
Laboratory biomarkers associated with suicidal ideation in major depressive disorder: a retrospective study in the emergency department
Biomarkers in MDD with suicidal ideation
- Received:
- July 23, 2025
- Accepted:
- September 22, 2025
- Published Online:
- September 30, 2025
- Printed:
- October 1, 2025
Authors
Abstract
AimMajor Depressive Disorder (MDD) is a prevalent psychiatric condition that significantly contributes to global disease burden. Suicidal ideation (SI), a common manifestation of MDD, represents a critical point along the suicide risk continuum. Recent research has indicated that MDD may be associated not only with psychological symptoms but also with systemic physiological alterations detectable through laboratory biomarkers. This study aims to investigate the association between routinely collected laboratory parameters and SI in patients with MDD presenting to the emergency department (ED), with the goal of identifying potential biological indicators of acute suicide risk.
MethodsThis retrospective observational study utilized data from the MIMIC-IV database (v2.2). A total of 123 adult patients (≥ 18 years) diagnosed with MDD (ICD-9: 296.20; ICD-10: F32.9) and presenting to the ED with SI as the chief complaint were included. Laboratory data from the first 24 hours of admission were analyzed. Statistical analyses included t-tests, Mann–Whitney U tests, chi-square tests, and subgroup analyses.
ResultsAmong the 123 patients (54.5% male), 45.5% had a history of multiple suicide attempts, 48.0% had psychiatric comorbidities, and 31.7% had substance use disorders. Abnormal white blood cell counts (80.5%), neutrophils (64.2%), hemoglobin (36.6%), and creatinine (29.9%) were prevalent. Male patients exhibited significantly higher rates of abnormal ALT, creatinine, hemoglobin, and hematocrit values. Patients with multiple suicide attempts had higher rates of antidepressant use, smoking, alcohol consumption, and chronic medical conditions.
ConclusionThis study underscores the complex interplay between psychiatric, behavioral, and physiological factors in MDD patients with SI. Routine laboratory parameters may serve as accessible adjunctive markers in acute suicide risk stratification. Integrating biological data with psychiatric assessment in ED settings may enhance early identification and intervention for high-risk individuals.
Keywords
Introduction
Major Depressive Disorder (MDD) is one of the leading causes of neuropsychiatric impairment worldwide and represents a substantial contributor to overall disease burden. MDD has been estimated to account for approximately 49.4 million disability- adjusted life years globally in 2020, highlighting its significant impact on population health 1. MDD is a prevalent psychiatric condition involving depressive episodes of at least two weeks with mood changes, reduced interest, cognitive impairments, and physiological disturbances 2. Emerging evidence suggests that MDD is associated not only with psychological symptoms but also with measurable alterations in systemic biomarkers. Increased concentrations of inflammatory markers such as C-reactive protein 3, interleukin-6 4, and various other pro- inflammatory cytokines 5 have been consistently identified in individuals with MDD, indicating the presence of a persistent low-grade inflammatory state. Higher serum albumin levels have been inversely associated with depressive symptoms, as shown by Zhang et al. 6, and were also significantly linked to lower odds of depression in another study 7. Additionally, abnormalities in serum sodium, creatinine, white blood cell counts, and liver enzymes have been noted in some cohorts, potentially reflecting the somatic burden or comorbid conditions frequently co-occurring with MDD 3. Suicidal ideation (SI), defined as thoughts of engaging in behavior intended to end one’s life, represents a critical early marker in the continuum of suicidal behavior, which may progress to suicide planning, attempts, and completed suicide if unaddressed 8. SI is strongly associated with psychological factors such as hopelessness, feelings of worthlessness, and impaired problem-solving, as well as neurobiological alterations including serotonergic dysfunction and hypothalamic-pituitary- adrenal (HPA) axis dysregulation 9,10. The biological disturbances in individuals with MDD are not only markers of disease severity but may also contribute to the heightened mortality in this population. Individuals diagnosed with MDD face an overall mortality rate that is 1.8 times higher than that of the general population 11. This elevated disease burden is partly attributed to the increased likelihood of SI and suicidal behaviors, including suicide attempts and completed suicides 11. Emergency departments (EDs) frequently represent the first point of contact for individuals in suicidal crisis, serving as critical gateways for mental health triage, stabilization, and referral 12. Presentations to the ED for suicidal thoughts or behaviors, whether ideation, planning, or recent attempts, are considered psychiatric emergencies that demand immediate and comprehensive evaluation to assess risk and initiate appropriate intervention strategies 13. In these acute care settings, routine laboratory testing is commonly employed as part of medical clearance protocols prior to psychiatric admission or transfer. While primarily aimed at identifying underlying medical conditions or substance intoxication, these tests can also yield physiological data relevant to psychiatric evaluation 14.
The Medical Information Mart for Intensive Care IV (MIMIC-IV) is a large, publicly available electronic health database developed through a collaboration between the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center, comprising comprehensive, de-identified clinical data from over 60,000 patients between 2008 and 2019 15. This dataset integrates a wide range of information, including ED encounters, vital signs, laboratory results, medications, diagnoses, procedures, and demographic characteristics. Given its granularity and longitudinal structure, MIMIC-IV enables researchers to investigate complex relationships between psychiatric presentations and associated physiological markers across diverse clinical settings. The objective of this study is to investigate the association between laboratory biomarkers and SI among patients diagnosed with MDD who present to the ED. By analyzing routinely collected laboratory data during initial ED evaluation, the study aims to determine whether certain physiological markers indicate acute psychiatric risk. Ultimately, this approach may contribute to the identification of biological indicators that could assist clinicians in the early detection of SI in high-risk patients and to explore whether specific laboratory parameters may serve as biological markers of suicidality in individuals with MDD.
Materials and Methods
Participants and Study Design
This retrospective observational study utilized data from the MIMIC-IV database (version 2.2). In accordance with institutional and data access regulations, the required approvals to access the MIMIC-IV database were obtained, including certification through the Collaborative Institutional Training Initiative (Record ID: 68301129). Compliance with data use protocols and the performance of all data extraction procedures for the present study were ensured. We identified adults (≥18 years) diagnosed with MDD who presented to the ED for SI. This was determined using the following International Classification of Diseases codes: ICD-9 code 296.20 and ICD-10 code F32.9. Patients were included if they had at least one ED admission recorded in the MIMIC-IV database. This initial selection yielded a cohort of 1,635 unique patients. To ensure the clinical relevance and specificity of the sample, further inclusion and exclusion criteria were applied. Patients were retained in the final sample only if SI was explicitly documented as the chief complaint during the ED visit. Individuals were excluded if they had comorbid acute medical conditions, additional psychiatric diagnoses listed as the primary reason for admission, or multiple ED visits, with only the first admission per patient included in the analysis. After these criteria were applied, a total of 123 patients remained eligible for analysis. Laboratory values from the first 24 hours were averaged if multiple results were present. Abnormalities were defined according to the reference ranges embedded in the MIMIC-IV database. The use of the de-identified, publicly available MIMIC-IV database was approved by the MIT Institutional Review Board, with informed consent waived due to the anonymized nature of the data.
Data Collection
Demographic information included age, sex, ethnicity, smoking status, and multiple suicide attempts. Relevant comorbidities were identified, including substance use disorder, alcohol use disorder, psychiatric disorders and chronic diseases including diabetes, hypertension, and asthma. Information regarding psychotropic medications at the time of admission such as antidepressants, were also obtained. Laboratory data were collected exclusively from the first 24 hours following admission and included serum sodium, serum creatinine, bicarbonate, albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), white blood cell (WBC), hemoglobin, hematocrit, lymphocytes, neutrophils, eosinophils, monocytes, and alkaline phosphatase.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 27). Continuous variables were assessed for normality using the Kolmogorov–Smirnov test and were presented as median (IQR) according to data distribution, whereas categorical variables were expressed as proportions. The t-test and Mann–Whitney U test were used to analyze continuous variables. The chi-square test was applied for the analysis of categorical variables. Subgroup analyses were conducted to compare patients with SI, as well as those with and without substance use disorders or other psychiatric comorbidities, in terms of the prevalence and distribution of abnormal laboratory values. In cases involving multiple comparisons, Bonferroni correction was applied to adjust for the inflated risk of Type I error. A p-value < 0.05 was considered statistically significant.
Ethical Approval
This study did not require ethical approval as it utilized the publicly available and fully de-identified MIMIC-IV database. According to the data usage policy of MIMIC-IV, all data are de- identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA) standards, and no individual consent or institutional review board approval is necessary for analysis. The use of the database was approved through completion of the required training (CITI Program Record ID: 68301129). All procedures were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Results
A total of 123 adult patients (male: 54.5%) aged between 18 and 39 years (59.3%) and diagnosed with MDD who presented to the ED were included in the analysis. A notable proportion had chronic medical conditions (43.9%) and a history of multiple suicide attempts (45.5%). Antidepressant use was reported by 71.5% of participants, and 48.0% had at least one comorbid psychiatric disorder, most commonly bipolar disorder and schizophrenia spectrum disorders. Additionally, 31.7% of the samples had a diagnosed substance use disorder, with cocaine and polysubstance use being the most frequent. Detailed demographic and clinical characteristics are presented in Table 1. Among the laboratory parameters, abnormal white blood cell count was observed in 80.5% of patients, followed by neutrophils (64.2%), hematocrit (38.2%), lymphocytes (38.2%), hemoglobin (36.6%), and monocytes (35.8%) (Table 2). Table 3 presents the comparison of clinical and behavioral characteristics between patients with and without multiple suicide attempts. Patients with multiple suicide attempts had a significantly higher prevalence of substance use disorder (p = 0.0087), psychiatric comorbidities (p < 0.0001), and alcohol use disorder (p < 0.0001), compared to those with no history of multiple attempts. Similarly, the rate of antidepressant use was notably elevated among patients with multiple suicide attempts (94.6% vs. 52.2%, p < 0.0001). Smoking was also more frequent in this group (26.8% vs. 10.4%, p = 0.0341). Additionally, the presence of chronic medical conditions was significantly higher in the multiple attempt group (p < 0.0001). Figure 1 illustrates the strength and direction of monotonic relationships between continuous laboratory parameters using Spearman’s rank correlation. The strongest positive associations were found between ALT and AST (r = 0.79, p < 0.001) and hemoglobin and hematocrit (r = 0.74, p < 0.001), reflecting expected clinical parallels. In contrast, a moderate negative correlation was identified between creatinine and bicarbonate (r = –0.23, p = 0.011), potentially indicating metabolic compensation. Additional weak but significant correlations included ALT and alkaline phosphatase (ALP) (r = 0.30) and sodium and monocytes (r = –0.24). Statistically significant gender differences were found in the frequency of abnormal hemoglobin (male: 46.3%, female: 25.0%), hematocrit (male: 50.8%, female: 23.2%), alanine aminotransferase (male: 25.8%, female: 7.6%), and creatine (male: 29.9%, female: 12.7%) values. Abnormal hemoglobin, hematocrit, alanine aminotransferase, and creatinine levels were more frequent in males than in females.
Figure 2 illustrates the gender-based distribution of abnormal laboratory values for hemoglobin, hematocrit, creatinine, and ALT. The total number of abnormal laboratory parameters was significantly higher in male patients compared to females (p < 0.0001), and in those taking antidepressants compared to non-users (p = 0.0139). No significant difference was observed between patients with and without chronic disease (p = 0.1313).
Discussion
This study analyzes patients with MDD and SI in the ED, integrating demographic, clinical, and laboratory data. In addition to examining the behavioral and diagnostic characteristics of individuals with multiple suicide attempts, we also assessed physiological changes using routine lab data collected acutely. Our results reveal that patients with repeated suicidal behavior exhibit a higher burden of psychiatric comorbidity, substance and alcohol use, and chronic medical illness, alongside distinct physiological alterations, including abnormal laboratory parameters. Together, these findings suggest that suicidality in MDD may reflect not only psychological distress but also underlying biological dysregulation, offering a more comprehensive view of acute suicide risk in emergency contexts. A study by Bachmann 16 conducted a narrative review examining the global epidemiology of suicide, highlighting psychiatric comorbidity, substance use, and gender differences as key risk factors. Bachmann emphasized the heightened suicide risk shortly after psychiatric discharge, particularly in males and individuals with prior suicide attempts. Combinations of mood and substance-related disorders were noted to significantly amplify this risk. Another study by Reneses et al. 17 proposed a clinical staging model of depressive disorders, emphasizing that treatment resistance and persistent residual symptoms are markers of more advanced stages of illness, often associated with greater functional impairment and increased suicide risk. Consistent with these findings, our study revealed that 45.5% of participants had a history of multiple suicide attempts and over half were male. Additionally, 48.0% had comorbid psychiatric disorders, mainly bipolar and schizophrenia spectrum, and 31.7% had substance use disorders, particularly involving cocaine and polysubstance use. This convergence of psychological and physiological burden suggests that these individuals may represent a clinically complex, treatment-resistant subtype of MDD. The high rate of antidepressant use (71.5%) further supports this interpretation, underscoring the importance of sustained, multidisciplinary suicide prevention strategies. Our results support the conceptualization of suicidality not as an isolated symptom but as a dynamic, multifactorial process, reinforcing the need for integrated risk assessment strategies in emergency settings, aimed at delivering targeted psychiatric and medical interventions. The clustering of these risk factors highlights the necessity for enhanced screening and longitudinal follow-up beyond the immediate crisis.Another key finding of this study was the high prevalence of abnormal laboratory parameters among patients with MDD presenting with SI, particularly in those with repeated suicide attempts and among male patients. A study by Ceresa et al. 18 investigated gender-based differences in clinical and biochemical profiles among 234 patients hospitalized for unipolar depression. They found that male patients hospitalized for unipolar depression had elevated liver enzymes, creatinine, and hemoglobin levels, indicating gender-specific biochemical profiles. Similarly, Jiang et al. 19 investigated gender-specific differences in clinical and biochemical profiles among first-episode, drug- naïve MDD patients with suicide attempts. They reported that female MDD patients with suicide attempts showed elevated lipid and thyroid profiles, whereas males had lower BMI and free triiodothyronine, suggesting sex-specific metabolic vulnerabilities. In line with these findings, our results revealed significantly higher rates of abnormal ALT, creatinine, hemoglobin, and hematocrit in males, as well as elevated inflammatory markers such as white blood cell and neutrophil counts across the entire sample. Patients with a history of multiple suicide attempts exhibited significantly higher rates of chronic medical conditions, alcohol use disorder, and smoking compared to those without such a history. This supports the notion that suicidality in MDD often emerges within a broader context of physical health deterioration and behavioral risk patterns. Prior studies have linked medical comorbidities such as cardiovascular disease and chronic pain to elevated suicide risk in mood disorders 20,21, likely due to reduced quality of life and cumulative psychological burden. Additionally, alcohol misuse is a well-established proximal risk factor, contributing to disinhibition and affective dysregulation 22. Hughes, highlighted that chronic nicotine use modulates mesolimbic dopaminergic pathways involved in reward processing and increasing impulsivity and mood instability 23. In line with these, our finding of significantly higher smoking rates among patients with multiple suicide attempts supports the hypothesis that smoking may serve as a behavioral marker of shared neurobiological vulnerabilities in reward and impulse regulation. Collectively, these results emphasize the need for comprehensive suicide prevention approaches that extend beyond psychiatric diagnosis to include physical health, substance use, and lifestyle behaviors, especially in emergency settings where acute presentations may obscure chronic risk accumulation.
Limitations
One limitation of this study is the absence of a control group including either MDD patients without suicidality or healthy individuals, which constrains the ability to assess whether the observed clinical and laboratory patterns are specific to SI. Due to the retrospective and observational nature of this study, it is not possible to determine causal relationships between SI and the observed laboratory parameters. Additionally, the acute stress factors inherent in ED presentations could influence laboratory values, confounding the interpretation of results. The MIMIC-IV database lacks details on severity, duration, stressors, and psychiatric assessments. These limitations highlight the need for future prospective, multi-center studies incorporating richer clinical data to validate and expand upon the current findings.
Conclusion
This study presents a multifaceted examination of patients with MDD presenting to the ED with SI, highlighting the interplay between psychiatric comorbidities, behavioral risks, and systemic physiological disturbances. Our findings underscore the heightened vulnerability of individuals with a history of multiple suicide attempts, particularly in males, who are associated not only with elevated rates of psychiatric comorbidity and substance use, but also with systemic physiological alterations observable through routine laboratory assessments. Integrating lab data—especially inflammatory, metabolic, and hematologic—may improve risk assessment and clinical decision-making. By incorporating these biomarkers into risk stratification protocols, clinicians may enhance the early identification of patients at heightened risk for self-harm. Taken together, these observations support the implementation of a multidimensional suicide prevention model that integrates neurocognitive screening, biological monitoring, and continuity of psychiatric care, emphasizing the importance of early identification, multidisciplinary follow-up, and long-term support beyond the point of crisis stabilization in the ED.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Santomauro DF, Mantilla Herrera AM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700-12.
-
Otte C, Gold SM, Penninx BW, et al. Major depressive disorder. Nat Rev Dis Primers. 2016;2:16065.
-
Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46-56.
-
Valkanova V, Ebmeier KP, Allan CL. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2013;150(3):736-44.
-
Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67(5):446-57.
-
Zhang G, Li S, Wang S, Deng F, Sun X, Pan J. The association between serum albumin and depressive symptoms: a cross-sectional study of NHANES data during 2005–2018. BMC Psychiatry. 2023;23(1):448.
-
Al-Marwani S, Batieha A, Khader Y, El-Khateeb M, Jaddou H, Ajlouni K. Association between albumin and depression: a population-based study. BMC Psychiatry. 2023;23(1):780.
-
Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 2008;192(2):98-105.
-
Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci. 2003;4(10):819-28.
-
Oquendo MA, Baca-Garcia E, Mann JJ, Giner J. Issues for DSM-V: suicidal behavior as a separate diagnosis on a separate axis. Am J Psychiatry. 2008;165(11):1383-84.
-
Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. 2014;13(2):153-60.
-
Betz ME, Boudreaux ED, Jacobs DG. Suicide risk screening in emergency departments: Diagnostic accuracy and ideal practices. West J Emerg Med. 2016;17(2):264-70.
-
Boudreaux ED, Camargo CA Jr, Arias SA, et al. Improving suicide risk screening and detection in the emergency department. Am J Prev Med. 2016;50(4):445-53.
-
Postolache TT, Mortensen PB, Tonelli LH. Inflammatory markers and suicide. Curr Top Behav Neurosci. 2008;7:251-68.
-
Johnson AEW, Bulgarelli L, Shen L, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1.
-
Bachmann S. Epidemiology of suicide and the psychiatric perspective. Int J Environ Res Public Health. 2018;15(7):1425.
-
Reneses B, Agüera-Ortiz L, Sevilla-Llewellyn-Jones J, et al. Staging of depressive disorders: Relevance of resistance to treatment and residual symptoms. J Psychiatr Res. 2020;129:234-40.
-
Ceresa A, Esposito CM, Surace T, et al. Gender differences in clinical and biochemical parameters of patients consecutively hospitalized for unipolar depression. Psychiatry Res. 2022;310:114476.
-
Jiang D, Lang X, Wang D, Zhang XY. Gender differences in risk factors for suicide attempts among young, first-episode and drug-naive major depressive disorder patients with anxiety symptoms. Front Psychiatry. 2024;15:1424103.
-
Scott KM, Lim C, Al-Hamzawi A, et al. Association of mental disorders with subsequent chronic physical conditions. JAMA Psychiatry. 2018;73(2):150-8.
-
Tang NKY, Crane C. Suicidality in chronic pain: A review of the prevalence, risk factors, and psychological links. Psychol Med. 2020;50(4):519-32.
-
Darvishi N, Farhadi M, Haghtalab T, Poorolajal J. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: A meta-analysis. PLoS One. 2015;10(5):e0126870.
-
Hughes JR. Smoking and suicide: A brief overview. Drug Alcohol Depend. 2008;98(3):169-78.
Figures
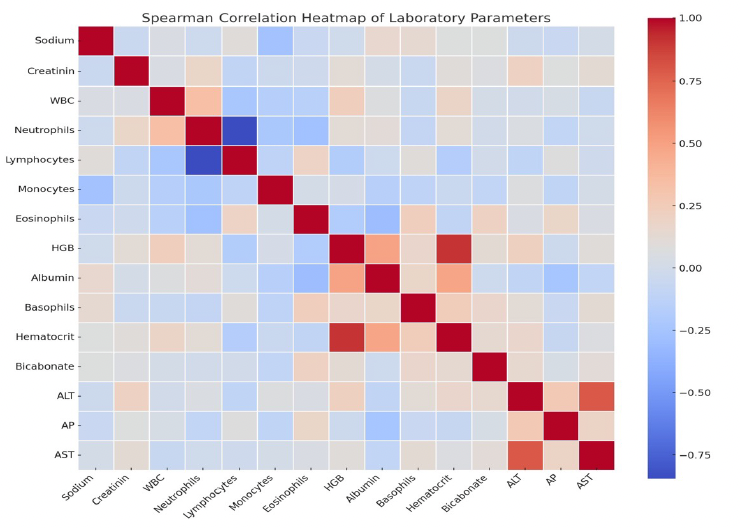
Figure 1. Spearman correlation heatmap of laboratory parameters. Warmer colors (red) indicate positive correlations, while cooler colors (blue) represent negative correlations
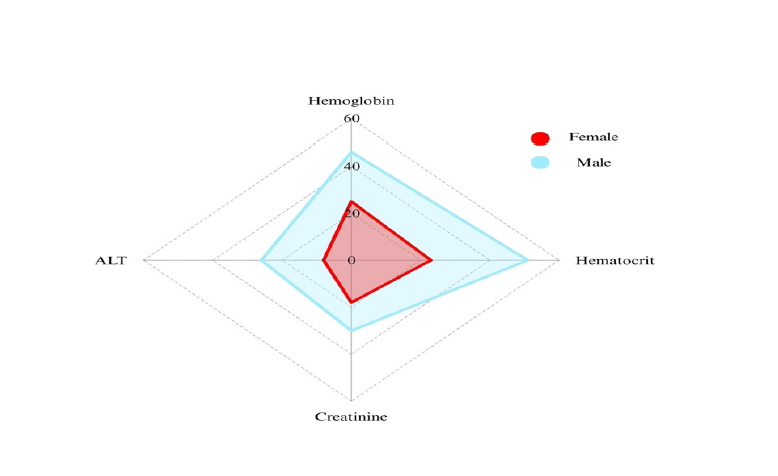
Figure 2. Radar chart of gender differences in abnormal hemoglobin, hematocrit, creatinine and alanine aminotransferase values
Tables
Table 1. Demographic details of the participants
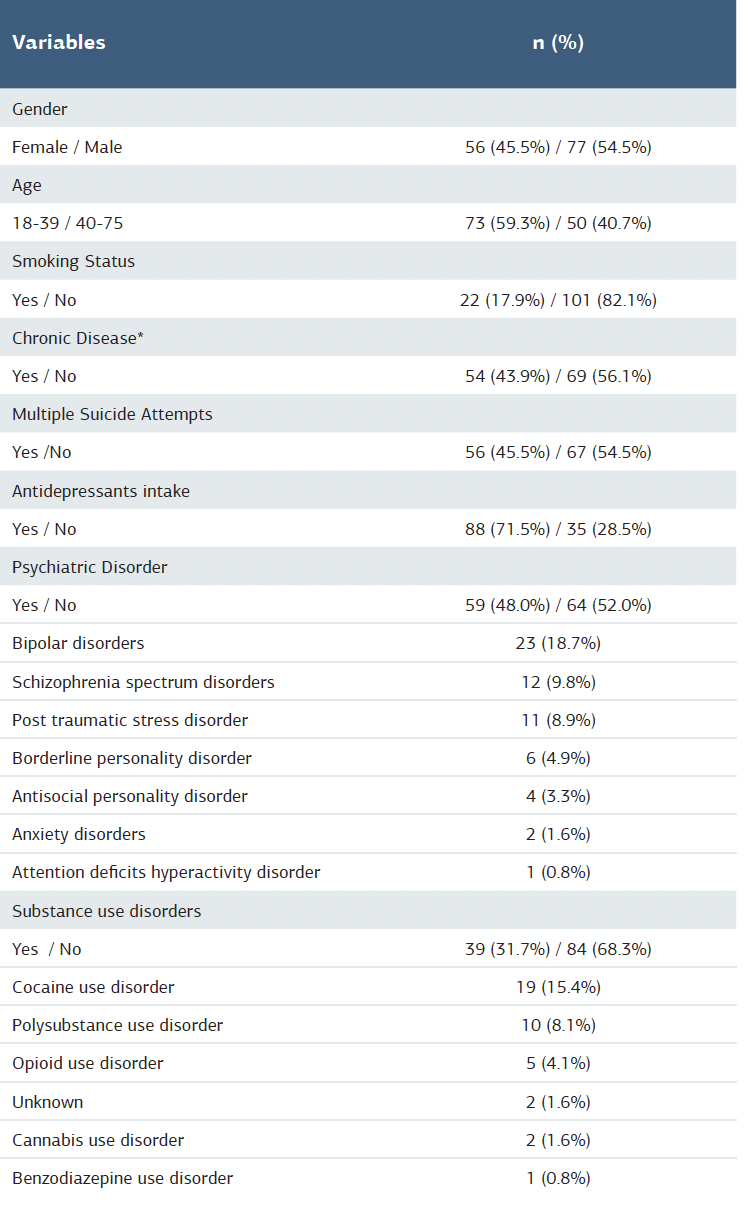
Percentages are based on valid cases per variable (N=123) *Including diabetes, cancer, chronic heart disease, asthma, stroke.
Table 2. Frequency of patients with abnormal laboratory parameters
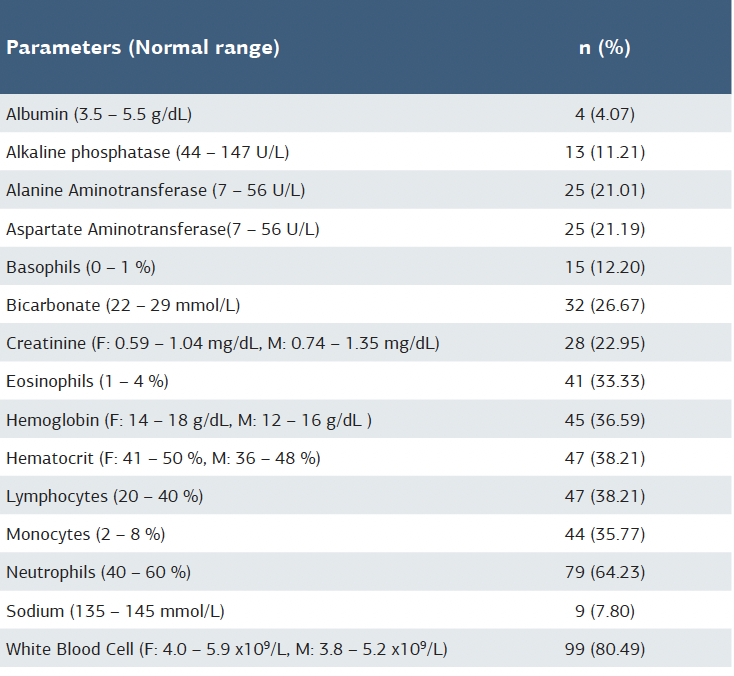
Percentages are based on valid cases per variable (N = 123). F = female; M = male.
Table 3. Comparison of clinical and behavioral characteristics between patients with and without multiple suicide attempts
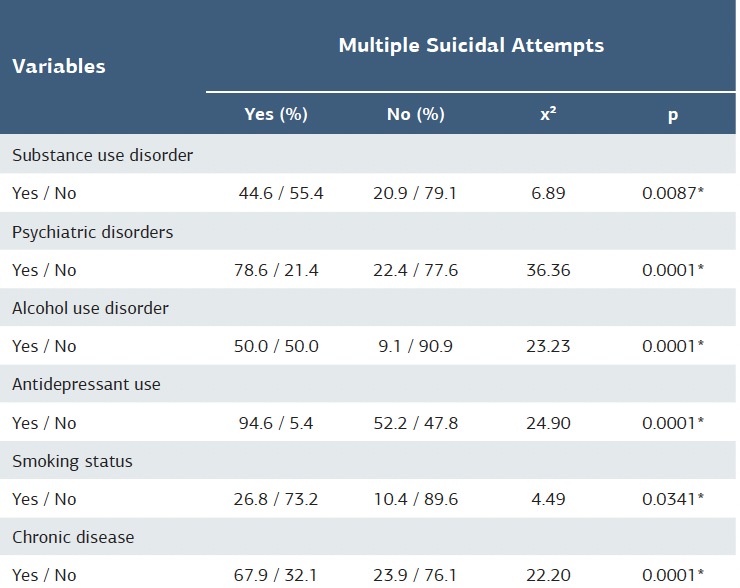
χ²: Chi-square test, *p<0.05
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Melih Çamcı, Nur Efşan Akıncı, Gülsüm Akdeniz. Laboratory biomarkers associated with suicidal ideation in major depressive disorder: A retrospective study in the emergency department. Ann Clin Anal Med 2025;16(9):730-735