
Importance of serum albumin levels in cardiovascular events
Albumin and cardiovascular events
Authors
Abstract
Cardiovascular diseases are among the leading causes of death worldwide. Inflammatory conditions, endothelial dysfunction and oxidative stress play a role in the onset and/or development of many cardiovascular diseases, especially heart failure and coronary artery disease. Serum albumin has many physiological functions, including anti-inflammatory, antioxidant, anti-platelet aggregation activity and anticoagulant. It is also critical for fluid exchange across the capillary membrane. Serum albumin performs binding and transport functions for many substances such as hormones, fatty acids, steroids, inorganic ions, vitamins and drugs. Albumin has important links with inflammation and cardiac events. Decreased SA levels are associated with myocardial infarction, atrial fibrillation, heart failure and coronary heart disease. This is because a decrease in serum albumin levels, i.e. hypoalbuminemia, plays a role in impairments in vasodilatory ability and anticoagulation, fibrinolysis, vascular permeability and increased blood viscosity. Hypoalbuminemia will lead to decreased antioxidant levels in plasma and trigger cardiovascular diseases due to decreased antioxidant levels. The aim of this review is to provide an overview of the relationship between serum albumin and cardiovascular diseases.
Keywords
Introduction
Cardiovascular diseases (CVD) are among the leading causes of death worldwide. Inflammatory conditions, endothelial dysfunction and oxidative stress play a role in the onset and/or development of many CVDs, especially heart failure and coronary artery disease. Serum albumin (SA) has many physiological functions, including anti-inflammatory, antioxidant, anti-platelet aggregation activity and anticoagulant. It is also critical for fluid exchange across the capillary membrane.1
The most prominent known activities of SA include regulating fluid distribution between vascular compartments and maintaining plasma oncotic pressure. Albumin is the most abundant protein in the blood. It is not possible to isolate a single function of SA. Because most of its functions are interrelated and play a role in maintaining homeostasis. The reference range of SA in an adult human is 3.5-5 g/dl. However, the pathologic limit may differ according to the tests used. SA levels are lower in women than in men. It tends to decrease with age.2
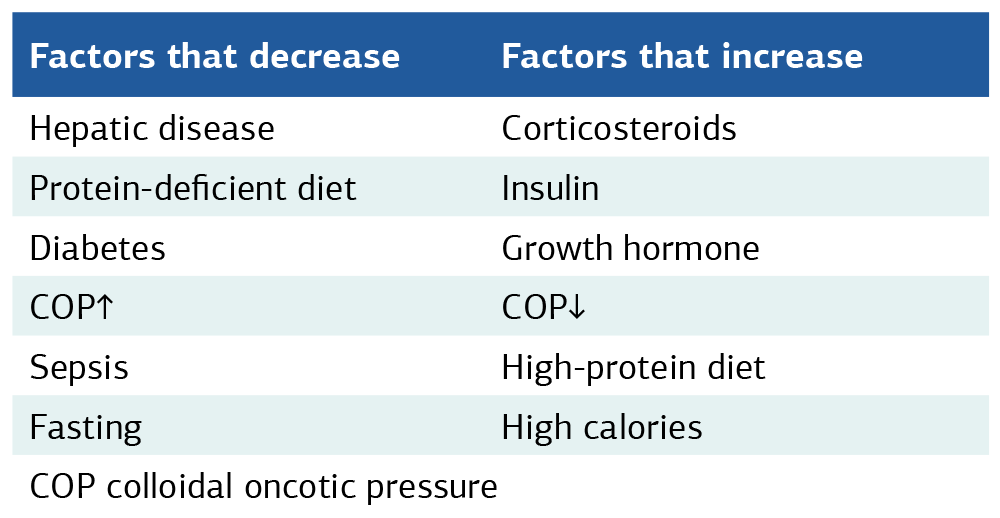
Synthesis and Biological Functions of AlbuminAlbumin is synthesized from hepatocytes. It is synthesized at a rate of almost 150 mg/kg/day.3 Albumin synthesized in hepatocytes is transferred to the extracellular space by exocytosis. Approximately 2/5 is found intravascularly. 3/5 is transferred to the interstitial spaces of organs and tissues, especially muscle, connective tissue, adipose tissue and skin.3,4 There is albumin activity between the interstitial-intravascular spaces via lymphatic vessels. Albumin concentration is high in plasma. The high concentration, together with a strong negative net charge, maintains the plasma oncotic pressure. Albumin in serum is higher than albumin in the interstitial space.5 For example, concentrations of about 13 g/L in skeletal muscle and about 7 g/L in adipose tissue have been described.6 The level of synthesis of albumin varies according to the osmolality of the hepatic extravascular space, differences in colloid osmotic pressure and the body’s requirements (Table 1).7
SA performs binding and transport functions for many substances such as hormones, fatty acids, steroids, inorganic ions, vitamins and drugs.8 It has also been reported to maintain the permeability of capillaries. Low albumin levels have been reported to impair the vasodilator response to nitric oxide. It has antioxidant functions against oxidative stress involved in the pathogenesis of atherosclerosis.9
Types of AlbuminAlbumin can be obtained from many sources. These include rat serum albumin (RSA), human serum albumin (HSA) (Figure 1), bovine serum albumin (BSA) and ovalbumin (egg white, OVA). However, HSA10 and BSA are the most preferred in drug delivery.
Albumin is a negatively charged protein composed of 585 amino acids that form a single polypeptide chain with a molecular weight of 66.5 kDa (Figure 1). It is organized as a series of α-helices stabilized by 17 disulfide bonds. It consists of three homologous domains (I-III). These domains have two subdomains (A and B) and each domain consists of 4 and 6 α-helices. Albumin in solution is characterized by a flexible texture thanks to disulfide bonds. An unbound cysteine residue (Cys-34) in subdomain IA is a redox active thiol (-SH) group. The thiol moiety includes thiolation (HSA-SR), nitrosylation (HSA-S-NO) and the ability to bind substances.8 Albumin has an average half-life of 19 days. PH range is between 4-9. It can be heated at 60 °C for 10 hours.10 BSA has a molecular weight of 69,323 kDa. It has an isoelectric point of 4.7 in water at 25 °C. This property makes it negatively charged at neutral pH and positively charged at acidic pH.11,12 This creates binding conditions for both negatively and positively charged substances. BSA is generally preferred for drug delivery. Because it is cost effective, easy to control and purify. It can also bind hydrophobic and hydrophilic drugs, is water soluble and has the capacity to overload. The only possible undesirable situation is that it may cause an in vivo immunogenic response in humans.13
Albumin and Cardiovascular DiseaseAlbumin is believed to have important links with inflammation and cardiac events. It has also been suggested to have some commonalities with factors that aggravate CVDs.14 Therefore, a number of studies have been conducted to fully explain the link between CVD and SA. SA reference range is 3.5-5 g/dl.15 A value below 3.5 g/dl (< 3.5 g/dl) is called hypoalbuminemia. However, there is no clear definition to explain the relationship between SA level and the prediction of cardiovascular adverse events. Recent studies have shown that cardiovascular risks are increased even within the SA reference range (3.5-4.0 g/dL).16 Furthermore, in patients hospitalized for acute myocardial infarction (AMI), a serum albumin level < 3.8 g/dl has been described as an independent predictor of cardiac events.17,18
Hypoalbuminemia is recognized as a new and critically important marker for coronary artery disease (CAD). Furthermore, hypoalbuminemia is associated with elevated total and low-density lipoprotein (LDL) cholesterol levels and increased risk of CVD mortality.1 Hypoalbuminemia is also associated with impairments in vasodilatory ability and anticoagulation, fibrinolysis, increased vascular permeability and blood viscosity (Figure 2). Increases in these factors also increase the risk of CVD.9,19
Previous studies have shown that a decrease in SA levels is associated with myocardial infarction,18 atrial fibrillation,19 heart failure20 and coronary heart disease (Figure 3).21 This is because hypoalbuminemia will cause a decrease in antioxidant levels in plasma. It has been suggested that decreased antioxidant levels and CVDs are associated with each other.2
Ethics ApprovalNot applicable. This article is a narrative review of previously published studies and does not involve new data collection from human participants or animals.
Statistical AnalysisNot applicable. No new statistical analysis was performed in this narrative review.
Reporting GuidelinesThis article is a narrative review of previously published literature. No specific reporting guideline was applicable.
Discussion
When the study data were evaluated, it was explained that, independent of inflammation and risk factors, hypoalbuminemia was linked to the occurrence of many CVDs, including heart failure, ischemic heart disease, AF and venous thromboembolism.14 8870 people without CVD were followed for 8 years. Hypoalbuminemia was linked to the occurrence of AF in women, independent of new-onset heart failure, heart disease and inflammation.19,20,21,22 In a study of 12,833 individuals followed for 25. 1 years to assess the prospective relationship between serum albumin and AF risk, it was concluded that the effect of serum albumin on AF is widespread. There is no evidence that increasing serum albumin levels (albumin infusion, dietary improvement, etc.) attenuates the clinical risk of AF. However, measurement of serum albumin is performed by an inexpensive and routinely available blood test. Therefore, if serum albumin is shown to contribute to the prevention of AF, a very important clinical benefit would be achieved.23 Elevated serum albumin levels may be protective in cardiovascular events. In a study in which < 3.8 g/dL was considered a low SA level, among 289 AMI patients in the acute phase of AMI, 194 AMI patients improved in the chronic phase with SA levels ≥ 3.8 g/dL. This improved subgroup had better outcomes than the non-improved subgroup.24 However, it remains unclear whether the higher the albumin levels, the better the prognosis for CVD.15
In a study of 352 patients with chronic heart failure, low serum albumin was associated with elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels and increased long-term mortality.25 Low serum albumin has also been shown to be an independent predictor of short- and long-term events in patients with acute heart failure. Another study for 546 patients with non-ischemic acute heart failure reported that low serum albumin on admission was an independent predictor of adverse cardiac events.26 In a 708-day study of 204 patients with chronic coronary syndrome, they proved that low serum albumin predicts adverse cardiovascular events, including myocardial infarction (MI), all-cause mortality and stroke.27 In a prospective study involving > 100,000 individuals, an inverse relationship between plasma albumin and CVD was reported, which was attributed to the fact that albumin is a negative acute phase reactant.28 An albumin value ≤ 3.2 g/dL was found to be a critical predictor of in-hospital mortality in elderly patients hospitalized for acute HF.29 A cross-sectional study described that SA density was inversely associated with the incidence of peripheral arterial disease (PAD) in hemodialysis patients.30 In fact, results from the HEMO study, which enrolled 1411 hemodialysis patients, reported that CVD risk increased as albumin levels decreased in patients with SA concentrations ≥ 3.6 g/dL. For every 1 g/dL increase in SA, the odds ratio decreased by 68% for CAD, 67% for CVD, 61% for PAD and 77% for all atherosclerotic diseases.31 In the Cardiovascular Health Study, 5450 healthy individuals aged ≥ 65 years were enrolled. Hypoalbuminemia has been shown to be significantly associated with HF within 10 years.32
Limitations
This narrative review is based on previously published studies and does not include a systematic search or quantitative synthesis. Therefore, the findings reflect associations reported in the literature and do not establish causality.
Conclusion
The SA level has evolved as an indicator of nutritional and inflammatory status and has been described to predict CVD prognosis. Further and extensive studies on the pathophysiology of albumin levels are needed to fully explain the relationship between albumin levels and adverse events in CVD patients.15
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Not applicable.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: Y.H.
Methodology: Y.H.
Investigation: Y.H.
Data Curation: Y.H.
Writing – Original Draft Preparation: Y.H.
Writing – Review & Editing: Y.H.
Visualization: Y.H.
Supervision: Y.H.
Abbreviations
ACE: Angiotensin-Converting Enzyme
ACS: Acute Coronary Syndrome
AF: Atrial Fibrillation
AMI: Acute Myocardial Infarction
BMI: Body Mass Index
CAD: Coronary Artery Disease
CRP: C-Reactive Protein
CVD: Cardiovascular Disease
HDL: High-Density Lipoprotein
IL-6: Interleukin-6
LDL: Low-Density Lipoprotein
MI: Myocardial Infarction
NYHA: New York Heart Association
ROS: Reactive Oxygen Species
TNF-α: Tumor Necrosis Factor Alpha
References
-
Arques S. Serum albumin and cardiovascular disease: state-of-the-art review. Ann Cardiol Angeiol (Paris). 2020;69(4):192-200. 10.1016/j.ancard.2020.07.012
-
Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8-12. 10.1016/j.ejim.2018.04.014
-
Carvalho JR, Verdelho Machado M. New insights about albumin and liver disease. Ann Hepatol. 2018;17(4):547-560. doi:10.5604/01.3001.0012.0916
-
Levitt DG, Levitt MD. Human serum albumin homeostasis: a new look at the roles of synthesis, catabolism, renal and gastrointestinal excretion, and the clinical value of serum albumin measurements. Int J Gen Med. 2016;9:229-255. doi:10.2147/IJGM.S102819
-
Evans TW. Review article: albumin as a drug—biological effects of albumin unrelated to oncotic pressure. Aliment Pharmacol Ther. 2002;16(suppl 5):S6-S11. doi:10.1046/j.1365-2036.16.s5.2.x
-
Ellmerer M, Schaupp L, Brunner GA, et al. Measurement of interstitial albumin in human skeletal muscle and adipose tissue by open-flow microperfusion. Am J Physiol Endocrinol Metab. 2000;278(2):E352-E356. doi:10.1152/ajpendo.2000.278.2.E352
-
Wingfield W. Fluid and electrolyte therapy. In: Raffe MR, ed. The Veterinary ICU Book. Jackson, WY: Teton New Media; 2002:166-188.
-
Kragh-Hansen U. Human serum albumin: a multifunctional protein. In: Otagiri M, Chuang VTG, eds. Albumin in Medicine: Pathological and Clinical Applications. Singapore: Springer; 2016:1-24.
-
Chien SC, Chen CY, Lin CF, Yeh HI. Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark Res. 2017;5:31.
-
Larsen MT, Kuhlmann M, Hvam ML, Howard KA. Albumin-based drug delivery: harnessing nature to cure disease. Mol Cell Ther. 2016;4:3. doi:10.1186/s40591-016-0048-8
-
Karimi M, Bahrami S, Ravari SB. Albumin nanostructures as advanced drug delivery systems. Expert Opin Drug Deliv. 2016;13(11):1609-1623. doi:10.1080/17425247.2016.1193149
-
Phan HTM, Bartelt-Hunt S, Rodenhausen KB. Investigation of bovine serum albumin attachment onto self-assembled monolayers using QCM-D and SE. PLoS One. 2015;10(10):e0141282. doi:10.1371/journal.pone.0141282
-
Elzoghby AO, Samy WM, Elgindy NA. Albumin-based nanoparticles as potential controlled release drug delivery systems. J Control Release. 2012;157(2):168-182. doi:10.1016/j.jconrel.2011.07.031
-
Arques S. Serum albumin and cardiovascular diseases: a comprehensive review of the literature. Ann Cardiol Angeiol (Paris). 2018;67(2):82-90.
-
Yoshioka G, Tanaka A, Goriki Y, Node K. The role of albumin level in cardiovascular disease: a review of recent research advances. J Lab Precis Med. 2023;8:7. doi:10.21037/jlpm-22-57
-
Xia M, Zhang C, Gu J, et al. Impact of serum albumin levels on long-term mortality in first-onset AMI. Clin Chim Acta. 2018;477:89-93.
-
Yoshioka G, Tanaka A, Nishihira K, Shibata Y, Node K. Prognostic impact of serum albumin for developing heart failure remotely after AMI. Nutrients. 2020;12(9):2637. doi:10.3390/nu12092637
-
Djousse L, Rothman KJ, Cupples LA, Levy D, Ellison RC. Serum albumin and risk of myocardial infarction. Circulation. 2002;106(23):2919-2924.
-
Liao LZ, Zhang SZ, Li WD, et al. Serum albumin and atrial fibrillation. Eur J Epidemiol. 2020;35(2):113-122.
-
Gopal DM, Kalogeropoulos AP, Georgiopoulou VV, et al. Serum albumin concentration and heart failure risk. Am Heart J. 2010;160(2):279-285.
-
Nelson JJ, Liao D, Sharrett AR, et al. Serum albumin level as predictor of incident coronary heart disease. Am J Epidemiol. 2000;151(5):468-477.
-
Mukamal KJ, Tolstrup JS, Friberg J, Gronbaek M, Jensen G. Fibrinogen and albumin levels and risk of AF. Am J Cardiol. 2006;98(1):75-81.
-
Ronit A, Kirkegaard-Klitbo DM, Dohlmann TL, et al. Plasma albumin and incident cardiovascular disease: results from the CGPS and an updated meta-analysis. Arterioscler Thromb Vasc Biol. 2020;40(2):473-482.
-
Yoshioka G, Tanaka A, Nishihira K, et al. Prognostic impact of follow-up serum albumin after AMI. ESC Heart Fail. 2021;8(6):5456-5465.
-
Yi S, Chen M. Decreased albumin and prognosis in chronic HF. Medicine (Baltimore). 2020;99(51):e23872.
-
Ancion A, Allepaerts S, Oury C, et al. Serum albumin level and hospital mortality in acute HF. ESC Heart Fail. 2017;4(2):138-145.
-
Suzuki S, Hashizume N, Kanzaki Y, et al. Prognostic significance of serum albumin in stable CAD. PLoS One. 2019;14(7):e0219044.
-
Hou X, Li Y, Wang H, et al. The negative association between serum albumin levels and coronary heart disease risk in adults: evidence from NHANES 2011–2018. Sci Rep. 2023;13:27974. doi:10.1038/s41598-023-27974-w
-
Kinugasa Y, Kato M, Sugihara S, et al. Hypoalbuminemia as prognostic factor in acute HF. Circ J. 2009;73(12):2276-2281.
-
O’Hare AM, Hsu CY, Bacchetti P, Johansen KL. Peripheral vascular disease risk factors in hemodialysis. J Am Soc Nephrol. 2002;13(2):497-503.
-
Beddhu S, Kaysen GA, Yan G, et al. Association of serum albumin and atherosclerosis in hemodialysis. Am J Kidney Dis. 2002;40(4):721-727.
-
Filippatos GS, Desai RV, Ahmed MI, et al. Hypoalbuminaemia and incident heart failure in older adults. Eur J Heart Fail. 2011;13(10):1078-1086. doi:10.1093/eurjhf/hfr088
Figures
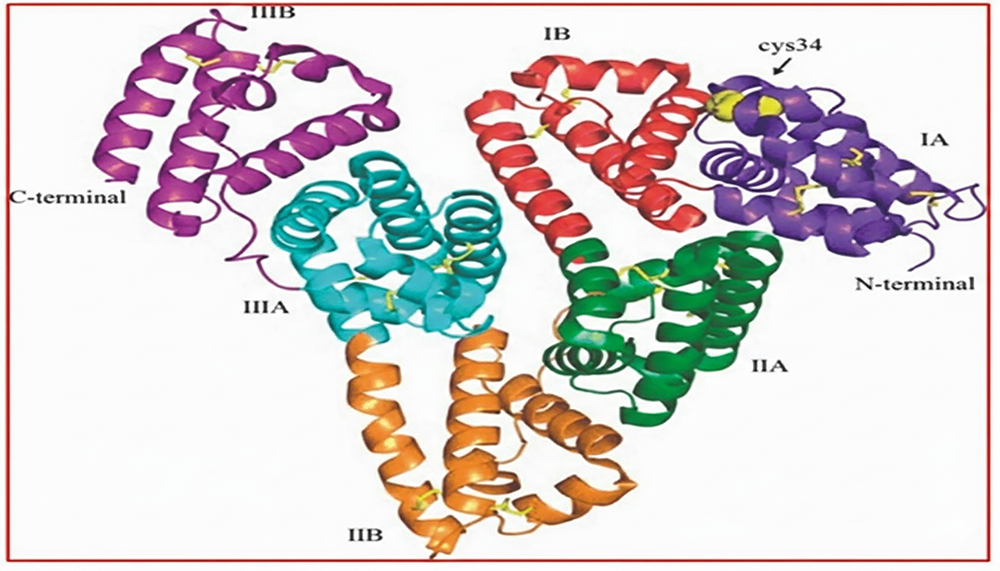
Figure 1. Structure of human serum albumin (A single polypeptide containing 585 amino acids) [11]
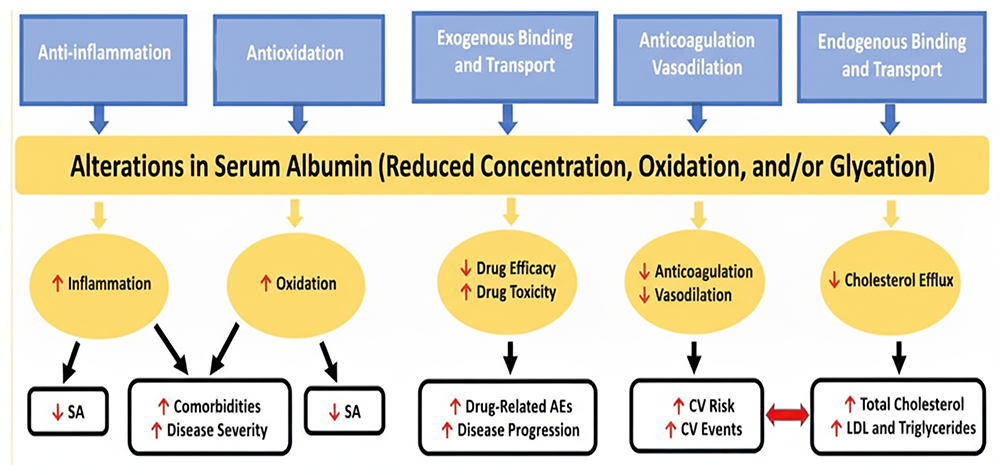
Figure 2. Demonstration of interactive effects between physiological functions of SA, except colloid oncotic pressure. AE, adverse event; CV, cardiovascular; LDL, low-density lipoprotein; SA, serum albumin. [9]
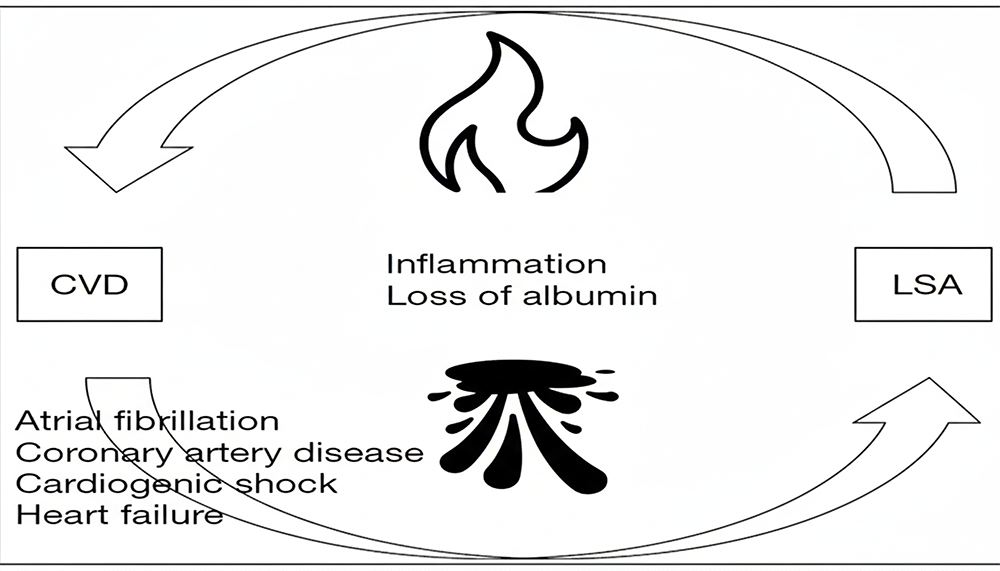
Figure 3. Association between low serum albumin and cardiovascular disease. [15]
Tables
Table 1. Factors that decrease or increase albumin synthesis [9]
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yasemin Hacanlı. Importance of serum albumin levels in cardiovascular events. Ann Clin Anal Med 2026;17(Suppl 1):S84-87. doi:10.4328/ACAM.22337
- Received:
- July 23, 2024
- Accepted:
- August 26, 2024
- Published Online:
- April 30, 2025
- Printed:
- February 20, 2026