
Long-term evaluation of the ocular surface after reconstructive surgery in malignant periocular tumors
Evaluation of the ocular surface after reconstructive surgery
- Received:
- September 27, 2024
- Accepted:
- March 10, 2025
- Published Online:
- March 15, 2025
- Printed:
- October 1, 2025
Authors
Abstract
Aim Our aim in this study was to evaluate postoperative complications and dry eye parameters after reconstructive surgery for primary periocular malignant lesions.
Methods Patients who underwent reconstructive surgery after malignant eyelid and periocular tumor excision were evaluated in two groups: those with defects involving the lid margin and those with defects sparing the lid margin. Demographics, histopathology, lesion location, horizontal eyelid defect size, surgical procedure, postoperative complications, and dry eye test results were compared between the groups.
Results The study included 68 patients: 35 with lesions involving the lid margin and 33 with lesions sparing the lid margin. The mean age was 69.9±14.95 years. Histopathology confirmed basal cell carcinoma in 86.8% of the cases, and 54.4% of the tumors were on the lower lid. Cases involving the lid margin had more postoperative complications, as well as a higher rate of postoperative dry eye disease (DED) (p < 0,05).
Conclusion Our results indicate that reconstructive surgeries for tumors involving the lid margin are more prone to postoperative complications and may also cause the onset or exacerbate preexisting DED.
Keywords
Introduction
Eyelid tumors are the most frequent neoplasms encountered in clinical ophthalmology practice 1,2. Malignant eyelid tumors constitute approximately 5-10% of all skin cancers and represent the main reason for eyelid reconstruction in oculoplastic surgery 3,4,5. A successful reconstruction of the eyelid and periocular region requires good knowledge of its complex structure. The choice of surgical procedure depends on the size, location, and depth of the lesion. Anterior lamellar defects not involving the eyelid margin are repaired by primary closure, rotational flaps, or free skin grafts according to the size of the defect. For full-thickness defects that involve the eyelid margin, repair by primary closure with or without cantholysis is recommended for those less than 30% of the horizontal lid width, whereas larger defects covering more than 30% require tarsoconjunctival flaps, rotational flaps, or myocutaneous semicircular flaps, free grafts, or a combination of these procedures 5. The Tenzel technique (myocutaneous semicircular flap) is a one-stage procedure used in full- thickness defects affecting 30% to 50% of the horizontal length of the lid 6. The Hughes procedure (tarsoconjunctival flap) is a reliable two-stage eyelid-sharing technique for the reconstruction of full-thickness defects that span more than 50% of the lid 7. Each of these procedures has its advantages and disadvantages.
Dry eye disease (DED) is an ocular surface disorder frequently encountered after eyelid surgery 8,9. The TFOS DEWS II revised the definition of dry eye as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles” 10. As some reconstructive surgeries involve a full-thickness lid defect, DED is inevitable 11. For this reason, a good understanding of the anatomy and physiology of the eyelid and ocular surface is necessary to manage dry eye after eyelid surgery.
The importance of the ocular surface and possible dry eye complications may be overlooked while focusing on the excision and complete treatment of malignant tumors. Therefore, we aimed in this study to retrospectively analyze the surgical outcomes of reconstructive procedures performed in patients with periocular malignant lesions and evaluate their effects on the ocular surface and tear film.
Materials and Methods
Data were collected from the clinical notes and electronic records of patients who underwent reconstructive surgery after malignant eyelid and periocular tumor excision in the ophthalmology department of Diskapi Yıldırım Beyazıt Training and Research Hospital between 2014 and 2023. The patients were divided into two groups, those with lesions involving the lid margin and those with lesions sparing the lid margin. In addition to lid margin involvement, we evaluated the patient’s demographic characteristics, the histologic type, and the location of the lesion according to Spinelli and Jelks 12, horizontal defect size in lesions involving the lid margin, the surgical procedure performed, postoperative complications, and dry eye test results. Patients with at least 6 months of postoperative follow-up were included in the study to allow evaluation of long-term complications.
In both margin-involving and margin-sparing cases, surgical procedures were selected according to lesion location and defect size after excision, as follows:
1. Lesions involving the lid margin:
a. Primary closure for full-thickness defects < 30% of the lid width (Figure 1).
b. Tenzel’s lateral advancement flap for defects 30%-50% of lid width
c. Hughe’s tarsoconjunctival flap with skin graft for defects > 50% of lid width
2. Lesions sparing the lid margin:
a. Primary closure for elliptical defects ≤ 2 cm × 1 cm.
b. Secondary closure with a rotational flap or free graft for irregular defects > 1 cm × 1 cm (Figure 2).
The surgical excision was performed either by leaving 3-4 mm of intact tissue around the tumor border and frozen section examination at the same intervention or excisional biopsy of the suspicious lesion in a prior surgery. If malignant tumor cells were detected in the surgical margin, further excision was performed until a clear margin was obtained.
Based on the TFOS DEWS II report, the dry eye assessment included Ocular Surface Disease Index (OSDI), noninvasive tear break-up time (NIBUT), and ocular surface staining 10. Dry eye assessment was compared between groups preoperatively and postoperatively with intervals of 6 months, 1 year, and 3 years.
Ocular Surface Disease Index
The patients completed the OSDI questionnaire before the examination to ensure their responses would not be influenced by the clinical procedures. The 12 items on the OSDI questionnaire were rated from 0 to 4, with 0 indicating the stated symptom occurred “none of the time”; 1, “some of the time”; 2, “half of the time”; 3, “most of the time”; or 4, “all of the time”. The total OSDI value was then calculated with the following formula: OSDI = (sum of the scores for all questions answered × 100) / (total number of questions answered × 4) 13,14. The previously validated Turkish version of the OSDI questionnaire was used 13. An OSDI value between 0 and 12 was considered normal, and values of 13 or more were considered pathologic.
Noninvasive Tear Break-up Time
The NIBUT of the participants was measured using a Sirius multifunctional topography device according to the manufacturer’s instructions. Before starting the measurement, the image was centered and sharpened. The patient was instructed to blink twice to spread the tear film across the ocular surface, then keep their eyes open as long as possible. The device automatically measures after the patient blinks twice. The device evaluates time-dependent changes in the integrity of the tear film spread over the anterior corneal surface. The test is performed through videokeratoscopy, a video recording of the Placido disk ring projection on the patient’s precorneal tear film. A homogeneously distributed tear film on the ocular surface causes a regular appearance in the rings and any deformation or disruption in the tear film results in deformation in one or more rings. The device records the time from the patient’s double blink to distortion or interruption in the Placido disk pattern as the NIBUT. The mean duration of all break-up intervals occurring in the precorneal tear film after blinking is recorded by the device as the average NIBUT. A NIBUT ≥10 s was considered normal 10.
Ocular Surface Fluorescein Staining
After NIBUT measurement, the ocular surface was stained with fluorescein and examined using a cobalt blue filter 15,16. Pathologic fluorescein staining was evaluated according to the TFOS DWES II report and defined as: > 5 corneal spots, > 9 conjunctival spots, or lid margin staining (≥ 2 mm length and ≥ 25% width).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows version 21.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as mean ± SD. The chi- square test was used for categorical variables. Parametric variables were compared between groups via analysis of variance and t-test. Nonparametric data were compared using the Kruskal-Wallis and Mann-Whitney U tests, as appropriate. The level of statistical significance was set at p<0.05.
Ethical Approval
This study was approved by the ethics committee of the University of Health Sciences, Diskapi Yildirim Beyazit Training and Research Hospital in Ankara, Turkey (Date: 2020-04-20, No: 85/05).
Results
A total of 68 patients who underwent eyelid and periocular reconstructive surgery were identified for inclusion in the study. The mean age was 69.9±14.95 years (range: 32-93 years; 68.6 ± 14.4 years in patients with lid involvement, 71.3 ± 15.6 years in those without lid involvement) (p = 0,46). There was a male preponderance, with 72% (n = 49) of the patients being men. Sex distribution was statistically similar in groups (p = 0,17). Histopathology confirmed that 86.8% (n = 59) of the eyelid and periocular malignancies were basal cell carcinoma (BCC) (Figures 1 and 2). The most common location was the lower eyelid (54.4%, n = 37). The patients’ lesion locations, horizontal defect sizes, and surgical procedures are summarized in Table 1. Postoperative complications among patients with eyelid margin involvement included ectropion in two patients after Hughes ’ procedure and mild entropion without trichiasis in 1 patient after Tenzel’s procedure for lid reconstruction. Four patients exhibited acceptably mild lid margin notching after Tenzel’s procedure in three patients and pentagon excision with primary closure in one patient (Figure 1b). Among the lid-sparing cases, only one patient with a lesion near the medial canthus developed mild ectropion that was treated 6 months later with a lazy-T procedure. The other two cases of ectropion developed after Hughes ’ procedure were treated after approximately 5 months with lateral tarsal strip fixation. The patients with entropion and eyelid notching were satisfied with their results, and no further surgery was performed.
Preoperatively, only the mean OSDI score was significantly higher in the lid margin involved group. In the postoperative period assessments, the OSDI score was higher in the lid margin spared group in the first year of control. The NIBUT and corneal staining were more common among patients with lid margin involvement in the 6-month and 1st year of control, but the differences did not reach statistical significance in the 3rd year of control. Detailed patients’ dry eye test results are summarized in Table 2.
Discussion
A stable precorneal tear film and healthy ocular surface are essential for comfort and clear vision. Periocular tumors, especially those involving the lid margin, can alter tear film composition and homeostasis by affecting the meibomian glands, which leads to changes in tear volume and turnover and results in ocular surface dysfunction and discomfort. Surgical excision of these lesions can also result in postoperative complications such as lagophthalmos and DED by causing iatrogenic meibomian gland loss, irregular lid margin contour, and lid retractor and orbicularis oculi muscle loss or dysfunction 10,11. Management of such complications is as important as removing the malignant tumor for the quality of life after tumor excision. Therefore, we aimed in this study to emphasize the importance of maintaining a healthy ocular surface and a stable tear film after preocular malignant tumor excision.
Hyperemic and/or hypertrophic eyelid margins, ectropion, entropion, ocular irritation, and persistent mucoid discharge are reported complications after eyelid reconstructions 7. Our study revealed that complications were statistically more frequent in cases involving the lid margin. Two cases of ectropion, one case of entropion, and four cases of lid margin notching were reported after surgical treatment among those with lid margin involvement, whereas only one case of ectropion was reported among those with excisional defects sparing the lid margin. Ectropion required correction in a secondary surgery 5 to 6 months after the first operation. Luu et al. 17 reported hypertrophic changes in the lower eyelid margin after Hughes ’ procedure. Aggarwal et al. 18 reported one patient with a small pyogenic granuloma and another with mild ectropion after Hughes ’ procedure. They also stated that using an amniotic membrane in the second stage of Hughes ’ procedure prevented the hypertrophic changes in the lid margin. In our study, only one case of ectropion was reported after Hughes ’ procedure. According to TFOS DEWS II, the lid margin and meibomian glands are recognized as key components in the etiology of DED, and eyelid surgeries are listed as an iatrogenic cause of DED onset or worsening of preoperative dry eye 19. The management of DED should start with a preoperative evaluation and continue postoperatively, especially in patients with preexisting DED 9.
In this study, the results of dry eye assessments showed no significant difference between groups except for the OSDI score (OSDI score p = 0,0001; NIBUT p = 0,94; corneal staining p = 0,97). This could be explained as a result of the affected lid and lid margin, as we mentioned above. Whereas, in the postoperative assessments, the lid margin involved group showed a significantly lower NIBUT and a higher prevalence of fluorescein corneal staining in the 6th month (p = 0,008; p = 0.001, respectively) and 1st year of control (p = 0,017; p = 0,049 respectively). As patients in our study had a high mean age (69.9 ± 15.0 years), which is considered another risk factor for DED, these patients were followed up in our clinic with dry eye treatment postoperatively. Therefore, results of dry eye assessments in the 3rd year of control were comparable in both groups, showing better results with no significant difference (OSDI score p = 0,54; NIBUT p = 0,085; corneal staining p = 0,96). To the best of our knowledge, this is the first study to evaluate ocular surface findings and dry eye tests; according to the TFOS DEWS II 2017 report 19, in patients with malignant eyelid and periocular tumors after surgical treatment, with comparison according to lid margin involvement for three years. Klein-Theyer et al. 20 conducted a study evaluating the ocular surface and tear film function in 18 patients following the modified Hughes ’ procedure and observed a lower fluorescein tear break-up time (TBUT) (p=0.03), higher OSDI, and increased corneal staining in operated eyes compared to non-operated eyes. Similarly, Zaky et al. 21 reported lower TBUT in operated eyes than in non-operated eyes after the modified Hughes ’ procedure. Wang et al. 22 also reported that McMonnies dry eye score was significantly higher and NIBUT was lower in operated eyes after the modified Hughes ’ procedure when compared to contralateral eyes (p < 0.05). In the abovementioned studies, dry eye tests were compared between operated and contralateral non-operated eyes, especially after the modified Hughes ’ procedure. In contrast, Gonnermann et al. 23 compared 17 patients who underwent full-thickness eyelid reconstruction with a control group and observed no significant difference in TBUT and Schirmer test results.
DED after periocular tumor excision is a multifactorial disease. The mechanism of DED in these cases is mainly attributed to one or more of the following factors: meibomian gland loss, changes in the eyelid anatomy that affect normal eyelid closure and its relation with the cornea, and loss of the orbicularis oculi in some cases, which might lead to decreased blink rate and lagophthalmos. In patients with lid margin involvement, loss of meibomian glands in both the upper and lower eyelids after Hughe’s procedure and the lower eyelid in Tenzel’s procedure causes decreased lipid secretion and hence an unstable tear film. Also, changes in the eyelid anatomy and its position relative to the ocular surface increase the risk of DED or exacerbate the pre-existing condition.
Limitations
There are several limitations of this study, including the relatively small number of patients per group and our evaluation of only operated eyes in both groups. In addition, our evaluation did not include inflammatory markers or osmolarity. Therefore, we believe that further studies should be conducted with a larger number of subjects and a more comprehensive analysis including pre- and postoperative inflammatory cytokines and osmolarity to more clearly understand the effects of eyelid reconstructive surgery on DED.
Conclusion
In conclusion, tumor size and location are the best factors in selecting a surgical procedure for eyelid repair and reconstruction. Very good results are achievable depending on proper surgical planning, surgical experience, and postoperative care. Our results indicate that surgical procedures for tumors involving the lid margin are more prone to postoperative complications and might induce DED or exacerbate pre-existing DED. Therefore, for the best functional and esthetic results, we believe that the reconstruction of large defects after malignant tumor excision should be performed by experienced surgeons. Furthermore, preoperative and postoperative DED management should not be neglected in all patients with periocular tumors.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of University of Health Sciences, Diskapi Yildirim Beyazit Training and Research Hospital (Date: 2020- 04-20, No: 85/05)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Huang YY, Liang WY, Tsai CC, et al. Comparison of the clinical characteristics and outcome of benign and malignant eyelid tumors: an analysis of 4521 eyelid tumors in a tertiary Medical Center. Biomed Res Int. 2015;2015:453091.
-
Deprez M, Uffer S. Clinicopathological features of eyelid skin tumors. A retrospective study of 5504 cases and review of the literature. Am J Dermatopathol. 2009;31(3):256-62.
-
Eren MA, Gündüz. Demographic features and histopathological diagnosis in primary eyelid tumors: results over 19 years from a tertiary center in Ankara, Turkey. Int J Ophthalmol. 2020;13(8):1287-93.
-
Burgic M, Iljazovic E, Vodencarevic AN, et al. Clinical characteristics and outcome of malignant eyelid tumors: a five-year retrospective study. Med Arch. 2019;73(3):209-12.
-
Mathijssen IMJ, Meulen JC van der. Guidelines for reconstruction of the eyelids and canthal regions. J Plast Reconstr Aesthet Surg. 2010;63(9):1420-33.
-
Cha JA, Lee KA. Reconstruction of periorbital defects using a modified Tenzel flap. Arch Craniofac Surg. 2020; 21(1):35-40.
-
Hishmi AH, Koch KR, Matthaei M, Bölke E, Cursiefen C, Heindl LM. Modified Hughes procedure for reconstruction of large full-thickness lower eyelid defects following tumor resection. Eur J Med Res. 2016;21(1):27.
-
Morax S, Touitou V. Complications of blepharoplasty. Orbit 2006;25(4):303-18.
-
Heidari M, Haydar AA, Rajabi MT, Rafizadeh SM. Corneal biophysical changes after upper eyelid blepharoplasty and ptosis surgery: a review. BMC Ophthalmol. 2023;23(1):253.
-
Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf 2017;15(3):276-83.
-
Espinoza GM, Israel H, Holds JB. Survey of oculoplastic surgeons regarding the clinical use of tear production tests. Ophthalmic Plast Reconstr Surg. 2009;25(3):197-200.
-
Subramanian N. Reconstructions of eyelid defects. Indian J Plast Surg. 2011;44(1):5-13.
-
Irkec M. Reliability and validity of Turkish translation of the Ocular Surface Disease Index (OSDI) in dry eye syndrome. Invest Ophthalmol Vis Sci. 2007;48(13):408-610.
-
Dogru M, Stern ME, Smith JA, Foulks GN, Lemp MA, Tsubota K. Changing trends in the definition and diagnosis of dry eyes. Am J Ophthalmol. 2005;140(3):507-8.
-
Kim J. The use of vital dyes in corneal disease. Curr Opin Ophthalmol. 2000;11(4):241-7.
-
Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003:22(7):640-50.
-
Luu ST, Cannon PS, Selva D. Hypertrophic changes of the lower eyelid margin after Hughes procedure for eyelid reconstruction: the management and outcomes. Ophthal Plast Reconstr Surg. 2010;26(5):344-7.
-
Aggarwal S, Shah CT, Kirzhner M. Modified second stage Hughes tarsoconjunctival reconstruction for lower eyelid defects. Orbit. 2018:37(5):335-40.
-
Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511-38.
-
Klein-Theyer A, Howarth-Winter J, Dieter FR, Haller-Schober EM, Reidl R, Boldin I. Evaluation of ocular surface and tear film function following modified Hughes tarsoconjunctival flap procedure. Acta Ophthalmol. 2014:92(3):286-90.
-
Zaky AG, Elmazar HMF, Elaziz MSA. Longevity results of modified Hughes procedure in reconstructing large lower eyelid defects. Clin Ophthalmol. 2016;10:1825-8.
-
Wang M, Kersey TL, Sloan BH, Craig JP. Evaporative dry eye following modified Hughes flap reconstruction. Clin Exp Ophthalmol. 2018;46(6):700-2.
-
Gonnermann J, Klein JP, Klamann KJ, et al. Dry eye symptoms in patients after eyelid reconstruction with full-thickness eyelid defects: using the Tomey TG-1000 thermographer. Ophthalmic Res. 2012;48(4):192-8.
Figures
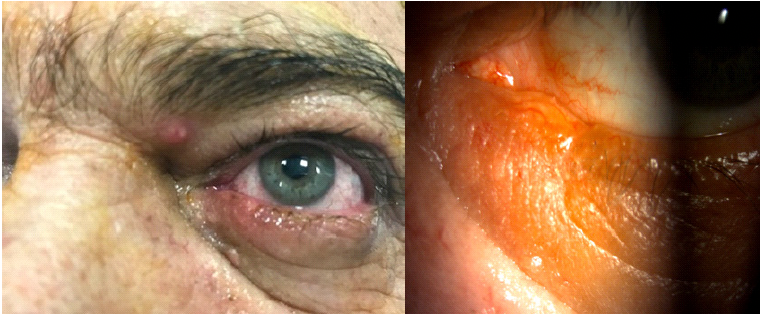
Figure 1. a) Basal cell carcinoma involving the lower lid margin in a 42-year-old male patient. b) Postoperative image after pentagon excision with a safe margin. Note the acceptably mild notching in the lid margin

Figure 2. a) Basal cell carcinoma in the lower eyelid sparing the lid margin in a 69-year-old male patient. b) The defect after tumor excision was larger than 1 cm2 and was reconstructed with a glabellar flap. c) Appearance at 17 months postoperatively
Tables
Table 1. Distribution of tumor location, defect size, and surgical procedures used for lid reconstruction
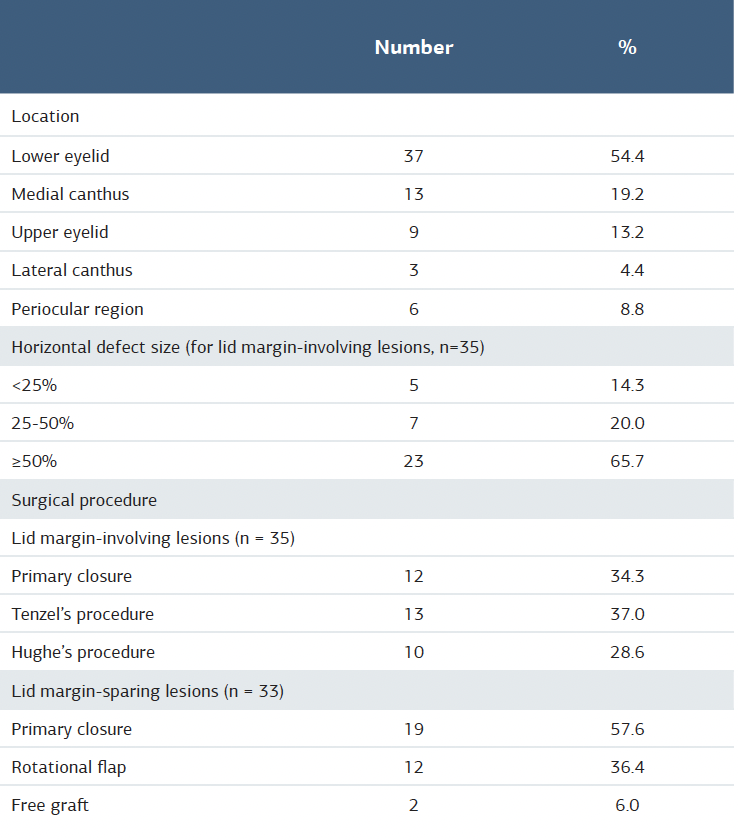
Table 2. Comparison of preoperative and postoperative dry eye test results between the groups
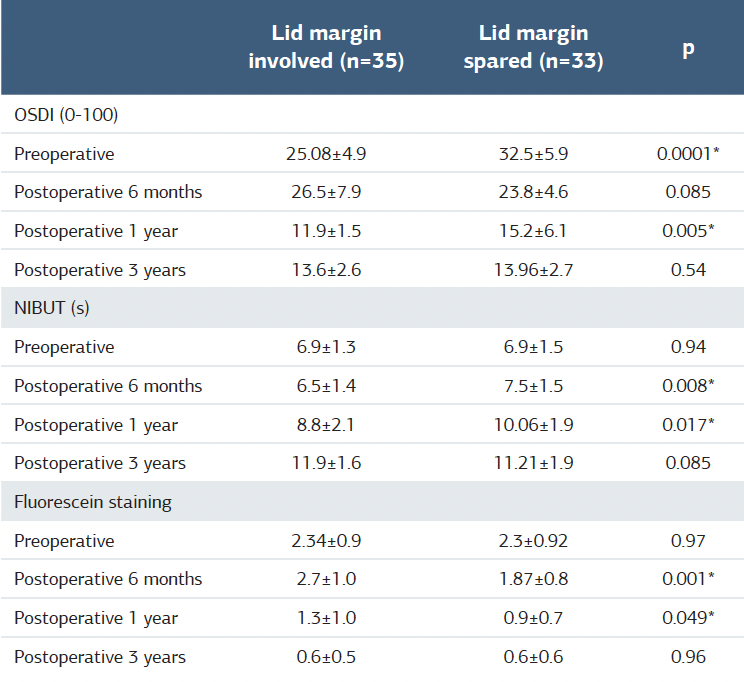
OSDI = ocular surface disease index; NIBUT = non-invasive tear break-up time *p<0.05 independent-samples t-test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Neşe Arslan, Ahmet Alp Bilgiç, Naciye Kabataş, Mutlu Acar.vLong-term evaluation of the ocular surface after reconstructive surgery in malignant periocular tumors. Ann Clin Anal Med 2025;16(10):688-692