
The use of bispectral index for monitorization of the depth of sedation in procedural sedoanalgesia in the emergency department
Bispectral Index for monitorization of the depth of sedation
Authors
Abstract
Aim To determine the effectiveness of the Bispectral Index (BIS) measurement as an objective criterion for measuring the depth of sedation in the emergency department (ED) by comparing it with the Modified Ramsey Sedation Scale (MRSS), which is a clinical scale for measuring sedation depth.
Methods In this study, the compatibility of BIS values and MRSS values at the moment when the patients reached clinically appropriate sedation depth for intervention in those requiring sedation-analgesia in the ED due to extremity trauma were compared.
Results No statistically significant correlation was found between patients’ initial MRSS scores at the time of intervention and either their initial or minimum BIS values (p > 0.05). A moderate negative correlation (r = -0.432, p = 0.022) was observed between the MRSS values and the minimum BIS readings. No statistically significant difference was observed in minimum BIS values based on the sedative agent administered (p > 0.05).
Conclusion In this study, a moderate correlation was found between the lowest BIS values and the MRSS scores corresponding to those BIS values. Although further comprehensive and detailed studies are necessary to establish the limitations and optimal use of BIS monitoring during procedural sedation-analgesia in the ED—especially considering both existing literature and the limitations of this study—BIS appears to be a promising alternative to clinical sedation scales for monitoring sedation depth.
Keywords
Introduction
Procedural sedation and analgesia (PSA) is a fundamental practice frequently used in emergency departments (EDs) and improves comfort for both patients and physicians. Reducing pain and anxiety shortens the time required for diagnostic and therapeutic interventions and increases the success rate.1 While over-sedation carries risks such as excessive sedation, respiratory depression, decreased protective airway reflexes, vomiting, and aspiration, under-sedation may lead to inadequate pain and anxiety control during procedures.2,3 Therefore, PSA monitoring is important for a safe, effective, and comfortable intervention.4,5 Subjective scales such as the Modified Ramsey Sedation Scale (MRSS) are still commonly used in monitoring the depth of sedation.6
Bispectral Index (BIS) monitoring allows objective measurement of sedation depth with numerical data obtained through electroencephalographic measurements of the frontal lobe using noninvasive electrodes placed on the patient’s forehead.7 It has long been used in operating rooms as an objective tool for assessing sedation depth. There are studies in the literature showing that it correlates well with clinical sedation scores.8,9 However, limited data are available regarding the use of BIS for PSA in the ED.
PSA is a routine practice in EDs that improves comfort for both patients and physicians. Reducing pain and anxiety shortens the duration of diagnostic and therapeutic procedures and increases success rates. However, over-sedation carries risks such as respiratory depression, decreased airway reflexes, vomiting, and aspiration, while under-sedation may result in inadequate analgesia and anxiety control. Therefore, appropriate PSA monitoring is essential for safe and effective interventions.
This study aimed to compare the MRSS, a more commonly used but subjective method for monitoring sedation depth in the ED, with BIS monitoring, which provides an objective assessment based on numerical data.
Materials and Methods
Our study was designed as a prospective observational study. It was conducted in the Department of Emergency Medicine, Kartal Dr. Lutfi Kirdar City Hospital, Istanbul, between 01.01.2017 and 01.01.2019. Adults aged 18 years and older who underwent PSA for traction and reduction due to limb fracture or dislocation were included, and BIS values and MRSS scores were evaluated. MRSS was preferred as it is the most commonly used scale to monitor sedation depth in our ED. Patients with conditions that could affect consciousness—such as intellectual disability, dementia, cranial tumors, cerebrovascular disease, or head trauma; patients with a baseline Glasgow Coma Score <15; patients under the influence of drugs; those incompatible with BIS electrodes; those who declined participation; and pregnant patients—were excluded from the study.
Study Protocol and MeasurementsThe pulse, blood pressure, and oxygen saturation of all patients were continuously monitored before and during PSA. During PSA, the interventional procedure was performed by an orthopedic surgeon, while an emergency medicine physician administered sedoanalgesia and monitored the patient. Physicians and other healthcare professionals involved in the procedure were blinded to BIS monitoring. The choice of sedative and analgesic drugs was left to the discretion of the ED physician, in accordance with clinical protocols. During the study, practitioners used midazolam, propofol, and ketamine as sedatives, and tramadol and fentanyl as analgesics. The researcher did not interfere with treatment and was responsible for video recording the procedure and documenting the data on a pre-prepared form. BIS values were monitored by the researchers. MRSS and BIS values were recorded during the intervention. The time when adequate sedation was achieved at the start of PSA, and the lowest MRSS and BIS values observed throughout the procedure were noted. MRSS and BIS values were compared based on the American Society of Anesthesiologists’ sedation depth definitions.7 Procedure-related complications (e.g., vomiting, aspiration, use of a bag-valve mask, or intubation due to respiratory depression) were also recorded. Patients were monitored until they were clinically awake and BIS values returned to baseline. Vital signs were measured using Nihon Kohden Life Scope VS BSM-3000 series bedside monitors, and BIS values were measured with BIS VISTATM Monitor Systems.
Ethical ApprovalThis study was approved by the Ethics Committee of Kartal Dr. Lütfi Kırdar City Hospital (Date: 2016-07-29, No: 2016/514/88/10).
Statistical AnalysisThe NCSS (Number Cruncher Statistical System) 2007 (Kaysville, Utah, USA) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, first quartile, third quartile, frequency, percentage, minimum, maximum) were applied to evaluate the data. The conformity of quantitative data to normal distribution was tested using the Shapiro–Wilk test and graphical analysis. The Kruskal–Wallis test and Dunn–Bonferroni post-hoc test were used to compare BIS values across sedative agents. Pearson correlation analysis was used to assess relationships between quantitative variables. A p-value less than p<0.05 was considered statistically significant. To determine the sample size, power analysis was performed using the G*Power (v3.1.9.2) program. Based on the study by Gill et al., which found a correlation of -0.690 between RSS and BIS, it was calculated that at least 14 subjects would be required to detect a correlation at this level with 80% power at α = 0.05. A total of 28 cases were included in the study.
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
A total of 28 patients were included in the study, of whom 15 (53.6%) were women and 13 (46.4%) were men. The ages of the patients ranged from 18 to 89 years, with a mean age of 47.07 ± 22.78 years. The demographic and clinical characteristics of the patients evaluated for the use of BIS in monitoring sedation depth during PSA in the ED are as follows: 53.6% (n=15) of the patients had fractures, 28.6% (n=8) had dislocations, 3.6% (n=1) had a combination of fracture and dislocation, and 14.2% (n=4) underwent fixation-traction using a Steinmann pin.
Regarding the sedative agents used, the most common combination was ketamine and propofol, administered to 67.9% (n=19) of the patients. Midazolam was used in 14.2% (n=4), ketamine alone in 10.8% (n=3), and propofol alone in 7.1% (n=2) of the cases.
The BIS and MRSS values recorded during the PSA procedure are presented in Table 1.
In terms of the relationship between MRSS and BIS values, no statistically significant correlation was observed between the initial MRSS scores and both the initial and minimum BIS values (p > 0.05). Similarly, no significant correlation was found between the MRSS scores at minimum BIS and the initial BIS values of the intervention (p > 0.05). However, a moderate negative correlation was identified between the MRSS scores at minimum BIS and the minimum BIS values (r = -0.432, p = 0.022) (Table 2). A statistically significant difference was found in the initial BIS values across the different agents (p = 0.027). According to the Dunn–Bonferroni post-hoc test, the initial BIS values in patients who received midazolam were significantly lower than those who received ketamine (p = 0.037). No statistically significant differences were observed between the remaining agents (p > 0.05). Additionally, no significant difference was found in the minimum BIS values based on the sedative agent used (p > 0.05) (Table 3). During the PSA procedure, one patient who was administered midazolam had respiratory depression and recovered with the bag valve mask support. Nausea occurred in 2 patients who received ketamine, and no other complications were observed.
Discussion
In this study, we investigated the relationship between BIS and MRSS scores to assess sedation depth in patients undergoing PSA. Our findings revealed a moderate negative correlation between MRSS and minimum BIS values, while no statistically significant associations were observed among other parameters. In comparisons based on sedative agents, initial BIS values were lower in patients who received midazolam compared to those who received ketamine. No major complications occurred during PSA; only mild and transient side effects were observed. These results suggest that the combined use of BIS and MRSS may contribute to safer and more effective sedation monitoring. Subjective clinical tools such as MRSS, the Richmond Agitation-Sedation Scale, and the Observer’s Assessment of Alertness/ Sedation Scale are commonly used to assess sedation depth during PSA.10 BIS, by contrast, enables objective evaluation through electroencephalographic measurements obtained noninvasively via electrodes placed on the patient’s forehead.11,12 Although BIS has been widely studied in operating rooms and intensive care units,13 data on its use in ED-based PSA remains limited. A small number of studies suggest that BIS may serve as a useful objective tool in this contex.14,15 In our country, 1000–2000 patients are admitted to EDs daily, often under limited staffing conditions. This high workload highlights the need for objective tools. Early detection and timely intervention of complications are possible with simple monitoring techniques.16 We believe that in crowded EDs, BIS-derived numerical data may facilitate clinical decision-making and prevent complications associated with excessive sedation. With this study, we aimed to demonstrate the compatibility of BIS with clinical scoring systems. We observed a moderate correlation between BIS values and MRSS. Numerous studies in the literature have compared BIS with clinical sedation scales in ICU and OR settings.17,18 We found no significant difference in minimum BIS values across sedative agents used in the ED. Abouelela et al. evaluated BIS in mechanically ventilated ICU patients, and Zheng et al. explored its correlation with the Richmond Scale during flexible bronchoscopy; both studies reported significant associations.8,19 Shetty et al., in a systematic review, concluded that there is not yet enough evidence to establish the superiority of BIS over clinical scales in critically ill patients on mechanical ventilation.13
Few studies have been conducted specifically in EDs. Gill et al. compared MRSS and BIS during PSA and reported a correlation between the two methods.20 They excluded patients given ketamine due to previously reported inconsistencies in BIS readings with dissociative agents. In contrast, we included patients who received ketamine, as it is a frequently used PSA agent and does not cause hypotension. While initial BIS values differed by agent (lower in midazolam recipients), minimum BIS values showed no significant difference. In a study by Agrawal et al., BIS and MRSS were compared in 20 pediatric ED patients undergoing PSA, and a strong correlation was found.21 Avcı et al. also reported a high correlation between RSS and BIS in ED-based PSA patients.9
Although most BIS-related studies focus on ICU settings, ED studies indicate that BIS may support early recognition of complications during PSA, especially in resource-limited environments.11 In addition, recent research by Çınaroğlu et al. (2024) demonstrated that near-infrared spectroscopy (NIRS), a non-invasive spectrophotometric method, can effectively aid in the early diagnosis of intracranial hemorrhage in emergency department settings. This supports the potential of integrating NIRS and BIS as complementary technologies for objective patient monitoring in the ED.22
In our study, the lowest BIS value recorded was 47, and the patient in question required bag-valve mask ventilation due to shallow breathing. Nevertheless, our findings are not sufficient to confirm the superiority of BIS over clinical assessment tools. Previous studies generally involved non-dissociative sedatives. Our study is distinct in that it included patients receiving ketamine+propofol and ketamine alone. Unfortunately, the number of patients who received only ketamine, a dissociative agent, was limited, preventing us from drawing definitive conclusions. Larger studies are needed to evaluate the reliability of BIS monitoring in ketamine sedation.
In our study, sedative drug selection was left to the discretion of the treating physician, and no standardization was imposed. Patients who received only midazolam had lower BIS values than those given ketamine, but no significant differences were observed for other agents. Future studies should explore sedation depth differences between dissociative and non-dissociative drugs by forming standardized treatment groups.
Limitations
PSA practitioners in this study did not follow a standardized protocol for sedation and analgesia agents. Additionally, although clinical evaluation tools are based on structured scoring systems, they are inherently subjective and open to individual interpretation. This study aimed to propose a more objective assessment method; however, the subjectivity of clinical scales may have limited the clarity of the findings. The study was conducted in a crowded ED, where a dedicated procedural area was not available. As a result, external environmental stimuli may have influenced BIS measurements.
Conclusion
A moderate correlation was found between MRSS and BIS values in patients undergoing sedation and analgesia in the ED. BIS monitoring appears to be a valuable tool for assessing sedation depth during PSA in the ED. However, randomized controlled trials are necessary to establish stronger evidence, particularly regarding the use of different sedative agents.
Declarations
Ethics Declarations
Ethical approval for this study was obtained from the Ethics Committee of Kartal Dr. Lütfi Kırdar City Hospital (Date: July 29, 2016; Decision No: 2016/514/88/10). It was conducted in accordance with the principles of the Declaration of Helsinki, and informed consent was obtained from all participants.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.G., S.Y.
Methodology: E.G., F.S.D., S.Y.
Investigation: E.G., F.S.D.
Data curation: E.G.
Formal analysis: E.G., S.Y.
Writing – original draft: E.G.
Writing – review & editing: F.S.D., S.Y.
Supervision: S.Y.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
BIS: Bispectral Index
ED: Emergency Department
EEG: Electroencephalography
GCS: Glasgow Coma Score
ICU: Intensive Care Unit
MRSS: Modified Ramsey Sedation Scale
NIRS: Near-Infrared Spectroscopy
OR: Operating Room
PSA: Procedural Sedation and Analgesia
References
-
Mathew B. Effectiveness of psychological intervention package on anxiety and wellness level among patients with anxiety disorders. J Family Med Prim Care. 2022;11(11):6704-6713. doi:10.4103/jfmpc.jfmpc_561_21
-
Godwin SA, Burton JH, Gerardo CJ, et al. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63:247-258.e18.
-
O’Connor RE, Sama A, Burton JH, et al. Procedural sedation and analgesia in the emergency department: recommendations for physician credentialing, privileging, and practice. Ann Emerg Med. 2011;58(4):365-370. doi:10.1016/j.annemergmed.2011.06.020
-
Cappellini I, Bavestrello Piccini G, Campagnola L, et al. Procedural Sedation in Emergency Department: A Narrative Review. Emerg Care Med. 2024; 1(2):103- 136
-
AK R, Tatliparmak AC, Yilmaz S. Enhancing prehospital analgesia: addressing methodological concerns and proposing the START-A mnemonic. Scand J Trauma Resusc Emerg Med. 2024;32(1):52. doi:10.1186/s13049-024-01220-2
-
Sachdeva A, Jaswal S, Walia HS, Batra YK. Correlating the Depth of Sedation Between the Ramsay Sedation Scale and Bispectral Index Using Either Intravenous Midazolam or Intravenous Propofol in Elderly Patients Under Spinal Anaesthesia. Cureus. 2023;15:e50763.
-
Oliveira CR, Bernardo WM, Nunes VM. Benefit of general anesthesia monitored by bispectral index compared with monitoring guided only by clinical parameters. Systematic review and meta-analysis. Braz J Anesthesiol. 2017;67(1):72-84. doi:10.1016/j.bjane.2015.09.001
-
Zheng J, Gao Y, Xu X, et al. Correlation of bispectral index and Richmond agitation sedation scale for evaluating sedation depth: a retrospective study. J Thorac Dis. 2018;10:190–195.
-
Avci S, Bayram B, Inanç G, et al. Evaluation of the compliance between EEG monitoring (Bispectral IndexTM) and Ramsey Sedation Scale to measure the depth of sedation in the patients who underwent procedural sedation and analgesia in the emergency department. Ulus Travma Acil Cerrahi Derg. 2019;25:447–452.
-
Lim TW, Choi YH, Kim JY, et al. Efficacy of the bispectral index and Observer’s Assessment of Alertness/Sedation Scale in monitoring sedation during spinal anesthesia: A randomized clinical trial. J Int Med Res. 2020;48(4):300060519893165.
-
Conway A, Sutherland J. Depth of anaesthesia monitoring during procedural sedation and analgesia: A systematic review and meta-analysis. Int J Nurs Stud. 2016;63 (1):201–212.
-
Bouafif L. Monitoring of Anesthesia by Bispectral Analysis of EEG Signals. Comput Math Methods Med. 2021;2021 (1):996-998.
-
Shetty RM, Bellini A, Wijayatilake DS, et al. BIS monitoring versus clinical assessment for sedation in mechanically ventilated adults in the intensive care unit and its impact on clinical outcomes and resource utilization. Cochrane Database Syst Rev. 2018;2:CD011240.
-
Froese L, Dian J, Gomez A, Batson C, Sainbhi AS, Zeiler FA. Association Between Processed Electroencephalogram-Based Objectively Measured Depth of Sedation and Cerebrovascular Response: A Systematic Scoping Overview of the Human and Animal Literature. Front Neurol. 2021;12:692207.
-
Park K, Froese L, Bergmann T, et al. Association Between Clinical Measures of Depth of Sedation and Multimodal Cerebral Physiology in Acute Traumatic Neural Injury. Neurotrauma Rep. 2024;5:916–956.
-
Sessler CN, Jo Grap M, Ramsay MA. Evaluating and monitoring analgesia and sedation in the intensive care unit. Crit Care. 2008;12(Suppl 3):S2.
-
Bagchi D, Mandal MC, Das S, Basu SR, Sarkar S, Das J. Bispectral index score and observer’s assessment of awareness/sedation score may manifest divergence during onset of sedation: Study with midazolam and propofol. Indian J Anaesth. 2013;57:351.
-
Heavner MS, Gorman EF, Linn DD, Yeung SYA, Miano TA. Systematic review and meta-analysis of the correlation between bispectral index (BIS) and clinical sedation scales: towards defining the role of BIS in critically ill patients. Pharmacotherapy. 2022;42(8):667–676.
-
Abouelela A, Abdelazim MS. A comparative study between the bispectral index and the clinical score in the evaluation of sedation level in critically ill, mechanically ventilated patients. Indian J Anaesth. 2013;57(4):351-357.
-
Gill M, Green SM, Krauss B. A study of the Bispectral Index Monitor during procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2003;41(2):234-241.
-
Agrawal D, Feldman HA, Krauss B, Waltzman ML. Bispectral index monitoring quantifies depth of sedation during emergency department procedural sedation and analgesia in children. Ann Emerg Med. 2004;43(2):247-255.
-
Çınaroğlu OS, Bora ES, Acar H, Arıkan C, Küçük M, Kırık S. Is near-infrared spectroscopy a promising predictor for early intracranial hemorrhage diagnosis in the Emergency Department?. Braz J Med Biol Res. 2024;57:e13155.
Tables
Table 1. Bispectral index monitoring and Modified Ramsey Sedation Scale values of the patients
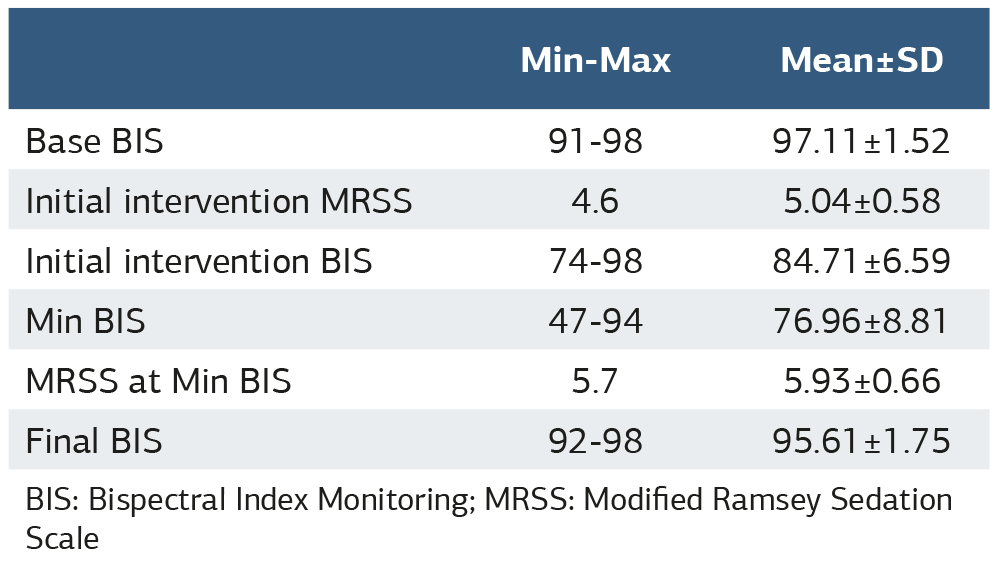
BIS: Bispectral Index Monitoring; MRSS: Modified Ramsey Sedation Scale
Table 2. The relationship between bispectral index monitoring and Modified Ramsey Sedation Scale values
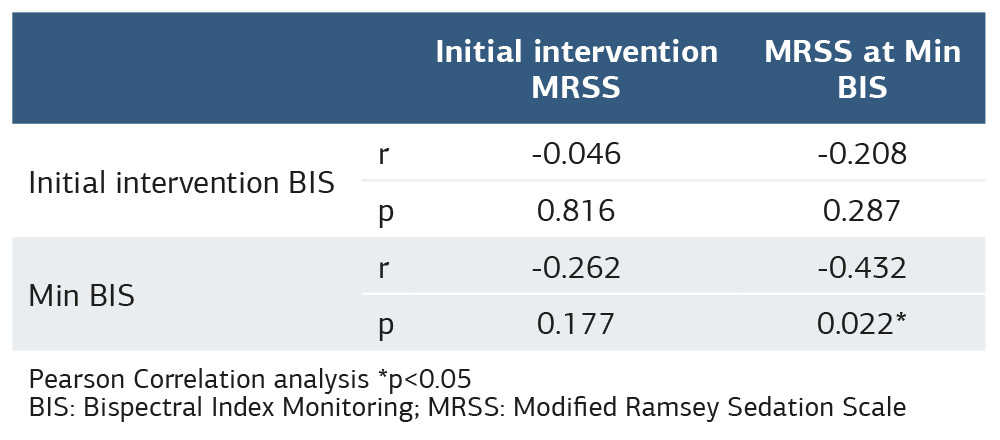
Pearson Correlation analysis *p<0.05 BIS: Bispectral Index Monitoring; MRSS: Modified Ramsey Sedation Scale
Table 3. Comparison of bispectral index monitoring values according to sedative agent
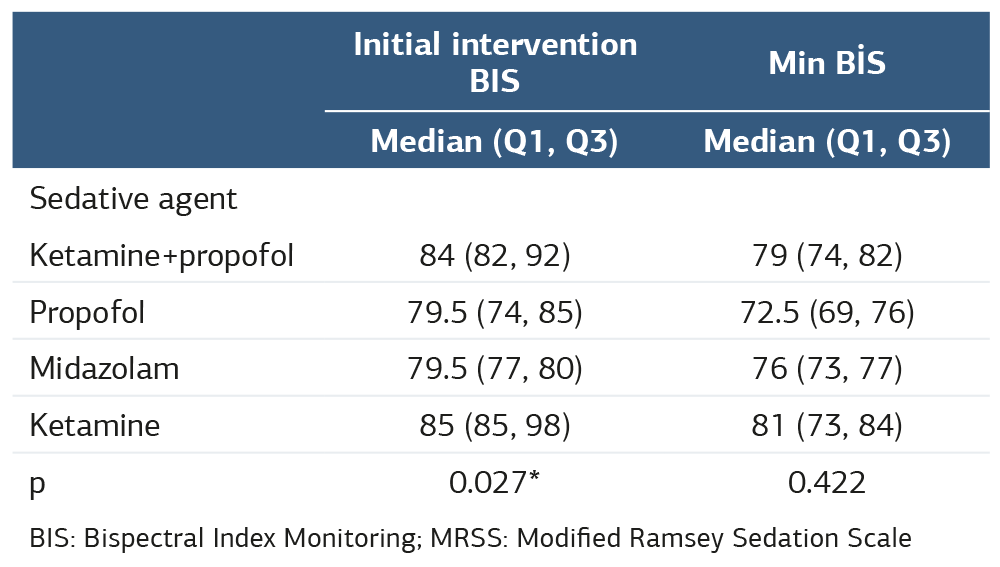
BIS: Bispectral Index Monitoring; MRSS: Modified Ramsey Sedation Scale
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Eren Gökdağ, Fatma Sarı Doğan, Sarper Yılmaz. The use of bispectral index for monitorization of the depth of sedation in procedural sedoanalgesia in the emergency department. Ann Clin Anal Med 2026;17(Suppl 2):S119-123. doi: 10.4328/ACAM.22682
- Received:
- March 29, 2025
- Accepted:
- May 12, 2025
- Published Online:
- June 4, 2025
- Printed:
- March 20, 2026