
Abstract
AimHepatocellular carcinoma (HCC) is one of the most common cancers worldwide. Liver transplantation (LT) is the only curative treatment that eliminates both the cirrhotic liver and the cancer. Our study aimed to demonstrate the ability of systemic and local inflammatory factors to predict prognosis and long- term survival outcomes for LT.MethodsWe analyzed 220 patients undergoing LT for HCC in two separate transplant centers between January 2012 and December 2024. The primary objectives were overall survival (OS), recurrence-free survival (RFS), and recurrence risk.ResultsThe optimal cutoff values for neutrophil to lymphocyte ratio (NLR) and aspartate aminotransferase/platelet count ratio index (APRI) for OS and RFS were 0.451 and 0.68, respectively. We showed that the APRI > 0.68 (high) group had significantly better overall survival outcomes for RFS and OS. Borderline significance was observed in OS for the NLR > 4.51 group. In particular, tumor size and tumor number were found to be significant factors negatively affecting survival.ConclusionWe determined that a high systemic NLR level was useful for predicting OS, but this was not significant for recurrence or RFS. It is not a useful systemic inflammatory index for screening patients undergoing LT at high risk of recurrence. In our study, a high APRI score was associated with an increased mortality rate. Conversely, a high APRI score was associated with a better RFS. We found that a high APRI value was associated with a better OS.
Keywords
Introduction
HCC is the sixth most common cancer worldwide. As the third most common cause of death, it continues to be an increasingly important health problem.1 Treatment options include LT, surgical resection, and locoregional treatment modalities. LT is one of the most effective treatment modalities for patients with early-stage HCC. LT eliminates both cancer and liver disease, such as cirrhosis. Thus, important risk factors for new tumor formation are eliminated.2 Although HCC patients who undergo LT are selected according to strict selection criteria, the recurrence rate after LT is approximately 10–20%.3 Since this directly affects long-term outcomes, selecting patients with the best probability of survival after LT in transplantation management is extremely important for the efficient use of scarce liver donor resources. Systemic markers associated with fibrosis and inflammation must be taken into consideration in the preoperative evaluation. The importance of changes in systemic inflammation in preoperatively predicting surgical and oncological outcomes in liver cancers, including HCC, has been shown in many studies.4 A number of inflammation- based biomarkers and biomarkers related to the degree of liver fibrosis were developed to predict prognosis.5 One of the most frequently used tools to assess patient outcomes is NLR. High NLR levels were reported to be associated with poor prognosis in patients with HCC who underwent liver resection.6 The influence of tumor-associated neutrophils (TANs) on tumor growth, invasion, and metastasis has been revealed.7 In parallel, there have been significant advances in the relationship between HCC progression and the tumor microenvironment (TME). As a result, NLR has begun to be used as a useful inflammatory marker to predict HCC recurrence.8 Furthermore, several models have been developed that predict liver fibrosis status and HCC-related outcomes, including APRI. To our knowledge, inflammatory markers associated with HCC recurrence can guide clinicians in identifying patients with poor prognosis preoperatively and postoperatively in patients undergoing LT. Numerous prognostic models for HCC have been proposed. Most of these generally incorporate clinicopathological features of the patient and tumor.9 These models often fail to reveal the specific inflammatory factors that influence long-term outcomes. Recent studies evaluating the role of inflammatory biomarkers and markers related to liver fibrosis grade in HCC patients in the context of LT have yielded inconsistent results and remained uncertain regarding their ability to predict survival.10 Our study aimed to demonstrate the ability of systemic and local inflammatory factors to predict prognosis and long-term survival outcomes.
Materials and Methods
For this study, patients undergoing living and deceased donor liver transplantation were recruited consecutively at two separate transplant centers between January 2012 and December 2024. During this period, a total of 1,530 patients underwent LT for any reason. Of these, 220 patients underwent LT for HCC. Inclusion criteria were those who had not received pre-LT radiotherapy or chemotherapy. The exclusion criteria were: 1) patients with concurrent tumors from other organs or metastatic liver tumors,
2) patients with other organ transplantation but missing clinical or follow-up information, and 3) patients with mixed tumors (HCC and cholangiocarcinoma) and recurrent HCC. Ultimately, 200 patients met the inclusion criteria. The primary objectives were OS, RFS, and recurrence risk ratio. The secondary aim was to investigate the relationship between high and low APRI and NLR and demographic and tumor characteristics. Inflammatory markers NLR and APRI were analyzed using cutoff values determined based on the Receiver Operating Characteristic (ROC) curve analysis. Preoperative serum samples were collected one week before liver transplantation in patients with HCC. NLR, a marker of inflammation with demonstrated prognostic value in liver resection for HCC, and APRI, as a non- invasive liver fibrosis marker, were used: APRI = (AST / AST upper limit of normal) / platelet count × 100. Post-LT follow-up was performed every three months using contrast-enhanced computed tomography (CT), AFP. OS was defined as the time from surgery to death or loss of follow-up. RFS was defined as the time from surgery to the detection of recurrence. Post- LT immunosuppressive protocol was performed as previously determined.11Ethical ApprovalThis study was approved by the Ethics Committee of Acıbadem University (Date: 26.06.2025, Decision No:10/380).Statistical AnalysisData were calculated as means, medians, frequencies, and percentages. The Mann–Whitney U test and the Kruskal–Wallis test were used to compare continuous variables. The area under the ROC curve (AUC) was used to determine the optimal cutoff value for RFS and OS analyses. ROC curve analysis was employed to determine optimal cut-off values for APRİ and NLR indices with respect to OS and RFS. Survival probabilities were estimated using the Kaplan–Meier method, and differences between groups were evaluated using the log-rank test. The Youden index was used to select thresholds that provided the best balance between sensitivity and specificity. All statistical analyses were performed using SPSS version 27.0.Reporting GuidelinesThis study was reported according to the STROBE guidelines.
Results
There were no differences in clinic-demographic features (Table 1). We evaluated the relationship between post-LT results and preoperative inflammatory indices (Figure 1). The optimal cutoff values for NLR and APRI for predicting postoperative OS and RFS were 4.51 and 0.68, respectively (Figure 2a,b). Borderline significance was observed in OS for the NLR >4.51 group (Figure 2c). We also analyzed RFS for NLR (Figure 2d).
Considering the relationship between APRI and tumor characteristics well-known to be associated with disease progression, alpha-fetoprotein (AFP) levels were significantly higher in the high APRI group. When prognostic indicators were analyzed, the mortality rate was significantly higher in the low APRI group (36.8% vs. 19.9%) (Figure 2e). Interestingly, RFS was longer in the high APRI group (median: 55 months vs. 35 months) (Figure 2f). Follow-up was significantly longer in the high APRI group (median: 64 months vs. 36 months). Kaplan-Meier analysis produced on the entire cohort showed that the high APRI group had significantly better overall survival outcomes for RFS and OS (Figure 2e,f).
In univariate Cox regression analysis, some clinical features and tumor variables were found to be significantly associated with OS. In particular, tumor size and tumor number were significant factors negatively affecting survival. MVI was also associated with a significantly increased risk of mortality. An APRI ≤0.68 was found to be a significant prognostic factor increasing the risk of death by approximately 2.2-fold. In the analysis for NLR, although survival was better in patients with NLR ≤4.51, the difference was not significant (Table 2).
According to multivariate Cox regression analysis, only APRI ≤0.68 remained a significant independent factor affecting overall survival (p=0.023, HR=2.40, 95% CI: 1.130-5.081). Tumor size and tumor number, although close to the significance threshold, were not statistically significant in multivariate analysis. Similarly, MVI also lost significance in the multivariate model. Other variables were not found to be independent factors affecting OS (Table 2). The lowest p value was found for early-stage tumor differentiation, which trended toward a reduced risk of recurrence (p=0.060, HR=0.235, 95% CI: 0.052-1.062), but did not reach statistical significance (Table 2).
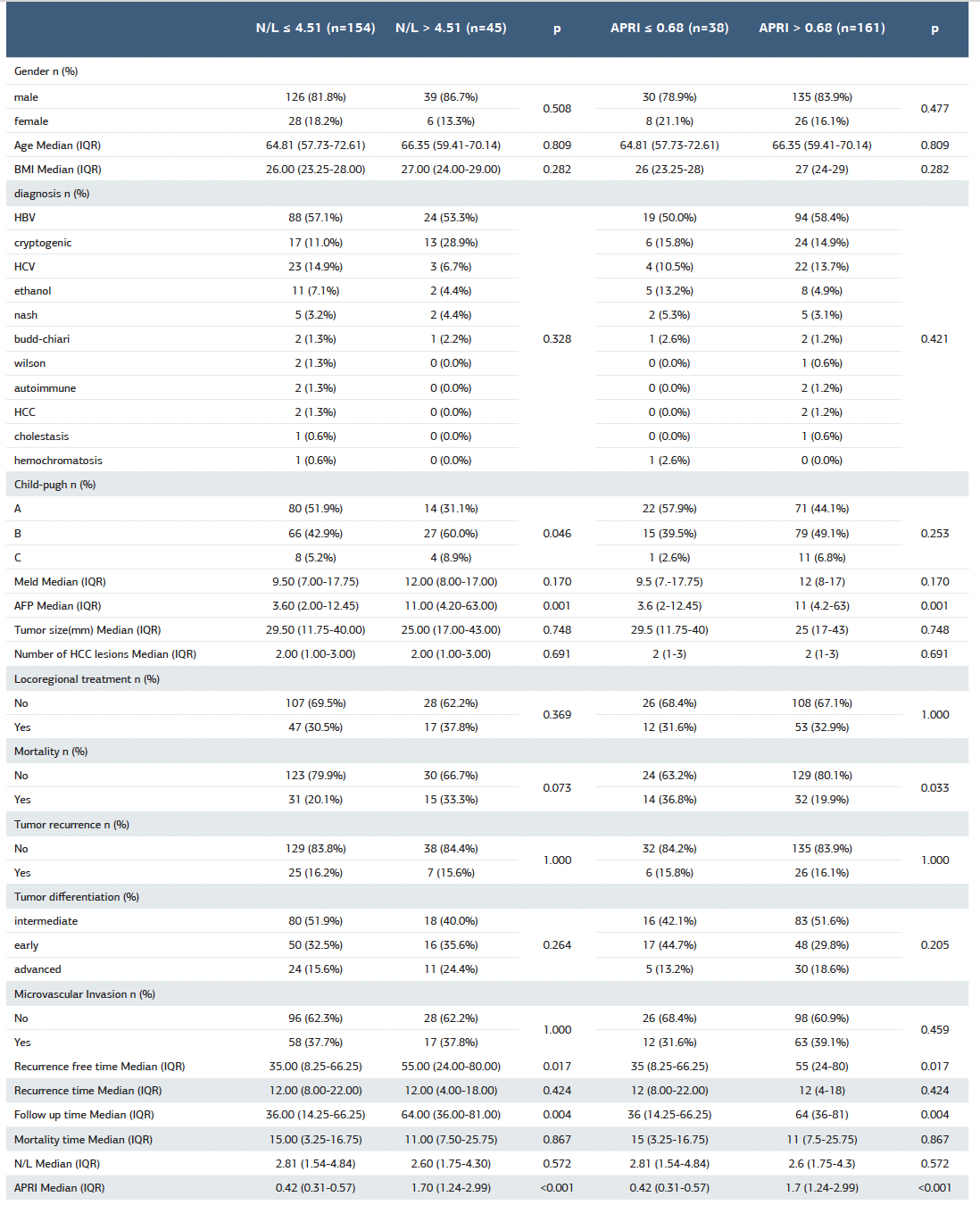
When patient and tumor variables were compared with high and low NLR, no difference was observed in terms of gender, age, and disease etiology, while AFP and CP B and C ratios were found to be higher in high NLR. Similarly, RFS was significantly longer in high NLR. The APRI score, an indicator of fibrosis level, was significantly higher in the group with NLR >4.51. This suggests that high NLR may be associated with advanced liver disease (Table 3).
When disease and tumor characteristics were examined with high and low APRI, a significant association was observed between high AFP and APRI >0.68. While the mortality rate was found to be lower with high APRI, RFS and recurrence-free follow-up time were observed to be significantly longer (Table 3).
AUC values were 0.55 and 0.51 for APRI and NLR, respectively. For OS with APRI ≤0.68, sensitivity was 30.4%, specificity was 84.3%, PPV was 36.8%, NPV was 80.1%, and accuracy was 71.9%. For OS with NLR ≤4.51, sensitivity was 67.4%, specificity was 19.6%, PPV was 20.1%, NPV was 66.7%, and accuracy was 30.7%. In the analysis for RFS, for APRI ≤0.68, sensitivity was 18.8%, specificity was 80.8%, PPV was 15.8%, NPV was 83.9%, and accuracy was 70.9%; for NLR ≤4.51, sensitivity was 78.1%, specificity was 22.8%, PPV was 16.2%, NPV was 84.4%, and accuracy was 31.7%.
Discussion
We also aimed to explore the association of APRI and NLR with OS and RFS in the patients with HCC after LT. We determined that a high systemic NLR level was useful for predicting OS, but this was not significant for recurrence or RFS. It is not a useful systemic inflammatory index for screening patients undergoing LT at high risk of recurrence. In our study, a low APRI score was associated with an increased mortality rate. Conversely, a high APRI score was associated with a better RFS. The time to recurrence was not different between high and low scores. We found that a high APRI value was associated with a better OS. This is inconsistent with other studies showing an association between high APRI and shorter OS.12 However, the results of the analysis for sensitivity, specificity, PPV, and NPV showed that APRI provided high specificity and acceptable accuracy in predicting mortality, but had limited screening power due to its low sensitivity. Based on these results, we demonstrated that while NLR has high sensitivity for mortality, its discriminatory power is limited due to very low specificity and low accuracy. Analysis of tumor recurrence revealed that although APRI has relatively higher specificity, its sensitivity remained low, while NLR, despite its high sensitivity, has low specificity and accuracy. Overall, we can suggest that while APRI and NLR provide some contribution to the prediction of mortality and overall survival, their clinical utility in predicting tumor recurrence is limited due to their low PPV values. While studies showed that an increased APRI score predicts the risk of developing HCC in patients with chronic hepatitis B,13 the findings of studies investigating the relationship between a high APRI and HCC prognosis are inconsistent. Most of these were single-center studies and were limited to specific populations, such as hepatitis B-associated HCC or those following hepatectomy. We also eliminated liver fibrosis and cirrhosis, which are important risk factors for the development of HCC. We reflect the true outcome of the scoring system based on these factors. Our study is also consistent with the conclusion that a low fibrosis index after LT is a poor prognostic factor for HCC, as demonstrated in our previous study.14 APRI, a marker associated with liver fibrosis, were found to be prognostic factors for OS in HCC patients, but were not statistically significant for RFS. Markers related to inflammation and nutrition are known to be prognostic factors in HCC patients undergoing hepatic resection. Of these, high NLR is associated with poor outcomes.15 but whether it is a predictor of poor survival in HCC patients undergoing LT is unclear. We found that high NLR was a poor prognostic marker for OS. These results may be attributable to tumor pathogenesis, study population size, and the varying cutoff values used in previous studies. In our study, we demonstrated for the first time that APRI is an independent prognostic factor in HCC patients undergoing LT. Contrary to other studies, we analyzed whether high APRI levels are definitive predictors of poor survival. Our results showed that NLR and APRI were associated with high CP B and C, liver disease, including advanced cirrhosis, and high AFP reflecting aggressive tumors. Our multivariate results demonstrated that NLR and APRI scores, when combined with established prognostic factors such as MVI, tumor number and size, and AFP, can predict poor OS and RFS before LT in patients with HCC. Tumor aggressiveness is closely related to surgical outcomes. Furthermore, NLR and APRI, both reflecting liver functional capacity and degree of fibrosis, have been shown to be important predictors of poor prognosis in patients undergoing surgery. Our study is a two-center study that included cirrhotic patients from diverse etiologies, encompassing a diverse population. In addition to the group of patients who did not receive preoperative systemic therapy, it also did not include factors that could affect long-term outcomes after surgery, such as ablation, vascular interventional therapy, or molecular-targeting therapy. Systemic lymphocyte count indicates the recipient’s cytotoxic immune response in HCC.16 One of the main reasons for post-LT extrahepatic recurrences is that tumor cells escape immune surveillance with immunosuppressive therapy, which facilitates extrahepatic organ metastasis.17 Serum albumin level is one of the factors that plays a role in the immune response to tumor in addition to nutritional status.18 NLR may affect surgery-related inflammation and the immune response in the transplanted graft in patients undergoing LT.19 In parallel, a high NLR increases the risk of early complications, including tumor recurrence. This is associated with decreased survival and poor prognosis in the post-LT period.20
According to these results, LT in patients with HCC should be individualized based on the clinical and pathological characteristics of the tumor, organ suitability, and the comparison of donor risk and recipient benefit expectations. Numerous HCC prognostic factors and models were identified in the past decades. Most of these were based on clinic- pathological, donor, and recipient factors.9,21 NLR is one of the inflammation-related risk factors, reflecting both the antitumoral effect of the immune system and the systemic inflammatory state. Systemic inflammatory markers can be used to predict recurrence in high-risk patients. Neutrophils are classified according to their functional phenotypes in different inflammatory states. Although there are studies based on whether it promotes tumor progression or inhibits it due to the complex diversity.22 However, NLR and APRI-based results should be interpreted with caution because these biomarkers are influenced by several factors. Neoplasms such as HCC can influence the inflammatory and immune responses of patients.23 Identifying a high-risk population by analyzing NLR and APRI in LT for HCC also constitutes a precise advantage in reducing failure-to-rescue.
Inflammatory parameters are reproducible, easy to perform, and cost-effective because they have very low variability even in complete blood counts that include different leukocyte types.11 Complete blood count results and associated inflammatory markers could have been affected by acute rejection, immunosuppressive or systemic chemotherapy, and infections. However, HCC patients did not receive systemic therapy before LT, and surgery was not performed until the infection was controlled. Therefore, our results were not affected by these factors.
Limitations
To assess cutoff values for poor long-term survival, curve analysis of NLR and APRI may not be fully representative as this may not provide accurate long-term predictive value for LT outcomes. However, large-scale, multicenter studies would be beneficial to investigate better prognostic models for reducing postoperative recurrence and developing targeted therapies.
Conclusion
Our study demonstrated the prognostic importance of inflammatory and fibrosis markers in patients with HCC undergoing LT. We demonstrated that low APRI and high NLR are associated with poor long-term outcomes in LT for HCC. The APRI score is an independent prognostic factor in HCC patients undergoing LT. NLR and APRI scores may be clinically helpful in making treatment decisions and predicting post-LT oncological outcomes in HCC patients. One of the limitation of this work is the retrospective nature of the data. They may affect the accuracy of the recorded biochemical and clinical parameters. According to these considerations, LT for HCC patients should be based on clinic-pathological characteristics, organ availability and the cost-benefit ratio of LT. Further research is needed to confirm the effectiveness of the markers as prognostic factor in HCC patients who underwent LT and to identify any interactions with other risk factors and outcome predictors.
Abbreviations
AFP: Alpha-fetoprotein
APRI: Aspartate aminotransferase-to-platelet ratio index
AUC: Area under the curve
HCC: Hepatocellular carcinoma
LT: Liver transplantation
MVI: Microvascular invasion
NLR: Neutrophil-to-lymphocyte ratio
NPV: Negative predictive value
OS: Overall survival
PPV: Positive predictive value
RFS: Recurrence-free survival
ROC: Receiver operating characteristic
References
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. doi:10.3322/caac.21834
- Hill A, Olumba F, Chapman W. Transplantation for hepatocellular carcinoma. Surg Clin North Am. 2024;104(1):103-111. doi:10.1016/j.suc.2023.09.002
- Bhangui P, Allard MA, Vibert E, et al. Salvage versus primary liver transplantation for early hepatocellular carcinoma: do both strategies yield similar outcomes? Ann Surg. 2016;264(1):155-163. doi:10.1097/sla.0000000000001442
- Harimoto N, Yoshizumi T, Shimagaki T, et al. Inflammation-based prognostic score in patients with living donor liver transplantation for hepatocellular carcinoma. Anticancer Res. 2016;36(10):5537-5542. doi:10.21873/anticanres.11137
- Yamamoto M, Kobayashi T, Kuroda S, et al. Verification of inflammation-based prognostic marker as a prognostic indicator in hepatocellular carcinoma. Ann Gastroenterol Surg. 2019;3(6):667-675. doi:10.1002/ags3.12286
- Chen JL, Guo L, Wu ZY, et al. Prognostic value of circulating tumor cells combined with neutrophil-lymphocyte ratio in patients with hepatocellular carcinoma. World J Gastrointest Oncol. 2024;16(2):372-385. doi:10.4251/wjgo.v16.i2.372
- Geh D, Leslie J, Rumney R, Reeves HL, Bird TG, Mann DA. Neutrophils as potential therapeutic targets in hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2022;19(4):257-273. doi:10.1038/s41575-021-00568-5
- Chen H, Zhou XH, Li JR, et al. Neutrophils: driving inflammation during the development of hepatocellular carcinoma. Cancer Lett. 2021;522:22-31. doi:10.1016/j.canlet.2021.09.011
- Qu WF, Tian MX, Lu HW, et al. Development of a deep pathomics score for predicting hepatocellular carcinoma recurrence after liver transplantation. Hepatol Int. 2023;17(4):927-941. doi:10.1007/s12072-023-10511-2
- Yugawa K, Maeda T, Nagata S, et al. A novel combined prognostic nutritional index and aspartate aminotransferase-to-platelet ratio index-based score can predict the survival of patients with hepatocellular carcinoma who undergo hepatic resection. Surg Today. 2022;52(7):1096-1108. doi:10.1007/s00595-021-02440-0
- Pascale MM, Frongillo F, Vasta P. Significance of the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio as prognostic predictors after liver transplantation. World J Transplant. 2025;15(2):100157. doi:10.5500/wjt.v15.i2.100157
- Li J, Chen M, Cai W, Yin D. Development and validation of a risk prediction model based on inflammatory and nutritional composite indicators for posthepatectomy liver failure following radical resection of hepatocellular carcinoma. J Inflamm Res. 2025;18:5261-5279. doi:10.2147/jir.s515918
- Paik N, Sinn DH, Lee JH, et al. Noninvasive tests for liver disease severity and the hepatocellular carcinoma risk in chronic hepatitis B patients with low-level viremia. Liver Int. 2018;38(1):68-75. doi:10.1111/liv.13489
- Bati İB, Tuysuz U, Eygi E. Prognostic significance of hemoglobin, albumin, lymphocyte, and platelet score in liver transplantation for hepatocellular carcinoma. Curr Oncol. 2025;32(8):464. doi:10.3390/curroncol32080464
- Gao F, Li X, Geng M, et al. Pretreatment neutrophil-lymphocyte ratio: an independent predictor of survival in patients with hepatocellular carcinoma. Medicine (Baltimore). 2015;94(11). doi:10.1097/md.0000000000000639
- Ha SY, Choi S, Park S, et al. Prognostic effect of preoperative neutrophil-lymphocyte ratio is related with tumor necrosis and tumor-infiltrating lymphocytes in hepatocellular carcinoma. Virchows Arch. 2020;477(6):807-816. doi:10.1007/s00428-020-02841-5
- Chen J, Li H, Zhuo J, et al. Impact of immunosuppressants on tumor pulmonary metastasis: new insight into transplantation for hepatocellular carcinoma. Cancer Biol Med. 2024;21(11):1033-1049. doi:10.20892/j.issn.2095-3941.2024.0267
- Goh MJ, Kang W, Jeong WK, et al. Prognostic significance of cachexia index in patients with advanced hepatocellular carcinoma treated with systemic chemotherapy. Sci Rep. 2022;12(1):7647. doi:10.1038/s41598-022-11736-1
- Kim KS, Kim JH, Kwon HM, et al. Neutrophilia is more predictive than increased white blood cell counts for short-term mortality after liver transplantation in patients with acute-on-chronic liver failure. Anesth Pain Med. 2023;18(4):389-396. doi:10.17085/apm.23048
- Dai Y, Feng Q, Huang J. A new nomogram use neutrophil-to-lymphocyte ratio and fibrinogen-to-lymphocyte ratio to predict the recurrence of colorectal adenoma. J Gastrointest Oncol. 2023;14(4):1898-1909. doi:10.21037/jgo-23-135
- Qi LN, Ma L, Wu FX, et al. Clinical implications and biological features of a novel postoperative recurrent HCC classification: a multicentre study. Liver Int. 2022;42(10):2283-2298. doi:10.1111/liv.15363
- Cui C, Chakraborty K, Tang XA, et al. Neutrophil elastase selectively kills cancer cells and attenuates tumorigenesis. Cell. 2021;184(12):3163-3177.e21. doi:10.1016/j.cell.2021.04.016
- Xiao Y, Zhu G, Xie J, et al. Pretreatment neutrophil-to-lymphocyte ratio as prognostic biomarkers in patients with unresectable hepatocellular carcinoma treated with hepatic arterial infusion chemotherapy combined with lenvatinib and camrelizumab. J Hepatocell Carcinoma. 2023;10:2049-2058. doi:10.2147/jhc.s432134
Tables
Table 1. Demographic and baseline characteristics of the total cohort
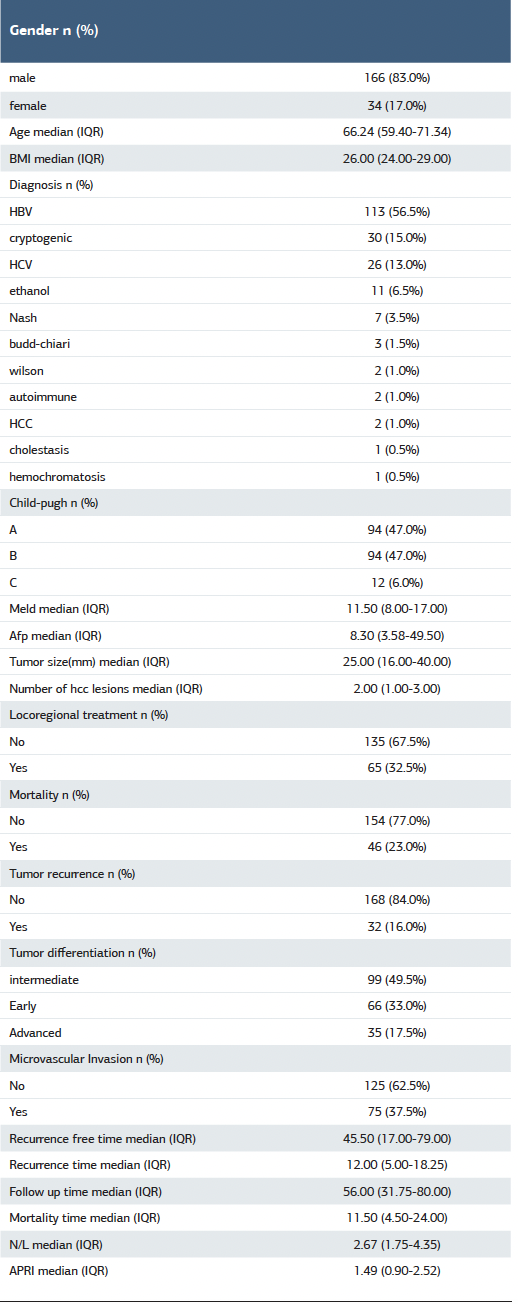
Table 2. Univariate and multivariate COX regression analysis of factors associated with overall survival and recurrence-free survival
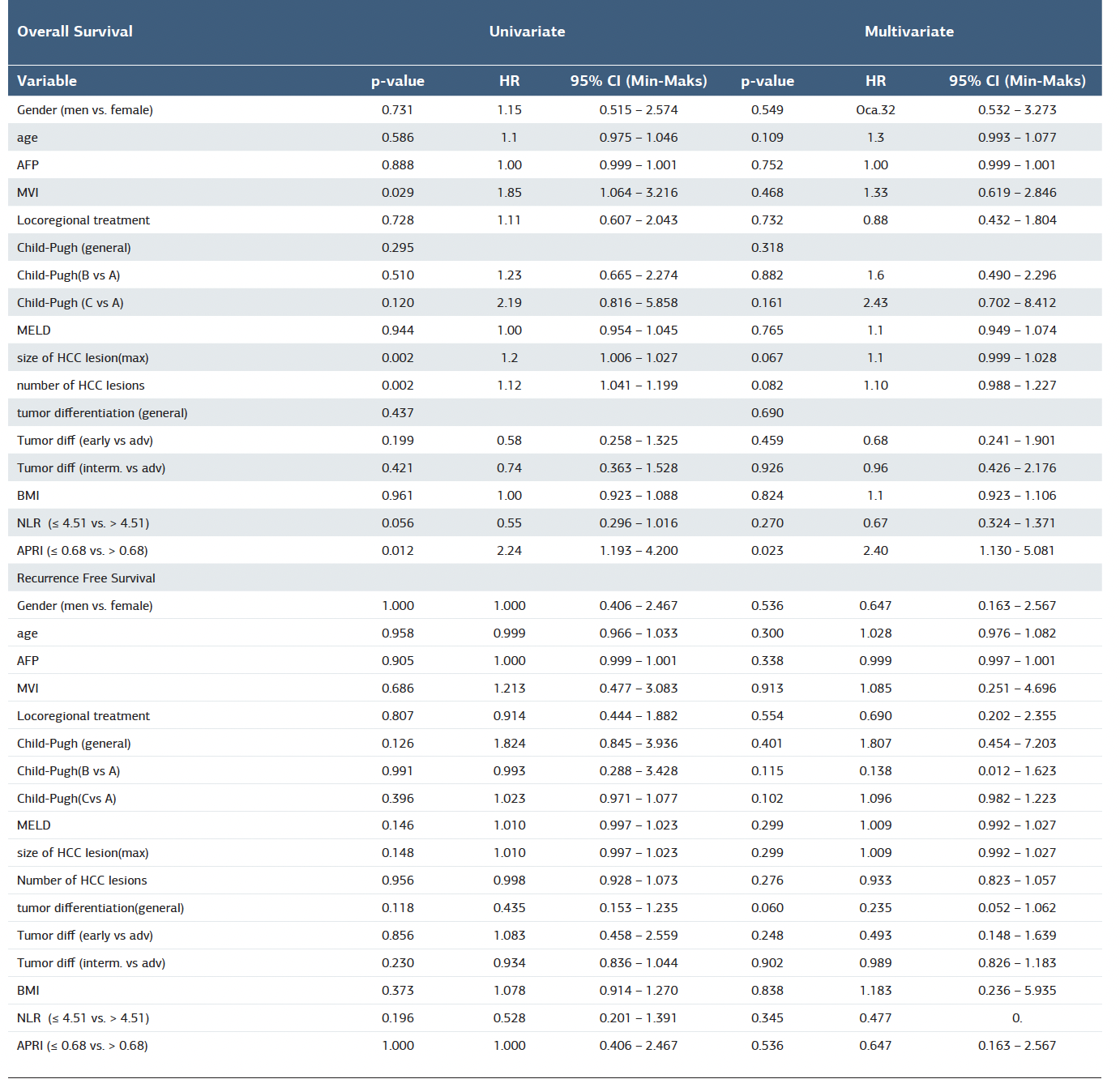
Table 3. Relationship between high and low NLR and APRI and demographic and tumor characteristics
Figures
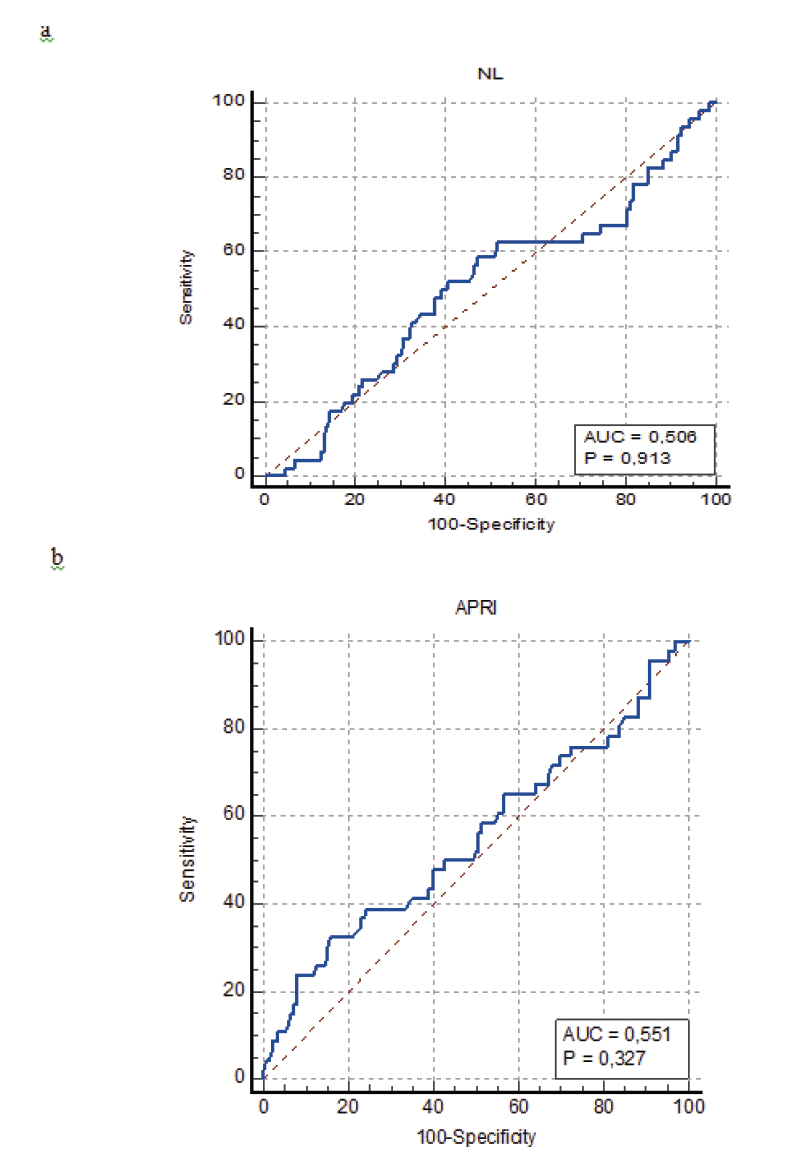
Figure 1. The Receiver Operating Characteristic (ROC) curves explore the value of preoperative NLR and APRI in predicting the long-term prognosis in Liver Transplantation (LT) for Hepatocellular Carcinoma (HCC). (a) The value of ROC in predicting overall survival in LT for HCC. (b) The value of ROC in predicting disease-free survival in LT for HCC
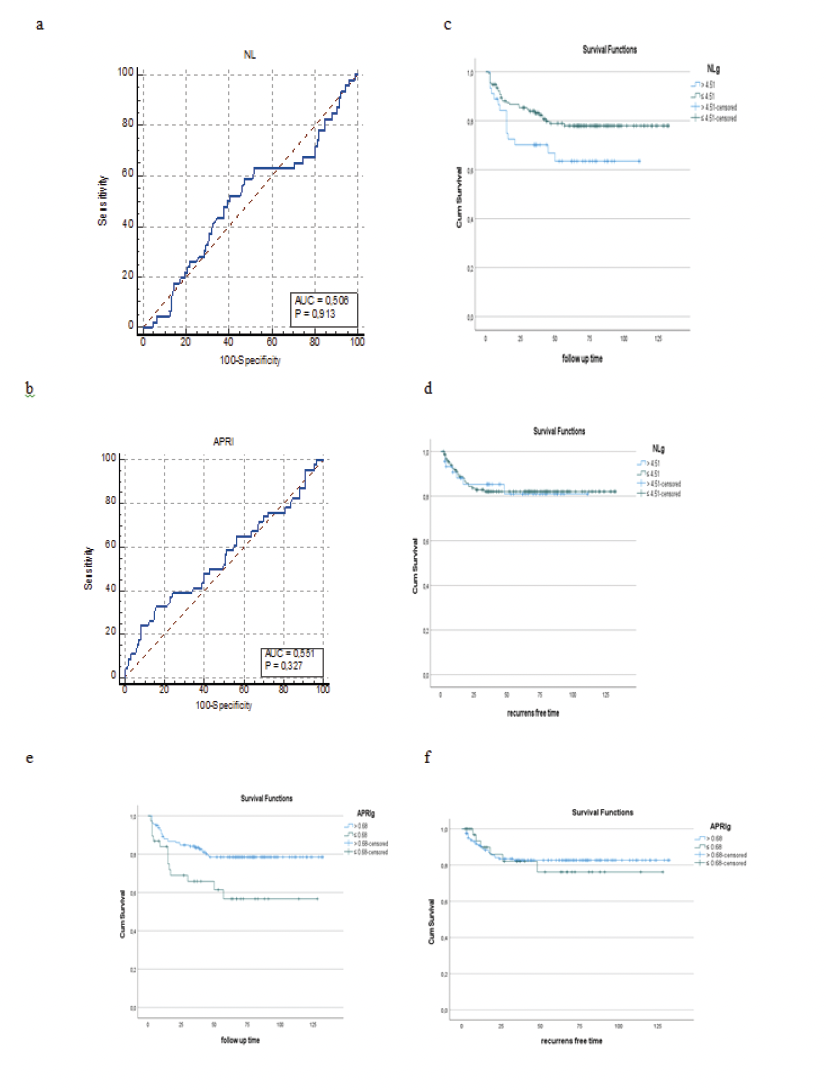
Figure 2. Receiver operating characteristic curve analysis of the preoperative NLR and APRI. a) 4.51 for the NLR b) 0.68 for the APRI. Overall and disease-free survival of patients after liver transplantation for HCC according to the NLR-APRI score in HCC patients from the entire cohort c) overall survival for NLR d) recurrence-free survival for NLR e) overall survival for APRI f) recurrence-free survival for APRI
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İmam Bakır Batı, Umut Tüysüz. Prognostic significance of APRI index and neutrophil/lymphocyte ratio in hepatocellular carcinoma patients undergoing liver transplantation. Ann Clin Anal Med 2025;16(10):752-758. doi:10.4328/ACAM.22861
Publication History
- Received:
- 22.08.2025
- Accepted:
- 22.09.2025
- Published Online:
- 30.09.2025
- Printed:
- 01.10.2025