
Biofeedback support in stress urinary incontinence the effect of pelvic floor muscle training on muscle activity potential
Muscle activity in incontinence
- Received:
- August 21, 2024
- Accepted:
- October 21, 2024
- Published Online:
- March 5, 2025
- Printed:
- October 1, 2025
Authors
Abstract
Aim The study aims to investigate the effect of biofeedback (BF) assisted pelvic floor muscle training (PFMT) on muscle activity potential in stress urinary incontinence (SUI).
Methods The study included 42 women diagnosed with SUI between the ages of 45-65. Individuals were divided into three groups: PFMT with BF, PFMT alone, and control group. All groups were given medical treatment. The treatment was carried out for 6 weeks and 3 days a week. In the PFMT program, 360-degree diaphragmatic breathing training, dynamic neuromuscular stabilization exercises, and pelvic floor muscle exercises were applied. Electromyography (EMG) evaluation was applied to the participants at the beginning of the program and at the end of the 6th week.
Results No difference was observed between the pre-treatment demographic characteristics and EMG values of the groups. While EMG parameters showed improvement in all groups after treatment. The highest increase in the work average value was in the PFMT + BF group. Peak and maximum voluntary contraction (%) value increases were found to be higher in the training groups compared to the control group, and there was no difference between the training groups.
Conclusion It was found that the PFMT + BF combined treatment method was beneficial in terms of its effect on muscle activity potential in SUI patients.
Keywords
Introduction
Stress urinary incontinence is not a fatal or life-threatening condition, but it is a growing public health problem because it generally has a negative impact on the quality of life and causes physical, social, and emotional problems in the individual 1. There are surgical and conservative methods for the treatment of SUI. Conservative treatment methods include PFMT, BF, electrical stimulation, vaginal cones, bladder training, and dynamic neuromuscular stabilization (DNS). The International Continence Society reports that PFMT should be the first recommended treatment for conservative treatment of SUI. The success rate of PFMT in the treatment of SUI has been found to be 56% to 75% 2,3. These exercises prevent pelvic floor insufficiencies by increasing anal sphincter muscle strength, urethral closure pressure and resistance. The patient’s complaints decrease in the 6th-8th weeks. The exercise program should be continued for at least 8-12 weeks, and when the continence level is reached, it should be combined with daily activities and become a lifelong lifestyle. For this, it is important to do the exercise regularly and correctly 4.
Studies have shown that more than 30% of women with SUI who were given PFMT were unable to contract their muscles correctly. In one study, approximately half of the women were unable to perform an effective contraction when verbally commanded, and one-fourth adopted a technique that could potentially worsen symptoms 5. The BF method, which is frequently used to facilitate this situation, provides information about the activity of striated muscles by giving visual and auditory stimuli to teach and control the correct contraction of the muscles.
The BF method is generally applied as an auxiliary method with PFMT rather than being used alone. With BF, the person increases the strength of this group of muscles by contracting only the PFM without contracting the abdominal muscles. Thus, the patient learns to selectively contract and relax the PFM by recognizing it. Superficial and internal electrodes, mobile applications, and EMG games are used for BF treatment 6.
There is no evidence that PFMT together with BF for the treatment of SUI in women provides superior therapeutic benefits compared to other types of applications (such as no application or PFMT alone) or that adding BF to other applications is more effective than applications alone 7. When the studies are examined, pelvic floor rehabilitation studies are found to investigate outcome measures such as urinary symptom severity, quality of life, and muscle strength 8,9. There are few studies that investigate the effect of PFMT activity potentials with the EMG method 10. In this respect, the results of our study are very important for the literature.
The aim of our study was to investigate the effect of BF- supported PFMT on muscle activity potential in SUI. It was aimed to provide a new perspective on the treatment protocol and to contribute to the literature by developing a more accessible exercise program that women diagnosed with SUI would enjoy and willingly participate in.
Materials and Methods
Procedure This study was conducted in the Urology Department between May 2023 and July 2024. All individuals participating in the study were given detailed information about the purpose and method of the study and their permissions were obtained by signing the informed consent form.
Participants In the study, 60 female volunteers were evaluated for eligibility and 18 were excluded from the study. The study was conducted on 42 female volunteers between the ages of 40- 65 who participated in the study voluntarily. Individuals were randomized into three groups: EMG - BF + PFMT group (n = 14), PFMT group (n = 14), and control group (n = 14) according to the envelope method. Medical treatment was also applied to all groups. Exclusion criteria from the study were; being pregnant, having an active urinary tract infection or a history of pelvic organ prolapse, and having undergone vaginal and pelvic surgery within the last 6 months. A demographic assessment form including age, height, weight, obstetric and gynecological characteristics, incontinence characteristics, and consumption habits was filled out for each participant. The treatment was carried out for 6 weeks and 3 days a week. Participants underwent EMG evaluation at the beginning of the treatment and at the end of week 6. All evaluations were performed by the same physiotherapist.
Measurements
Electromyography (EMG)
The electrical activity of a muscle is an indicator of muscle function. A single-channel NeuroTrac brand Myoplus 2 (Verity Medical Ltd, UK) EMG measuring device integrated with computer software was used to measure PTC activation in order to obtain electromyographic signals, digital analysis, and reports. Two active and one passive surface electrode were used in valid and reliable noninvasive surface EMG measurements. Active surface electrodes were placed on the right and left of the perineal body at 2 and 7 o’clock. The passive surface electrode was placed on the right thigh. The supine position with the PFM extremely relaxed was preferred during the measurement. In this position, the patient’s knees were flexed at 140 degrees, the soles of the feet were in full contact with the bed, and the thighs and feet were 30 cm apart. Only tonic PFM was evaluated during the measurement. The contraction and rest periods were set to five seconds on the device, and a total of 5 contractions and 5 resting EMG activities were measured for 50 seconds. The device gave a voice command of “work” to obtain a contraction response and “rest” to obtain a relaxation response. The average values of the EMG activity in the working and resting states in 50 seconds were recorded. At the end of the measurement, muscle activation was recorded in microvolts (μV).
Treatment Program
PFMT treatment
All cases were first taught how the correct function of the PFMT (correct contraction, relaxation, etc.) is. In the PFMT session, thoracic diaphragm activation, dynamic neuromuscular stabilization exercises (in supine, prone, and crawling positions), and endurance exercises were performed to retrain the ability to lengthen and extend the PFM. In thoracic diaphragm activation, 360° diaphragm breathing was taught with the hips and knees in 90° flexion. For DNS exercises, 3 and 6-month supine positions, 3, 6 and 7-month prone positions, 9-month crawling positions, and 3 and 4-month supine positions with a pilates ball were selected. Each development position was accepted as an exercise position. After correct positioning, the number of exercises was determined as the number of breaths. 3 sets, 10 repetitions, and 10 seconds of 360° expansive diaphragm breathing were performed in each position. A 2-minute rest period was given between sets and positions. An endurance exercise program was prepared that included cycles followed by a rest period twice as long as the contraction period in the retraining of the ability to shorten and lengthen the PFM. During this phase of training, one group performed exercises with BF support, while the other group performed exercises without BF. Slow contraction exercises were continued as 10 seconds of muscle holding and 20 seconds of relaxation, and fast contraction exercises were continued as 1-second contraction and 2 seconds of relaxation. An exercise program of 5 sets of 10 repetitions was created for each type of contraction. A 2-minute rest period was given between sets.
EMG-BF treatment
Animated EMG-BF treatment was performed with the NeuroTrac brand Myoplus 2 device and was performed in the same position (supine) as in the evaluation. Appropriate games (rabbit game, airplane game) were determined for animated EMG-BF treatment. Before starting the treatment, training was applied to show how to control the PFM and external urethral sphincter. Games were determined for animated EMG-BF treatment. There is a game protocol that includes 10 s contraction and 20 s relaxation cycles. Fast contraction exercises were continued as 1 s contraction and 2 s relaxation. There was an exercise program consisting of 5 sets of 10 repetitions for the type of contraction. A 2-minute rest period was given between sets. During the contraction (working phase), the patient was asked to count out loud so that the glottis would not close. In addition, the physiotherapist placed his hands on the abdominal and adductor muscles to prevent associated muscle contractions and observed the gluteal muscles.
Statistical Analysis
In the descriptive statistics of the data, mean, standard deviation, median, lowest, highest, frequency, and ratio values were used. Kolmogorov-Smirnov in the status of variables was measured with the Shapiro-Wilk test. Kruskal-Wallis test was recorded in the analysis of beautiful independent data with non-normal distribution. Wilcoxon test record in the analysis of dependent quantitative data. SPSS 28.0 program was used in the analyses.
Ethical Approval
This study was approved by the Ethics Committee of the Non- Interventional Clinical Research Ethics Committee of Istanbul Medipol University (Date: 2023-05-13, No: E-10840098- 772.02-3157).
Results
In our study investigating the effects of BF-supported PFMT on muscle activity potential in SUI, no significant difference was found between the groups in terms of demographic characteristics (p > 0.05) (Table 1).
There was no significant difference between the pre-treatment groups in terms of all EMG values. The analysis of the participants’ EMG parameters is shown in the table (Table 2). When the changes before and after treatment were compared, the study work average value showed a significant increase in all groups (p < 0.05). The pre-treatment/post-treatment value increase was found to be significantly higher in the PFMT + BF group than in the PFMT and control groups, and in the PFMT group than in the control group (p < 0.05).
When the changes before and after treatment were compared, the peak value showed a significant increase in all groups (p < 0.05). While the pre-treatment/post-treatment value increase was found to be significantly higher in the PFMT + BF and PFMT groups than in the control group (p < 0.05), no significant difference was found between the PFMT + BF and PFMT groups (p > 0.05).
When the changes before and after treatment were compared, the MVC (%) value showed a significant increase in all groups (p < 0.05). While the pre-treatment/post-treatment value increase was found to be significantly higher in the PFMT + BF and PFMT groups than in the control group (p < 005), no significant difference was found between the PFMT + BF and PFMT groups (p > 0.05) (Table 3).
Discussion
Surface electromyography (sEMG) is considered a tool for assessing PFM function by real-time assessment of PFM contractions and identification of motor unit action potentials. Electrical signals from muscles are generated by the activation of motor units during contraction. The bioelectrical activity of a muscle is monitored as a representation of muscle function 11. Dannecker et al., Bertotto A et al., Aukee et al. used sEMG to assess treatment progress, and increases in muscle activity were expressed in μV of amplitude. In these studies, it was reported that PFM resulted in a significantly greater increase in sEMG amplitude when the group receiving BF combined with PFMT was compared to the group receiving PFMT alone 12,13,14. In the study by Bertotto et al., improvements in muscle strength and EMG activity were observed in the PFMT + BF group, with the most significant gains reported in precontraction, endurance, and MVCs. The addition of BF to the treatment of muscle dysfunctions aims to improve voluntary motor activity by inducing neuroplasticity or functional neural regeneration mechanisms of the central nervous system. This neuroplasticity helps patients control and monitor future muscle activities and movements. sEMG-assisted BF was associated with a significant increase in the sEMG amplitude recorded during the tests 13. Aukee et al. reported greater improvement in patients who received sEMG-assisted BF training compared to those who received PFMT alone. The authors reported increased PFMT activity (μV) and fewer leakage episodes 14. Dannecker et al. attempted to determine the effect of 12 weeks of sEMG-BF- assisted training on PFMT in a study of 390 women diagnosed with SUI (80%) and MUI (20%). They observed that the sEMG electrical potential of the PFMTs increased from an average of 11.3 to 22 μV, thus confirming the high efficacy of PFMT 12. Rett et al., in their study of 26 women with SUI, found that all contractions (tonic and phasic) had significantly better PFM strength and sEMG amplitudes (μV) after 12 BF sessions 15. Yoo et al. reported that there was a significant change in the mean amplitude of tonic contraction measured by vaginal sEMG activity after the 8th session and that BF-assisted PFMT was successful in 57% of women with urinary incontinence 16. In 2017, Ptaszkowski et al. aimed to objectively evaluate the resting and functional bioelectrical activity of PFMT in women during menopause and compare it in three different positions of the pelvis (anterior pelvic tilt - position 1 (P1), posterior pelvic tilt - position 2 (P2), and neutral pelvic tilt - position 3 (P3)). The highest mean resting activity of sEMG PFMT (μV) was observed at P2, and this value was 11.6 μV (SD = 5.5 μV). The P1 value was found to be 9.8 μV (SD = 4.8 μV) and the P3 value was found to be 9.0 μV (SD = 4.2 μV). The results revealed a significant statistical difference. As a result, the posterior pelvic tilt position determines the higher resting and functional bioelectrical activity of the PFM 17. In our study, the posterior pelvic tilt position was preferred during the treatments. The EMG measurement results we made to determine the muscle activation values before and after the application support the literature. Finally, a study conducted in 2024 evaluated the effectiveness of DNS compared to traditional Kegel exercises and its effect on pelvic floor strength and core muscle activation in women diagnosed with SUI. The DNS group showed a greater increase in PFM strength compared to the Kegel exercise group. In other words, statistically, it was observed that DNS exercises provided more significant improvements in EMG measurements (average, peak, and MVC) compared to traditional Kegel exercises 3. In our study, the respiratory and stabilization approaches of the DNS method were used within the scope of pelvic floor training in individuals diagnosed with SUI. As a result, a significant improvement was observed in EMG parameters in the treatment groups with DNS exercises compared to the control group.
Limitations
As a limitation of our study, the short-term effects of the treatment were investigated. Long-term effects could also have been examined to obtain information about the permanence of the observed improvements.
Conclusion
It was found that the combined treatment method of PFMT + BF was beneficial in terms of its effect on muscle activity potential in SUI patients.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Istanbul Medipol University (Date: 2023-05-13, No: E-10840098-772.02-3157)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Krhut J, Gärtner M, Mokris J, et al. Effect of severity of urinary incontinence on quality of life in women. Neurourol Urodyn. 2018;37(6):1925-30.
-
Jacomo RH, Nascimento TR, Lucena da Siva M, et al. Exercise regimens other than pelvic floor muscle training cannot increase pelvic muscle strength–a systematic review. J Bodyw Mov Ther. 2020;24(4):568-74.
-
Sharma K, Gupta M, Parasher RK. The role of dynamic neuromuscular stabilization exercises in stress urinary incontinence among females aged 18-40 years. Cureus. 2024;16(5):1-19.
-
Abrams P, Andersson KE, Birder L, et al. Fourth International Consultation on Incontinence recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn. 2010;29(1):213-40.
-
Pennycuff JF, Borazjani A, Wang H, Iglesia C. Commercially available home pelvic training devices for the treatment of pelvic floor disorders: a systematic review and meta-analysis. Obstet Gynecol. 2022;140(2):275-92.
-
Araujo CC, Marques A de A, Juliato CRT. The adherence of home pelvic floor muscles training using a mobile device application for women with urinary incontinence: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2020;26(11):697-703.
-
Orhan C, Akbayrak T, Özgül S, et al. Effects of vaginal tampon training added to pelvic floor muscle training in women with stress urinary incontinence: randomized controlled trial. Int Urogynecol J. 2019;30(2):219-29.
-
Shah Z, Rathod P. Effect of home-based pelvic floor muscle training based on the severity of incontinence on quality of life in women with stress urinary incontinence. Physiother. 2020;14(2):80.
-
Sharma JB, Kakkad V, Roy KK, Kumari R, Pandey K. Role of incontinence severity index in evaluating severity and impact of treatment of stress urinary incontinence. J Midlife Health. 2022;13(2):139-44.
-
Ptaszkowski K, Malkiewicz B, Zdrojowy R, Paprocka-Borowicz M, Ptaszkowska L. The prognostic value of the surface electromyographic assessment of pelvic floor muscles in women with stress urinary incontinence. J Clin Med. 2020;9(6):1- 10.
-
Chmielewska D, Stania M, Kucab-Klich K, et al. Electromyographic characteristics of pelvic floor muscles in women with stress urinary incontinence following sEMG-assisted biofeedback training and Pilates exercises. PLoS One. 2019;14(12):1-22.
-
Dannecker C, Wolf V, Raab R, Hepp H, Anthuber C. EMG-biofeedback assisted pelvic floor muscle training is an effective therapy of stress urinary or mixed incontinence: a 7-year experience with 390 patients. Arch Gynecol Obstet. 2005;273(2):93-7.
-
Bertotto A, Schvartzman R, Uchôa S, Wender MCO. Effect of electromyographic biofeedback as an add-on to pelvic floor muscle exercises on neuromuscular outcomes and quality of life in postmenopausal women with stress urinary incontinence: a randomized controlled trial. Neurourol Urodyn. 2017;36(8):2142-7.
-
Aukee P, Immonen P, Penttinen J, Laippala P, Airaksinen O. Increase in pelvic floor muscle activity after 12 weeks’ training: a randomized prospective pilot study. Urology. 2002;60(6):1020-3.
-
Rett MT, Simoes JA, Herrmann V, Pinto CLB, Marques AA, Morais SS. Management of stress urinary incontinence with surface electromyography-assisted biofeedback in women of reproductive age. Phys Ther. 2007;87(2):136-42.
-
Yoo EH, Kim YM, Kim D. Factors predicting the response to biofeedback- assisted pelvic floor muscle training for urinary incontinence. Int J Gynaecol Obstet. 2011;112(3):179-81.
-
Ptaszkowski K, Zdrojowy R, Slupska L, et al. Assessment of bioelectrical activity of pelvic floor muscles depending on the orientation of the pelvis in menopausal women with symptoms of stress urinary incontinence: continued observational study. Eur J Phys Rehabil Med. 2017;53(4):564-74.
Tables
Table 1. Comparison of demographic characteristics of groups

A ANOVA / X² Ki-kare test (Fischer test), Mean±sd = mean±standard deviation; BMI = body mass index; PFMT = pelvic floor muscle training; BF = biofeedback
Table 2. Analysis of EMG parameters of participants
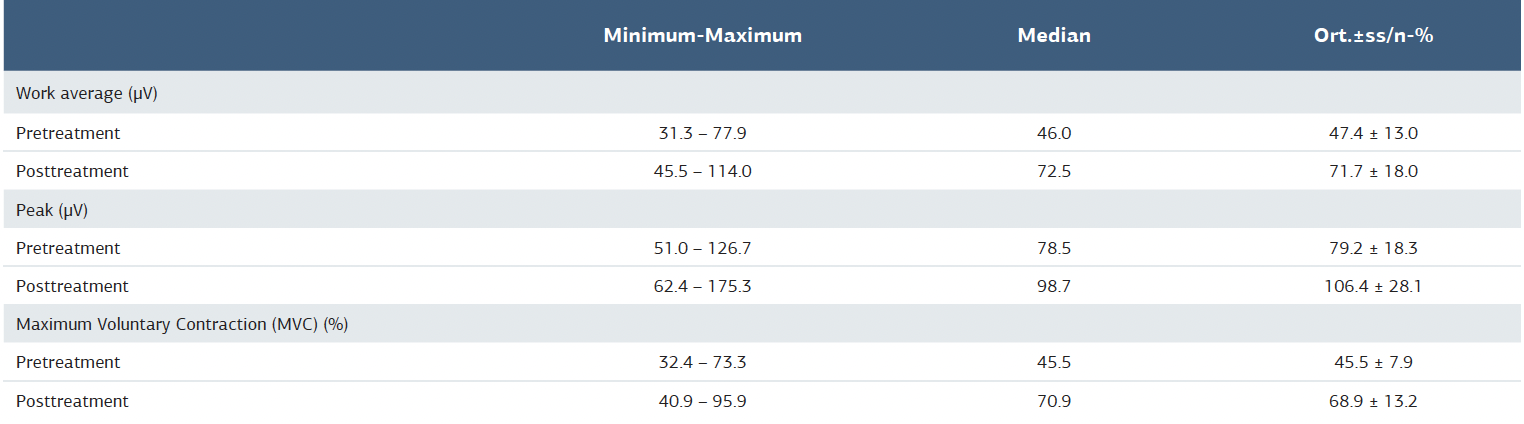
Table 3. Comparison of work average (μv), peak (μv) and MVC (%) values from EMG results of groups

K Kruskal-Wallis (Mann-Whitney u test) / w Wilcoxon test; Mean±SD = mean±standard deviation; PFMT = pelvic floor muscle training; BF = biofeedback
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Büşra İnce, Devrim Tarakçı, Aykut Başer. Biofeedback support in stress urinary incontinence the effect of pelvic floor muscle training on muscle activity potential. Ann Clin Anal Med 2025;16(10):683-687