
Incidental pathological findings in cholecystectomy: a single-center retrospective analysis
Incidental findings in cholecystectomy
Authors
Abstract
AimChronic cholecystitis and cholelithiasis are the most frequently encountered pathologies in cholecystectomy specimens; however, additional histopathological findings that are not clinically suspected may incidentally be detected. This study aimed to evaluate the frequency and distribution of incidental pathological findings in patients who underwent cholecystectomy at a single center.
MethodsThe data of 3,084 patients who underwent cholecystectomy at our institution between January 2021 and December 2024, and for whom pathology reports were available, were retrospectively analyzed. Histopathological diagnoses other than chronic cholecystitis, acute cholecystitis, and cholelithiasis were considered incidental findings. These findings were classified according to their types, and their proportions were calculated.
ResultsIncidental pathological findings were detected in 390 of 3,084 cases (12.65%). The most frequent incidental lesions were metaplasia (n = 182, 46.6%), adenomyomatous hyperplasia (n = 79, 20.3%), and cholesterol polyps (n = 77, 19.7%). Less common findings included xanthogranulomatous cholecystitis (n = 23, 5.9%), dysplasia (n = 18, 4.6%), and adenocarcinoma (n = 11, 2.8%). Among the adenocarcinoma cases, 81.8% occurred in women, with a mean age of 67.2 years.
ConclusionIncidental pathological findings are observed at a noteworthy frequency in cholecystectomy specimens. The presence of clinically significant lesions such as metaplasia, dysplasia, and adenocarcinoma underscores the importance of routine histopathological examination of all gallbladder specimens.
Keywords
Introduction
Gallbladder diseases, particularly cholelithiasis and chronic cholecystitis, are among the most common gastrointestinal surgical indications worldwide.1 The prevalence of cholelithiasis varies geographically, being reported in approximately 10–15% of the adult population in Western countries, while higher rates have been documented in certain regions such as Türkiye.2 Chronic inflammation related to gallstones can drive mucosal changes that may ultimately progress to carcinoma.3
Cholecystectomy is currently regarded as the gold-standard surgical treatment for symptomatic cholelithiasis and its complications.4 Postoperative histopathological examination not only confirms the diagnosis but also allows the detection of incidental pathologies that may remain clinically silent and undetectable on imaging studies.5 These incidental findings can be categorized into benign alterations (adenomyomatosis, cholesterol polyps), preneoplastic lesions (metaplasia, dysplasia), and malignant tumors (adenocarcinoma).6 Gallbladder carcinoma is thought to arise mainly through chronic inflammation associated with gallstones, along with precursor lesions such as biliary intraepithelial neoplasia (BilIN), intracholecystic papillary neoplasm (ICPN), and pyloric gland adenoma (PGA), which are considered sequential steps in the metaplasia–dysplasia–carcinoma pathway.7 These lesions provide important insights into tumor biology and may offer opportunities for earlier detection.
Within this pathological spectrum, the clinical significance of incidental findings becomes particularly evident when preneoplastic or malignant lesions are identified. Gallbladder adenocarcinoma is most often diagnosed at an advanced stage and is associated with a poor prognosis; however, when incidentally detected at an early stage, surgical resection can achieve curative outcomes.8 In the literature, the reported incidence of incidentally identified adenocarcinoma ranges between 0.2% and 2.0%, emphasizing the indispensable role of routine histopathological evaluation of cholecystectomy specimens.9
Materials and Methods
This retrospective study included all patients who underwent cholecystectomy at our institution between January 2021 and December 2024 and for whom pathology reports were available. Inclusion criteria consisted of cases with complete pathology reports and those who underwent cholecystectomy for gallbladder pathology. Exclusion criteria were incomplete pathology reports and cases in which no additional histopathological finding other than chronic or acute cholecystitis and cholelithiasis was identified.
In this study, incidental pathological findings were defined as additional histopathological diagnoses other than chronic cholecystitis, acute cholecystitis, and cholelithiasis. The detected findings were classified as adenocarcinoma, adenomyomatous hyperplasia, cholesterol polyps, metaplasia, dysplasia, xanthogranulomatous cholecystitis, and other rare lesions.
Ethical ApprovalThis study was approved by the Ethics Committee of Malatya Turgut Özal University (Date: 03.06.2025, Decision No: E-30785963-020-307299).
Statistical AnalysisData analysis was performed using SPSS Statistics v.26.0 (IBM Corp., Armonk, NY, USA). Continuous variables (e.g., age) were assessed for normality using the Kolmogorov–Smirnov test. Normally distributed data were expressed as mean ± standard deviation (SD), while non-normally distributed data were presented as median (minimum–maximum).
Categorical variables (sex, presence of incidental findings, and types of findings) were presented as counts and percentages. Comparisons between categorical variables were performed using the chi-square test or Fisher’s exact test when the expected cell counts were small. For continuous variables, the independent samples t-test was used for normally distributed data, while the Mann–Whitney U test was applied for non- normally distributed data.
Additionally, the relationship between types of incidental findings and demographic variables such as age and sex was specifically examined. A p-value of <0.05 was considered statistically significant in all analyses.
Reporting GuidelinesThis study was reported according to the STROBE guidelines.
Results
Among the 3,084 cholecystectomy cases included in the study, incidental pathological findings were identified in 390 patients (12.65%). The most frequent lesion was metaplasia, detected in 182 cases (46.6%), followed by adenomyomatous hyperplasia (n = 79, 20.3%) and cholesterol polyps (n = 77, 19.7%). Less common findings included xanthogranulomatous cholecystitis (n = 23, 5.9%), dysplasia (n = 18, 4.6%), and adenocarcinoma (n = 11, 2.8%) (Table 1).
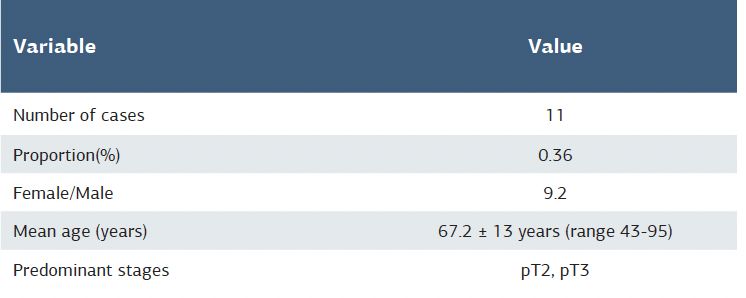
Adenocarcinoma cases were analyzed separately. This tumor was detected in 11 patients (0.36%). Of these, nine were women (81.8%) and two were men (18.2%), with a mean age of 67.2 ± 13 years (range: 43-95 years). Although none of the patients had a preoperative suspicion of malignancy, most of the cases with available staging data were classified as pT2-pT3 (Table 2).
In total, incidental pathological findings were identified in 390 patients (12.65%). In multivariable logistic regression analysis including age and sex, increasing age was found to be independently associated with incidental findings (OR = 1.02 per year; 95% CI: 1.01-1.03; p=0.004). Female sex, on the other hand, was not significantly associated with the presence of incidental lesions (OR = 1.12; 95% CI: 0.89-1.41; p=0.32).
Discussion
In the present study, the rate of incidental pathological findings in cholecystectomy specimens was determined to be 12.65%. This rate is clinically relevant, particularly considering the presence of preneoplastic and malignant lesions. The most frequently encountered incidental finding in our series was metaplasia, which has been reported in the literature to arise in the setting of chronic inflammation and to represent an important step in the pathogenesis of gallbladder adenocarcinoma.10 Dysplasia, on the other hand, is directly associated with carcinogenesis, and its detection warrants close clinical surveillance and, when necessary, additional surgical evaluation.11 Incidental dysplasia is generally managed with simple cholecystectomy if margins are negative, though close follow- up may be advisable in elderly patients.12 For incidental adenocarcinoma, management depends on tumor stage: pT1a is cured with cholecystectomy alone, whereas pT1b or higher requires extended resection with lymphadenectomy.13
Furthermore, multivariate analysis revealed that advancing age was independently associated with incidental findings, whereas sex showed no significant effect. This suggests that elderly patients represent a higher-risk group for preneoplastic and malignant changes, underscoring the value of routine histopathological evaluation in this population.14
Another important aspect in the prevention and early detection of gallbladder carcinoma is the management of gallbladder polyps. Frequently detected incidentally, these lesions are clinically relevant because of their premalignant potential. Current guidelines recommend that polyps ≤ 5–6 mm without risk factors do not require follow-up, whereas 6–9 mm polyps with additional risk factors should be monitored by ultrasound at 6, 12, and 24 months. Polyps ≥ 10 mm are generally regarded as an indication for cholecystectomy.15 Incorporating these recommendations into clinical practice is particularly important in settings such as ours, where incidental pathological findings were not uncommon, as it may help reduce unnecessary surgical procedures while ensuring timely treatment of high- risk patients.
In our study, the incidence of adenocarcinoma was 0.36%, which is consistent with the 0.2–2.0% range reported in the literature.16 The majority of cases occurred in elderly female patients, and none had preoperative suspicion of malignancy. This finding clearly highlights the diagnostic value and clinical importance of routine histopathological examination of cholecystectomy specimens.
Gallbladder adenocarcinoma is a malignancy that can be completely cured with surgical resection when detected at an early stage; however, due to its frequent diagnosis at advanced stages, the prognosis remains poor.17 Preoperative radiological examinations are often insufficient in terms of sensitivity, particularly in the presence of small lesions, and as a result, malignant cases can be easily overlooked.18 In this context, routine histopathological examination not only facilitates the identification of malignant tumors but also allows for the recognition of preneoplastic lesions, thereby contributing to the implementation of appropriate surgical or medical strategies before progression to advanced disease.19
In some centers, it has been suggested that routine histopathological examination may be omitted for gallbladder specimens that appear macroscopically normal, primarily due to cost constraints or workload considerations.20 However, both our study and similar reports have demonstrated incidental cases of adenocarcinoma and dysplasia, clearly indicating that such an approach carries significant clinical risks.21 In countries with a high prevalence of cholelithiasis, foregoing histopathological evaluation may result in a substantial number of missed diagnoses and late-stage detections.
Although routine histopathological examination of all cholecystectomy specimens may raise concerns regarding cost and workload, its value in detecting clinically silent premalignant and malignant lesions outweighs the economic burden, especially in regions with high gallstone disease prevalence. From a health policy perspective, modeling studies show that in a cohort of 10,000 patients, routine histology can yield an additional 12 life years at an incremental cost of approximately €76,500 per life year gained compared with macroscopic selective approaches.22 In low-incidence settings, however, selective histology may offer a more cost-effective balance between diagnostic yield and resource use.
Therefore, international guidelines and numerous studies recommend the routine histopathological assessment of all cholecystectomy specimens as the gold-standard approach.23
Limitations
The main limitations of this study are its retrospective and single-center design. In addition, radiological–pathological correlations were not systematically evaluated, which may have provided further insight into the preoperative detectability of incidental lesions. Nevertheless, the large sample size and the systematic histopathological evaluation of all specimens represent the major strengths of our study.
Conclusion
In this study, the rate of incidental pathological findings in cholecystectomy specimens was determined to be 12.65%, with clinically significant lesions such as metaplasia, dysplasia, and adenocarcinoma among the findings. Notably, the detection of adenocarcinoma in 0.36% of cases underscores the presence of malignant lesions that may remain undiagnosed in the preoperative period.
Routine histopathological examination facilitates not only the identification of malignancies but also the recognition of preneoplastic alterations, thereby contributing to the planning of appropriate surgical and follow-up strategies. Therefore, the histopathological evaluation of all gallbladder specimens remains indispensable, both for individual patient management and from a broader public health perspective.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Malatya Turgut Özal University (Date: 2025-06-03, No: E-30785963-020-307299)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
References
-
Wang X, Yu W, Jiang G, et al. Global epidemiology of gallstones in the 21st century: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2024;22(8):1586-1595. doi:10.1016/j.cgh.2024.01.051
-
Piovani D, Nikolopoulos GK, Aghemo A, et al. Environmental risk factors for gallbladder cancer: field-wide systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2025;23(9):1500-1513. doi:10.1016/j.cgh.2024.07.046
-
Afzal A, Liu YY, Noureen A, et al. Epidemiology of gallbladder cancer and its prevalence worldwide: a meta-analysis. Orphanet J Rare Dis. 2025;20(1):143. doi:10.1186/s13023-025-03652-0
-
Roy DK, Sheikh R. A systematic review and meta-analysis of the outcomes of laparoscopic cholecystectomy compared with the open procedure in patients with gallbladder disease. Avicenna J Med. 2024;14(1):3-21. doi:10.1055/s-0043-1777710
-
Jamal Z, Yu Z, Zafar N, Li D. Reconsidering routine histopathological examination of gallbladder specimens in cholecystectomy: optimizing clinical practice and resource management. Cureus. 2024;16(7). doi:10.7759/cureus.64762
-
Riddell ZC, Corallo C, Albazaz R, Foley KG. Gallbladder polyps and adenomyomatosis. Br J Radiol. 2023;96(1142):20220115. doi:10.1259/bjr.20220115
-
Fukumura Y, Rong L, Maimaitiaili Y, et al. Precursor lesions of gallbladder carcinoma: disease concept, pathology, and genetics. Diagnostics (Basel). 2022;12(2):341. doi:10.3390/diagnostics12020341
-
Miao W, Liu F, Guo Y, Zhang R, Wang Y, Xu J. Research progress on prognostic factors of gallbladder carcinoma. J Cancer Res Clin Oncol. 2024;150(10):447. doi:10.1007/s00432-024-05975-0
-
Zeng D, Wang Y, Wen N, Lu J, Li B, Cheng N. Incidental gallbladder cancer detected during laparoscopic cholecystectomy: conversion to extensive resection is a feasible choice. Front Surg. 2024;11:1418314. doi:10.3389/fsurg.2024.1418314
-
Bojan A, Foia LG, Vladeanu MC, et al. Understanding the mechanisms of gallbladder lesions: a systematic review. Exp Ther Med. 2022;24(3):604. doi:10.3892/etm.2022.11541
-
Pavlidis ET, Galanis IN, Pavlidis TE. New trends in diagnosis and management of gallbladder carcinoma. World J Gastrointest Oncol. 2024;16(1):13-29. doi:10.4251/wjgo.v16.i1.13
-
Nakanuma Y, Kakuda Y, Sugino T, Sato Y, Fukumura Y. Pathologies of precursor lesions of biliary tract carcinoma. Cancers (Basel). 2022;14(21):5358. doi:10.3390/cancers14215358
-
Feo CF, Ginesu GC, Fancellu A, et al. Current management of incidental gallbladder cancer: a review. Int J Surg. 2022;98:106234. doi:10.1016/j.ijsu.2022.106234
-
Wu X, Li B, Zheng C, Liu W, Hong T, He X. Incidental gallbladder cancer after laparoscopic cholecystectomy: incidence, management, and prognosis. Asia Pac J Clin Oncol. 2020;16(3):158-164. doi:10.1111/ajco.13308
-
Kamaya A, Fung C, Szpakowski JL, et al. Management of incidentally detected gallbladder polyps: Society of Radiologists in Ultrasound Consensus Conference recommendations. Radiology. 2022;305(2):277-289. doi:10.1148/radiol.213079
-
Chaturvedi A, Misra S, Chaudhary S, et al. Treatment outcomes of incidental gallbladder cancer: results from a high-volume tertiary care centre in North India. Indian J Surg Oncol. 2024;15(suppl 2):204-211. doi:10.1007/s13193-024-01937-7
-
Piñeros M, Vignat J, Colombet M, et al. Global variations in gallbladder cancer incidence: what do recorded data and national estimates tell us? Int J Cancer. 2025;156(7):1358-1368. doi:10.1002/ijc.35232
-
Foley KG, Lahaye MJ, Thoeni RF, et al. Management and follow-up of gallbladder polyps: updated joint guidelines between the ESGAR, EAES, EFISDS, and ESGE. Eur Radiol. 2022;32(5):3358-3368. doi:10.1007/s00330-021-08384-w
-
Arumugam S, Aggarwal S. A narrative review of selective versus routine histopathological examination of gallbladders in low-risk patients. Cureus. 2025;17(6). doi:10.7759/cureus.86609
-
Hasan A, Nafie K, Aldossary MY, et al. Unexpected histopathology results following routine examination of cholecystectomy specimens: how big and how significant? Ann Med Surg (Lond). 2020;60:425-430. doi:10.1016/j.amsu.2020.11.019
-
Alabi A, Arvind AD, Pawa N, Karim S, Smith J. Incidental gallbladder cancer: routine versus selective histological examination after cholecystectomy. Surg J (N Y). 2021;7(1). doi:10.1055/s-0040-1722175
-
Lundgren L, Henriksson M, Andersson B, Sandström P. Cost-effectiveness of gallbladder histopathology after cholecystectomy for benign disease. BJS Open. 2020;4(6):1125-1136. doi:10.1002/bjs5.50325
-
Kim M, Vengatesan K, Aploks K, Thompson K, Dong X, Seshadri R. National cancer database analysis of gallbladder cancer: evaluating survival benefit of chemotherapy in early-stage gallbladder cancer. World J Gastrointest Surg. 2025;17(5):103653. doi:10.4240/wjgs.v17.i5.103653
Tables
Table 1. Distribution of incidental pathological findings in cholecystectomy specimens
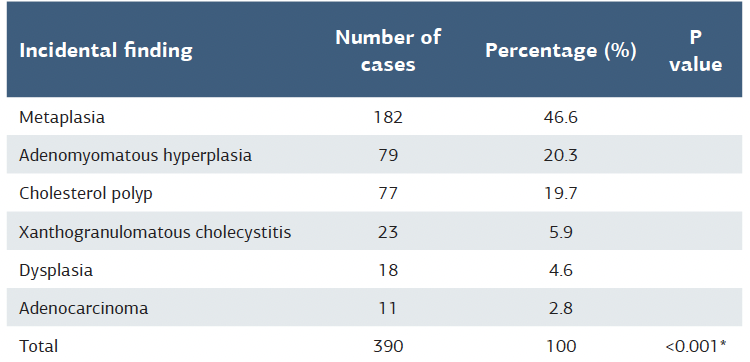
*p-value calculated by Chi-square test (χ² = 321.8, p<0.001).
Table 2. Demographic and pathological characteristics of adenocarcinoma cases
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Osman Gökhan Gökdere, Bahadır Öndeş. Incidental pathological findings in cholecystectomy: a single-center retrospective analysis. Ann Clin Anal Med 2025;16(10):759-762. doi:10.4328/ACAM.22871
- Received:
- August 30, 2025
- Accepted:
- September 29, 2025
- Published Online:
- September 30, 2025
- Printed:
- October 1, 2025