- Jager RD, Mieler WF, Miller JW. Age-related macular degeneration. N Engl J Med. 2008;358(24):2606-2617. doi:10.1056/NEJMra0801537
- Abugreen S, Muldrew KA, Stevenson MR, VanLeeuwen R, DeJong PT, Chakravarthy U. CNV subtype in first eyes predicts severity of ARM in fellow eyes. Br J Ophthalmol. 2003;87(3):307-311. doi:10.1136/bjo.87.3.307
- Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431. doi:10.1056/NEJMoa054481
- Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57-65.e5. doi:10.1016/j.ophtha.2008.10.018
- Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537-2548. doi:10.1016/j.ophtha.2012.09.006
- Kim LN, Mehta H, Barthelmes D, Nguyen V, Gillies MC. Meta-analysis of real-world outcomes of intravitreal ranibizumab for the treatment of neovascular age-related macular degeneration. Retina. 2016;36(8):1418-1431.
- Cebeci Z, Yilmaz YC, Kir N. Real-life experience of ranibizumab therapy for neovascular age-related macular degeneration from Turkey. Int J Ophthalmol. 2018;11(2):267-273.
- Sizmaz S, Esen E, Isik-Ericek P, Demircan N. Comparison of intravitreal injections of ranibizumab and aflibercept in neovascular age-related macular degeneration. Clin Exp Optom. 2022;105(1):55-60.
- Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444. doi:10.1056/NEJMoa062655
- Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99(2):220-226. doi:10.1136/bjophthalmol-2014-305327
- Cohen SY, Dominguez M, Coscas F, et al. Final 4-year results of the RAINBOW real-world study: intravitreal aflibercept dosing regimens in France in treatment-naive patients with neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2023;261(4):959-969.
- Holz FG, Minnella AM, Tuli R, Yoganathan P, Parikh S, Hamilton R, et al. Ranibizumab treatment patterns in prior ranibizumab-treated neovascular age-related macular degeneration patients: real-world outcomes from the LUMINOUS study. PLoS One. 2020;15(12):e0244183. doi:10.1371/journal.pone.0244183
- Horner F, Lip PL, Clark H, Chavan R, Sarmad A, Mushtaq B. Real-world visual and clinical outcomes for patients with neovascular age-related macular degeneration treated with intravitreal ranibizumab: an 8-year observational cohort (AMD8). Clin Ophthalmol. 2019;13:2461-2467.
- Framme C, Eter N, Hamacher T, et al. Aflibercept for patients with neovascular age-related macular degeneration in routine clinical practice in Germany: twelve-month outcomes of PERSEUS. Ophthalmol Retina. 2018;2(6):539-549.
- Almuhtaseb H, Johnston RL, Talks JS, Lotery AJ. Second-year visual acuity outcomes of nAMD patients treated with aflibercept: data analysis from the UK Aflibercept Users Group. Eye (Lond). 2017;31(11):1582-1588.
- Chandra S, Rasheed R, Menon D, et al. Impact of injection frequency on 5-year real-world visual acuity outcomes of aflibercept therapy for neovascular age-related macular degeneration. Eye (Lond). 2021;35(2):409-417.
- Carrasco J, Pietsch GA, Nicolas MP, Koerber C, Bennison C, Yoon J. Real-world effectiveness and real-world cost-effectiveness of intravitreal aflibercept and intravitreal ranibizumab in neovascular age-related macular degeneration: systematic review and meta-analysis of real-world studies. Adv Ther. 2020;37(1):300-315.
- Yildirim S, Akkin C, Oztas Z, Nalcaci S, Afrashi F, Mentes J. Direct treatment costs of neovascular age-related macular degeneration and comparison of gained and/or preserved vision with expenditure. Turk J Ophthalmol. 2018;48(1):27-32.
Tables
Table 1. Patient demographics and initial eye health assessments for each treatment group
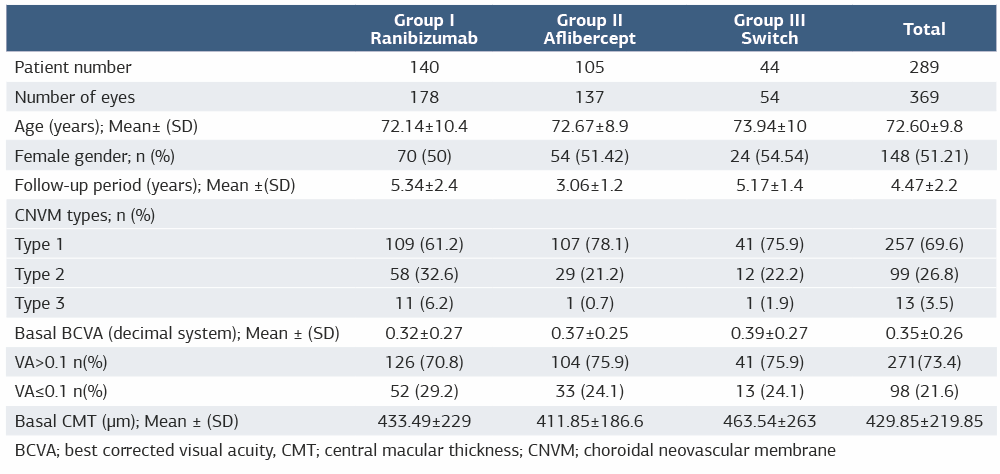
BCVA; best corrected visual acuity, CMT; central macular thickness; CNVM; choroidal neovascular membrane
Table 2. Annual average total direct medical expenses (Unit, TL)

Figures
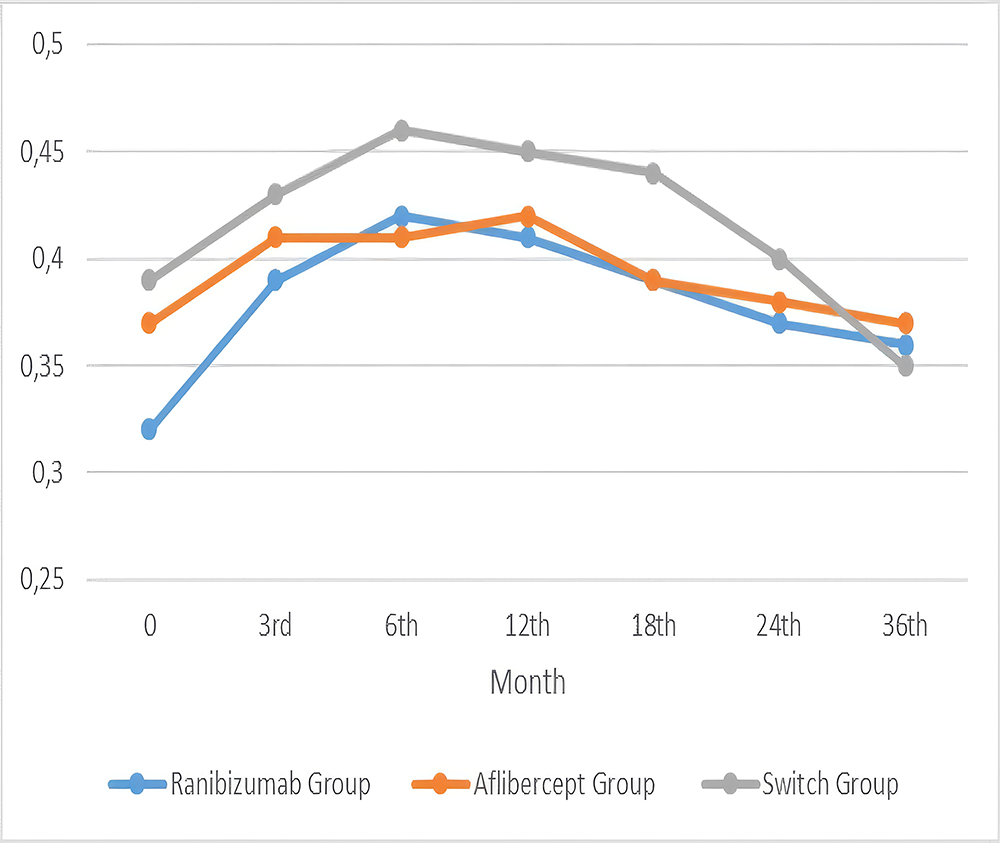
Figure 1. Three-year visual acuity changes in treatment groups
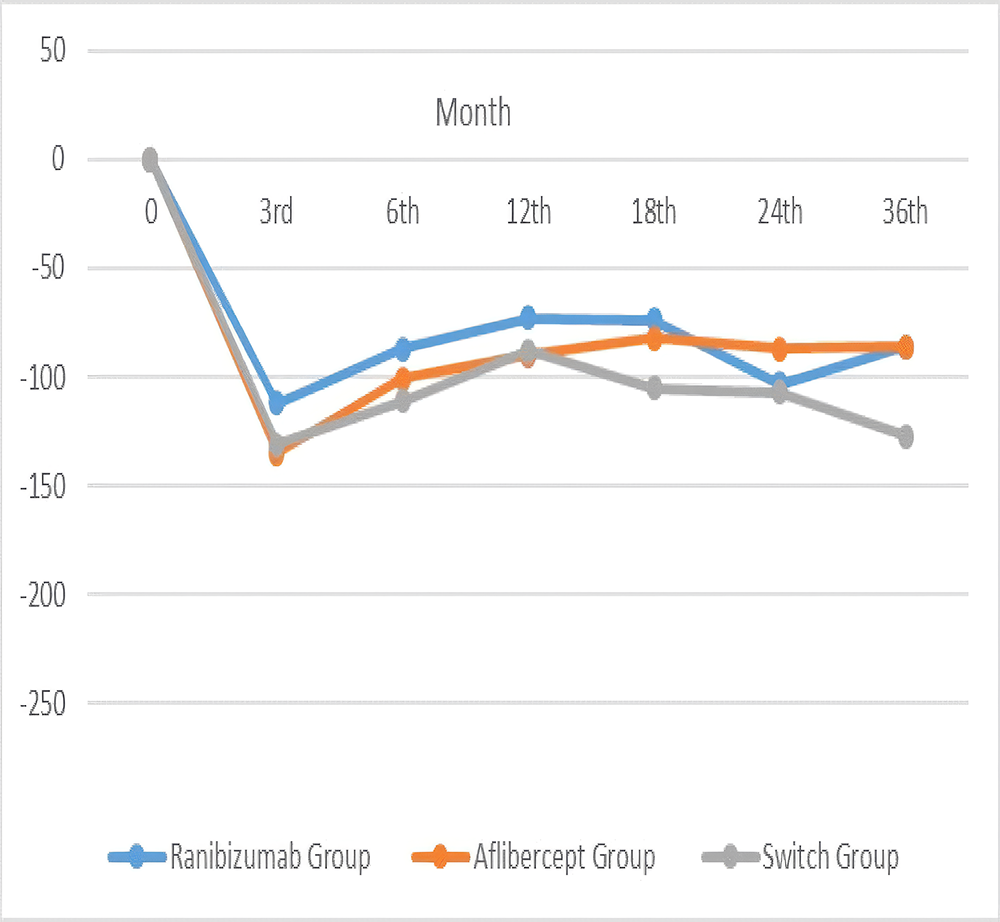
Figure 2. Three-year follow-up of cmt changes post-injection in treatment groups
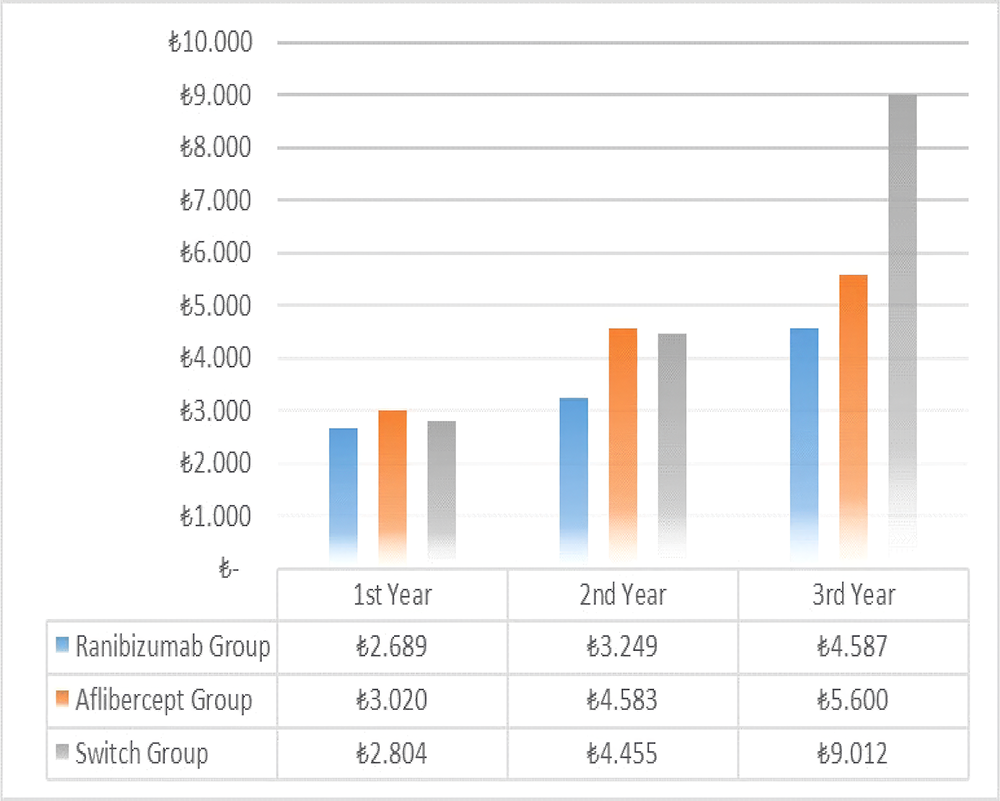
Figure 3. Cost per line gain in snellen acuity over three-year follow-up in treatment groups
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Betul Akbulut Yagci, Mahmut Kaya, Nilufer Kocak, Taylan Ozturk, Suleyman Kaynak. Real-life experience and direct treatment costs in treatment of neovascular age-related macular degeneration. Ann Clin Anal Med 2026;17(3):196-202. doi:10.4328/ACAM.22693
Publication History
- Received:
- 08.04.2025
- Accepted:
- 19.05.2025
- Published Online:
- 09.07.2025
- Printed:
- 01.03.2026