
Diagnostic accuracy of imaging modalities in periampullary tumors: comparison of CT, MRI and EU
Imaging in periampullary region tumors
Authors
Abstract
Aim Pancreatic cancers are diagnosed late due to nonspecific symptoms that are present in patients. Poor prognosis is the result of late diagnosis and low complete resection rate. Our aim was to compare the sensitivity of diagnostic imaging methods (e.g., computed tomography, magnetic resonance imaging, and endoscopic ultrasound), when used separately and together, for periampullary region tumors.
Methods This study retrospectively examined the accuracy of diagnostic tests. A total of 57 patients (21 women and 36 men) were included in the study. The superiority of the tests used in the diagnosis of cancer and their ability to detect major vascular invasion and lymph node involvement in patients operated on for periampullary region tumor were compared.
Results Of the patient group, 21.1% had inoperable tumors and 78.9% had malignant tumors that could be operated on. While major vascular invasion was detected in 21.1% (n=12) of the 57 patients, lymph node involvement was detected in 49.1% (n=28). When three diagnostic tests were used together for major vascular invasion and lymph node involvement, the sensitivity, specificity, and area under the curve were higher than when the tests were used alone.
Conclusion In our study, the combined use of the three tests significantly increased their diagnostic performance.
Keywords
Introduction
Pancreatic cancer is the seventh leading cause of cancer- related death worldwide due to poor prognosis and that less than 5% of patients survive 5 years after diagnosis.1 This poor survival is the result of late diagnosis and low complete resection rate.2 Risk factors for pancreatic cancer include diabetes, older age, smoking, obesity, history of chronic pancreatitis, genetic syndromes, or family history. Although painless jaundice is a characteristic symptom of pancreatic cancers, nonspecific symptoms, such as weight loss, abdominal pain, and fatigue cause delays in diagnosis. Pancreatic cancer typically has mild symptoms, and a small number of patients are diagnosed at a suitable stage for resection and possible treatment.3 However, the 5-year survival rate of patients with tumors confined to the duct epithelium can reach 100% if the tumors are smaller than 1 cm.4 Therefore, early diagnosis of pancreatic cancer is very important. It is estimated that an average of 11.7 years pass from the onset of the tumor to the development of obvious cancer, while it is estimated that an average of 6.8 years pass between the development of obvious cancer and the emergence of the disease.5 In fact, these timings show that there is a long period allowing for the early detection of pancreatic cancers.
With the increasing use of imaging methods, incidental detection of pancreatic lesions is increasing. Medical imaging has an important role in pancreatic cancer screening and early diagnosis, preoperative evaluation and staging, differential diagnosis, follow-up, and treatment evaluation. However, routine screening for pancreatic cancer is generally not recommended for patients who are asymptomatic, except for those with specific inherited genetic syndromes or a family history of pancreatic cancer.6 Differentiating between benign lesions and precancerous and cancerous lesions can prevent patients from undergoing unnecessary major surgery. Additionally, there are currently no biomarkers with sufficient sensitivity and specificity to be applied in the clinic for the diagnosis of pancreatic cancer. Carbohydrate antigen 19-9 (CA19-9), which is the only serum biomarker approved by the United States Food and Drug Administration, is not recommended for use alone in the early screening of pancreatic cancer due to its limited specificity.7
In the presence of clinical suspicion and risk factors, computed tomography (CT) is primarily recommended, in addition to magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP), endoscopic retrograde cholangiopancreatography (ERCP), endoscopic ultrasound (EUS), and EUS-guided fine needle aspiration also play important roles in diagnosis.8 Of these imaging methods, EUS is frequently used for the benefit of simultaneous biopsy of pancreatic tissue with a high sensitivity of 98%.9 Although there are studies comparing imaging methods in pancreatic cancers, there is no study where more than one diagnostic test is applied, and their common results are compared with the gold standard diagnostic method (histopathological results). In this study, we compared the diagnostic accuracy of imaging methods (CT, MRI, and EUS) and investigated the effect of using all methods together (CT+MRI+EUS) on the accuracy of diagnosis.
Materials and Methods
Patients diagnosed with pancreatic cancer between August 1, 2017, and August 1, 2022, were found from the hospital automation system. Patients who underwent EUS, abdominal CT, and MRI imaging, and had surgery due to pancreatic cancer were included in the study. The exclusion criteria were patients younger than 18 years and patients with file records could not be accessed from the hospital automation system. Demographic characteristics were recorded from patient files. Tumor size, lymph node and vascular invasion in EUS, abdominal CT, MRI, pathological results, and operative findings were evaluated.
Preoperative images of periampullary masses obtained by CT, upper abdominal MRI, and EUS were obtained. EUS was performed by either of the senior gastroenterologists of this report with the EG38700UTK type echoendoscope (Pentax, Orangeburg, NY, USA). A curvilinear array transducer with ultrasound frequency of 5–12 megahertz (MHz) was used for all patients. The criteria for tumor size included the largest diameter (cm) of a well-demarcated lesion with an echo- poor, homogeneous pattern. Lymph nodes were considered malignant if their maximum diameter was larger than 0.5 cm, as reported previously10,11,12 If the lymph nodes did not meet the size criteria or were not visualized, the regional lymph nodes were considered as benign. Major vascular involvement was established to be positive if direct tumor extension was seen in the vessel lumen, if vascular obstruction was noted, or if there was irregularity of the vessel wall and obliteration of the hyperechoic interface between the tumor and the major vessel.12,13
Helical CT scans were performed at our institution using a 128-detector multi detector CT unit (Philips Ingenuity 128, Eindhoven, Netherlands). Technical parameters were determined at 120 peak kilovoltage (kvP), 200–400 milliampere-second (mAs), rotation time 0.42 seconds, and slice thickness 1 mm for all phases. All patients were given water-soluble oral contrast material before the procedure. Contiguous 1-mm sections were obtained from the peripancreatic area; both non-contrast and enhanced images were taken after bolus injection of 100 mL of nonionic iodinated contrast solution at a rate of 2–3 mL/sec. Helical CT scanning started immediately after contrast injection. The scans were analyzed and reviewed by two radiologists experienced in abdominal imaging. Tumor size criteria included the largest diameter (cm) of a well-circumscribed lesion. Lymph nodes were considered malignant if their maximum diameter was larger than 1.0 cm, consistent with CT radiology literature. Major vascular involvement was determined to be positive if direct tumor extension was seen in the vessel lumen, if vascular thrombosis was noted, or if there was irregularity of the vessel wall and obliteration of the interface between the tumor and the major vessel.14,15
MRI was performed using a phased-array superficial body coil on a 1.5T MRI device (Philips Ingenia, Best, Eindhoven, Netherlands). In the T2A axial sequence, images were created using a 268x259 matrix, field of view (FOV) of 350 mm, slice thickness of 5 mm, slice spacing of 0.8 mm, and TR/TE of 4608/100 milliseconds (ms). In the T2W sagittal sequence, images were created using a 220x205 matrix, FOV of 220 mm, slice thickness of 3 mm, slice interval of 0.5 mm, and TR/TE of 3299/110 ms. In the T2A coronal sequence, images were obtained with 312x186 matrix, FOV 250 mm, section calings 4 mm, section interval 0.4 mm, TR/TE 5760/100 ms. In the pre-post contrast T1A axial and sagittal sequence, images were obtained with a 312x224 matrix, FOV of 150 mm, slice thickness of 4 mm, slice interval of 0.4 mm, and TR/TE of 514/8 ms. For the dynamic T1A axial sequence, the configuration was a 220x223 matrix, FOV of 240 mm, TR/TE of 6.0/1.88, dynamic scan time of 00:10.5 sec, and k0 time of 00:03.0 s.
All variables of the periampullary tumors were compared with explorative findings and the pathological specimens for the patients were those diagnosed as periampullary tumors.
Ethical ApprovalThis study was approved by the Ethics Committee of Health Science University, Adana City Training and Research Hospital (Date: 2022-09-08, No:111/2119).
Statistical AnalysisStatistical package for the social sciences (SPSS) 25.0 (SPSS Inc, Chicago, IL, USA) was used for statistical analysis. Categorical values were presented as percentages and numbers, while continuous variables were presented as mean ± standard deviation (SD) (SD; median and minimum, or maximum where appropriate). Receiver operating characteristic (ROC) analysis was applied to compare the diagnostic accuracy of imaging methods and the area under the curve (AUC) was calculated. With this analysis, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for each variable. Simple linear regression analysis for the pathological dimension was applied. For all tests, the statistical significance was set at p<0.05
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
A total of 57 patients of which 21 (36.8%) were women and 36 were (63.2%) men were included in the study. Of the cohort, 21.1% (n=12) had inoperable tumors and 78.9% (n=45) had malignant tumors that could be operated on. The age range of the participants was 37–85 years. According to the pathology results, major vascular invasion was detected in 21.1% (n=12) of patients while lymph node involvement was detected in 49.1% (n=28).
CT scans provided the most obvious result among the diagnostic tests for major vascular invasion involvement. In addition, when examined in the context of the area under the curve (AUC) value, CT scans showed excellent performance (98%). EUS and MRI showed good performance in terms of AUC values (84% and 86% respectively) and also showed similar results in terms of sensitivity and specificity. In cases where 3 diagnostic tests are used together, the sensitivity and specificity values of the diagnostic tests are 100%, again the AUC value was also found to be 100%. (table 1).
When three diagnostic tests were used together for lymphadenopathy, the sensitivity of the diagnostic tests was 95%, the specificity was 75.7%, and the AUC value was 85% (table 2).
When the data in the table is examined, the results obtained for EUS and the results from the pathological dimension were in 95% agreement, reflecting the linear results regarding the data obtained in the pathological dimension (table 3).
In addition, when the data regarding the beta coefficient is examined, the highest beta coefficient value was with EUS. All variables had a significant relationship (p<0.05) in the model.
Discussion
Different imaging methods have varied abilities for the detection of early pancreatic cancer. The only treatment method for diagnosed patients is surgery, but there are criteria that determine the operability of these patients. In the absence of metastatic disease that would prevent resection, evaluation of vascular invasion is an important parameter to determine the resectability of pancreatic cancer.2 The gold standard imaging test for determining vascular invasion is CT scanning. In our study, CT scans provided the most obvious result among the diagnostic tests showing major vascular invasion involvement. Although CT scanning is the best diagnostic test, the combined use of the three tests gave better results than CT scans alone and provided the best results for all parameters.
Hashemzadeh et al. reported that CT scanning has very low sensitivity but high specificity in detecting vascular invasion (sensitivity 16.7%, specificity 100%, positive predictive value (PPV) 100%, and negative predictive value (NPV) 83.87%).16 In another study, Karmazanovsky et al. reported the sensitivity, specificity, PPV, NPV and accuracy of CT in the diagnosis of vascular invasion as 94% and 84%, 94%, 84% and 91.3 respectively.17 In a meta-analysis by Nawaz et al. that included the evaluation of the vascular invasion ability of EUS and CT scans, the sensitivity, specificity, PPV, and NPV of EUS were 86%, 93%, 88%, and 90% while the CT values were 58%, 95%, 90%, and 75%.12 Zhang et al. also found the sensitivity and specificity values for major vascular invasion diagnosis to be 71% and 92%, respectively, for multidetector CT scans, and 67% and 94%, respectively, for MRI.18 Howard et al. reported 63% sensitivity, 100% specificity, and 86% overall accuracy for vascular invasion from CT scans of 21 patients with periampullary carcinoma.19 Studies show that the specificity of the gold standard multidetector CT scans are generally close to perfect, but its sensitivity varies across studies. In our study, although both sensitivity, specificity, and AUC were close to perfect, the combined method including CT+MRI+EUS was better. It is possible that this diagnostic method will prevent unnecessary operations in patients with organ metastases or major vascular invasion that cannot be distinguished by single imaging methods and are diagnosed intraoperatively. However, since there are few studies on this topic and these three tests are more expensive, further studies are required for validation. Considering that performing these three tests on the same patient will take more time and increase costs, the benefits of whether they are performed routinely or not should be examined in future studies.
While major vascular invasion was detected in 21.1% (n=12) of the 57 patients, lymph node involvement was detected in 49.1% (n=28). Vascular invasion is a relatively common condition in pancreatic cancer and is reported in 21–64% of patients, depending on the sample taken.20 Yamada et al. reported venous invasion at a high rate of 64.5%.21 The reason why the diagnosis of major vascular invasion was comparatively low at 21.1% in our study, could be because pancreatic cancer was detected at an earlier period or because imaging methods are performed easily and in large numbers in our country.
In our study, when three diagnostic tests in the evaluation of lymph node metastases were used together, the sensitivity of the diagnostic tests was 95%, specificity was 75.7%, and the AUC value was 85%. These rates are higher diagnostic values compared with using the tests separately. In a meta-analysis investigating the accuracy of CT scans for the evaluation of lymph node metastases in pancreatic and periampullary cancer, the diagnostic accuracy of CT scans for lymph node metastasis was low possibly because of lower CT sensitivity.22 However, the authors noted that PPV varied greatly between studies, with values ranging from 0% to 100%.22 In our study, the AUC value of CT scanning was relatively low and the AUC of EUS was higher. In any case, the triple diagnostic method of CT+MRI+EUS has the highest diagnostic ability of detecting lymph node metastasis.
Limitations
In our study, the EUS method was performed without the use of needle biopsy. However, conventional EUS cannot effectively distinguish between carcinomas and other etiologies without the use of invasive cytological examination because most pancreatic tumors, even those of benign etiologies, have a hypoechogenic appearance.
Conclusion
CT scanning continues to be the most used method for the diagnosis of vascular invasion and lymph node metastasis of periampullary pancreatic cancers. In our study, the method created by combining the results of three methods (CT+MRI+EUS) significantly increased diagnostic performance.
Declarations
Ethics Declarations
The study was approved by the Ethics Committee of Health Sciences University, Adana City Training and Research Hospital (Decision No: 111/2119). All procedures were conducted in accordance with the Declaration of Helsinki.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Due to the retrospective design of the study, the requirement for written informed consent was waived by the institutional ethics committee.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.K., M.O.T.
Methodology: A.K., B.S.A.
Investigation: M.O.T., O.Y., Y.S.
Data curation: A.B.U., E.A.
Formal analysis: A.K., M.A.
Resources: A.B.U., E.A., A.A.
Writing – original draft: A.K., B.S.A.
Writing – review & editing: A.P., A.A.
Supervision: A.P.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AUC: Area Under the Curve
CI: Confidence Interval
CT: Computed Tomography
EUS: Endoscopic Ultrasound
MRI: Magnetic Resonance Imaging
NPV: Negative Predictive Value
PPV: Positive Predictive Value
ROC: Receiver Operating Characteristic
SPSS: Statistical Package for the Social Sciences
References
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
-
Ahmad NA, Kochman ML, Lewis JD, et al. Endosonography is superior to angiography in the preoperative assessment of vascular involvement among patients with pancreatic carcinoma. J Clin Gastroenterol. 2001;32(1):54-58. doi:10.1097/00004836-200101000-00013
-
Owens DK, Davidson KW, Krist AH, et al. Screening for pancreatic cancer: US preventive services task force reaffirmation recommendation statement. JAMA. 2019;322(5):438-444. doi:10.1001/jama.2019.10232
-
Ariyama J. [Detection and prognosis of small pancreatic ductal adenocarcinoma]. Nihon Geka Gakkai Zasshi. 1997;98(7):592-596.
-
Yachida S, Jones S, Bozic I, et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature. 2010;467(7319):1114-1117.
-
Canto MI, Hruban RH, Fishman EK, et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology. 2012;142(4):796-804.
-
Bunganič B, Laclav M, Dvořáková T, et al. Accuracy of EUS and CEH EUS for the diagnosis of pancreatic tumours. Scand J Gastroenterol. 2018;53(10-11):1411-1417.
-
Lee ES, Lee JM. Imaging diagnosis of pancreatic cancer: a state-of-the-art review. World J Gastroenterol. 2014;20(24):7864-7877.
-
DeWitt J, Devereaux B, Chriswell M, et al. Comparison of endoscopic ultrasonography and multidetector computed tomography for detecting and staging pancreatic cancer. Ann Intern Med. 2004;141(10):753-763.
-
Fujita A, Ryozawa S, Mizuide M, et al. Diagnosis of pancreatic solid lesions, subepithelial lesions, and lymph nodes using endoscopic ultrasound. J Clin Med. 2021;10(5):1076.
-
Zakaria A, Al-Share B, Klapman JB, Dam A. The role of endoscopic ultrasonography in the diagnosis and staging of pancreatic cancer. Cancers (Basel). 2022;14(6):1373.
-
Nawaz H, Fan CY, Kloke J, et al. Performance characteristics of endoscopic ultrasound in the staging of pancreatic cancer: a meta-analysis. JOP. 2013;14(5):484-497.
-
Yang R, Lu M, Qian X, et al. Diagnostic accuracy of EUS and CT of vascular invasion in pancreatic cancer: a systematic review. J Cancer Res Clin Oncol. 2014;140(12):2077-2086.
-
Barat M, Aldhaheri R, Dohan A, et al. Utility of CT to differentiate pancreatic parenchymal metastasis from pancreatic ductal adenocarcinoma. Cancers (Basel). 2021;13(13):3103.
-
Pietryga JA, Morgan DE. Imaging preoperatively for pancreatic adenocarci- noma. J Gastrointest Oncol. 2015;6(4):343-357.
-
Hashemzadeh S, Mehrafsa B, Kakaei F, et al. Diagnostic accuracy of a 64-Slice multi-detector CT scan in the preoperative evaluation of periampullary neoplasms. J Clin Med. 2018;27;7(5):91.
-
Karmazanovsky G, Fedorov V, Kubyshkin V, Kotchatkov A. Pancreatic head cancer: accuracy of CT in determination of resectability. Abdom Imaging. 2005;30(4):488-500.
-
Zhang YJ, Huang J, Chen MS, Jiao LR. Preoperative vascular evaluation with computed tomography and magnetic resonance imaging for pancreatic cancer: a meta-analysis. Pancreatology. 2012;12(3):227-233.
-
Tellez-Avila FI, Chavez-Tapia NC, López-Arce G, et al. Vascular invasion in pancreatic cancer: predictive values for endoscopic ultrasound and computed tomography imaging. Pancreas. 2012;41(4):636-638.
-
Buchs NC, Chilcott M, Poletti PA, Buhler LH, Morel P. Vascular invasion in pancreatic cancer: imaging modalities, preoperative diagnosis and surgical management. World J Gastroenterol. 2010;16(7):818-831.
-
Yamada M, Sugiura T, Okamura Y, et al. Microscopic venous invasion in pancreatic cancer. Ann Surg Oncol. 2018;25(4):1043-1051.
-
Tseng DS, van Santvoort HC, Fegrachi S, et al. Diagnostic accuracy of CT in assessing extra-regional lymphadenopathy in pancreatic and peri-ampullary cancer: a systematic review and meta-analysis. Surg Oncol. 2014;23(4):229-235.
Tables
Table 1. The diagnostic accuracy of imaging methods for major vascular invasion
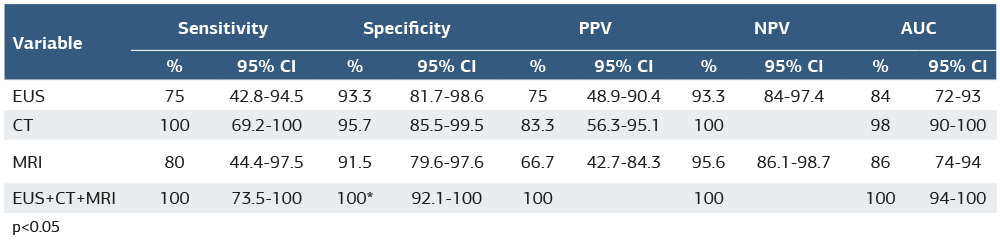
p<0.05
Table 2. The diagnostic accuracy of imaging methods for lymphadenopathy
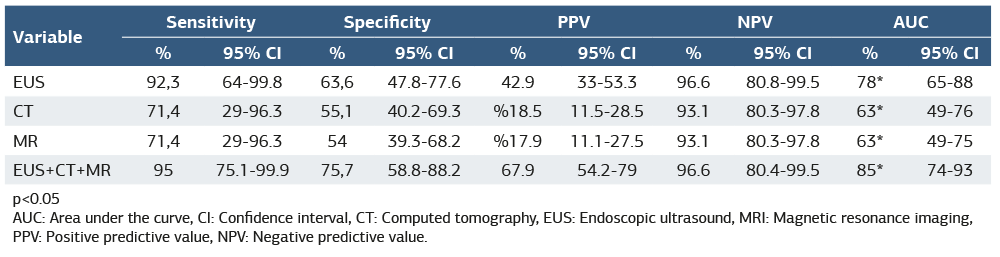
p<0.05 AUC: Area under the curve, CI: Confidence interval, CT: Computed tomography, EUS: Endoscopic ultrasound, MRI: Magnetic resonance imaging, PPV: Positive predictive value, NPV: Negative predictive value.
Table 3. Simple linear regression analysis results regarding pathological dimension
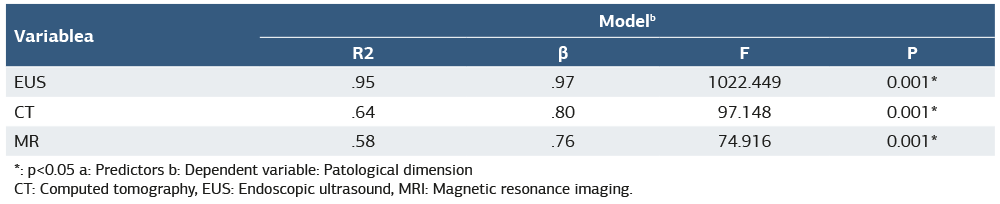
*: p<0.05 a: Predictors b: Dependent variable: Patological dimension CT: Computed tomography, EUS: Endoscopic ultrasound, MRI: Magnetic resonance imaging.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Adnan Kuvvetli, Mustafa Oguz Tugcan, Begum Seyda Avci, Onder Yesiloglu, Yeliz Simsek, Ahmet Burak Urfalioglu, Erdem Aksay, Mustafa Avsar, Alper Parlakgumus, Akkan Avci. Comparing the sensitivity of imaging methods when detecting tumor size in periampullary region tumors: A diagnostic accuracy. Ann Clin Anal Med 2026;17(Suppl 2):S109-113. doi: 10.4328/ACAM.22632
- Received:
- March 4, 2025
- Accepted:
- May 26, 2025
- Published Online:
- July 14, 2025