
Abstract
AimThis study aimed to evaluate and compare the accuracy of four intraoral scanners (IOS) in capturing the three-dimensional positions of orthodontic brackets on dental models.MethodsTwenty maxillary dental models bonded with MBT stainless steel brackets were scanned using four IOS systems: Primescan, Trios 4, iTero Element 5D, and Medit i700. A high-accuracy laboratory scanner served as the reference standard. Each model was scanned twice with each IOS, yielding 160 datasets. Scans were aligned to the reference using a two-step superimposition protocol, and bracket slot-center deviations were measured in mesiodistal, occlusogingival, buccolingual, and angular dimensions. Trueness, precision, and clinically acceptable deviation rates were analyzed using ANOVA/Kruskal–Wallis tests and intraclass correlation coefficients (ICC).ResultsPrimescan showed the highest trueness, with linear deviations of 0.05–0.07 mm and angular deviations of 0.58–0.62°. Trios 4 demonstrated similar accuracy, remaining within ±0.10mm and ± 1°. iTero Element 5D exhibited greater variation (0.10–0.12mm; 1.12–1.25°), while Medit i700 showed the highest deviations (0.11–0.13mm; 1.29–1.41°). Clinically acceptable deviation rates were 92.5% for Primescan, 88.1% for Trios 4, 76.4% for iTero, and 62.7% for Medit. Precision analysis showed the lowest repeat-scan variability for Primescan (0.03 ± 0.01 mm), whereas Medit displayed the highest variability. ICC values exceeded 0.90 for all scanners.ConclusionScanner accuracy varied significantly, with Primescan and Trios 4 demonstrating superior trueness and precision. iTero and Medit showed reduced accuracy, particularly in angular measurements. Scanner selection is therefore critical for workflows requiring high-fidelity bracket capture.
Keywords
Introduction
Digital technologies have significantly transformed diagnostic and therapeutic workflows in modern orthodontics. Among these innovations, intraoral scanners (IOS) have become essential tools, allowing clinicians to obtain optical impressions without conventional materials while improving patient comfort and clinical efficiency. IOS systems are now widely used for digital model creation, indirect bonding trays, virtual setup, and treatment monitoring.1 As their clinical use expands, the accuracy of these scanners becomes increasingly important, particularly when capturing small and complex structures such as orthodontic brackets.
Bracket position strongly influences the biomechanics of tooth movement, and even minor errors in height, angulation, or mesiodistal placement may lead to unwanted movements, prolonged treatment, or additional wire adjustments.2 Metallic brackets, however, present scanning challenges due to their reflective surfaces, sharp edges, and geometric complexity.3 Light reflection, surface gloss, and limited edge detection contribute to inaccuracies in three-dimensional (3D) reconstruction.
Although numerous studies have assessed the trueness and precision of IOS systems for full-arch scans or implant impressions,4 fewer have investigated their accuracy in capturing fixed orthodontic appliances. Recent evidence indicates that brackets introduce additional scanning errors and that performance varies according to scanner hardware, imaging algorithms, and post-processing filters.5 Because inaccurate scanning may compromise indirect bonding accuracy, custom archwire fabrication, and digital treatment simulations, understanding these performance differences is clinically relevant.
Despite increasing clinical adoption, comparative evidence on the accuracy of IOS systems specifically for bracket capture remains limited. Most studies evaluate a few scanners or lack detailed bracket-specific metrics. Therefore, a systematic comparison under standardized conditions is needed to guide clinicians in selecting scanners suitable for bracket-based digital workflows.
The aim of this study was to compare the accuracy of different intraoral scanners in capturing the 3D positions of orthodontic brackets on dental models. Using a high-precision laboratory scanner as the reference, we analyzed clinically relevant linear and angular deviations to better understand how scanner selection may influence digital orthodontic procedures.
Materials and Methods
Study DesignThis in-vitro experimental study was conducted to compare the accuracy of different intraoral scanners (IOS) in capturing the three-dimensional positions of orthodontic brackets bonded to standardized dental models. All procedures followed a strictly controlled laboratory workflow to eliminate intraoral variables such as saliva, patient movement, soft-tissue interference, and limited accessibility.Preparation of Dental ModelsA total of 20 maxillary dental arch models (polyurethane, Nissin Dental Products Inc., Kyoto, Japan) were used. These models were selected for their dimensional stability and ability to simulate enamel-like scanning properties. Each model demonstrated standard occlusal morphology with no defects, cracks, or undercuts that might influence scanning behavior.Bracket Bonding ProcedureBracket bonding was standardized across all models to minimize operator-related variability. Each dental model received 0.022-inch MBT prescription stainless steel orthodontic brackets (3M Unitek, Monrovia, CA, USA), bonded by a single experienced operator following a controlled protocol. The bonding surfaces were first lightly roughened with 600-grit abrasive paper to improve micromechanical retention. A thin layer of universal adhesive (Scotchbond Universal) was applied and gently air-thinned, after which each bracket was bonded using light-cured orthodontic composite (Transbond XT). To ensure uniformity in vertical height, mesiodistal positioning, and bracket angulation, a calibrated alignment jig was used during seating. Excess adhesive was carefully removed, and all brackets were polymerized with an LED curing unit for 20 seconds per tooth, ensuring consistent bonding strength and positional accuracy across all models.Reference Scanner and Gold-Standard DatasetA high-accuracy desktop laboratory scanner (E4 Lab Scanner, 3Shape A/S, Copenhagen, Denmark; accuracy ≤ 5 µm) was used to generate the gold-standard reference dataset for all measurements. Each dental model was scanned twice under identical conditions to ensure repeatability. The two datasets were compared within the scanner’s proprietary software, and the scan exhibiting the lower overall surface deviation was selected as the definitive reference model. All finalized reference scans were exported in STL format without any post-processing or smoothing and served as the trueness standard against which all intraoral scanner outputs were evaluated.Intraoral Scanners EvaluatedFour commercially available intraoral scanner (IOS) systems were included in the evaluation: Trios 4 (3Shape), which uses structured light technology; iTero Element 5D (Align Technology), operating on parallel confocal imaging; Medit i700 (Medit Corp.), utilizing structured light projection; and Primescan (Dentsply Sirona), which employs high-frequency active triangulation. Each scanner was operated strictly in accordance with the manufacturer’s recommended scanning protocol to ensure optimal performance and reproducibility. Prior to every scanning session, the devices were calibrated using their respective built-in calibration tools, guaranteeing consistency across all measurements and preventing accuracy drift over time.Scanning ProtocolEach of the 20 dental models was scanned twice with each intraoral scanner, yielding a total of 160 digital scan datasets. To ensure methodological consistency, all scans were performed under strictly standardized environmental conditions, including controlled ambient lighting at 550 lux, a stable workstation temperature of 22 ± 1°C, and a constant scanner-to-model distance and angulation. Before scanning, each model was thoroughly dried using oil-free compressed air to prevent reflection artifacts from moisture. A uniform S-shaped scanning path was employed across all devices, systematically capturing the occlusal, buccal, and palatal surfaces, followed by targeted high-detail passes over the metallic bracket surfaces to enhance data acquisition of reflective areas. All scans were exported in STL format without any post-processing, mesh smoothing, or noise-reduction filters to preserve raw data integrity for subsequent accuracy analysis.3D Alignment and MeasurementAll STL datasets were imported into Geomagic Control X (3D Systems, USA) for three-dimensional evaluation. Each IOS scan was superimposed onto its corresponding reference scan using a two-step alignment protocol. First, an initial three-point landmark alignment was performed to establish a preliminary spatial match. This was followed by global best-fit alignment using the iterative closest point (ICP) algorithm to optimize surface correspondence. To avoid bias introduced by reflective bracket surfaces, the alignment process was restricted exclusively to tooth surfaces, ensuring that superimposition accuracy reflected scanner performance rather than bracket geometry.
Following alignment, each bracket’s slot center was identified in 3D space and used as the reference point for positional assessment. Four principal metrics were extracted for each bracket: mesiodistal deviation, occlusogingival/vertical deviation, buccolingual displacement, and angular discrepancies, including torque (buccolingual inclination) and tip (mesiodistal inclination). All measurements were conducted by a single calibrated examiner and repeated after a two-week interval to assess intra-examiner reliability, ensuring reproducibility of the measurement protocol.Outcome DefinitionsTwo primary outcome variables were used to evaluate scanner performance: trueness and precision. Trueness was defined as the degree to which each IOS scan deviated from the corresponding reference model, reflecting how accurately the scanner captured the actual bracket position. Precision referred to the consistency between repeated scans obtained with the same device, indicating the scanner’s reproducibility under identical conditions. Based on established orthodontic bracket placement standards, deviations within ± 0.10 mm for linear measurements and ± 1° for angular measurements were considered clinically acceptable thresholds, as errors beyond these limits may influence bracket positioning accuracy and subsequent tooth movement.Ethical ApprovalEthical approval was not required as this was an in vitro study conducted on dental models and did not involve human participants, animals, or identifiable data.Statistical AnalysisStatistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). The distribution of all continuous variables was evaluated using the Shapiro–Wilk test to determine the appropriateness of parametric or non- parametric testing. Comparisons of trueness and precision among the four intraoral scanners were conducted using one-way ANOVA for normally distributed data or the Kruskal– Wallis test for non-normally distributed data. When significant differences were identified, Tukey’s HSD or Dunn’s post hoc tests were applied for pairwise comparisons, depending on the underlying data distribution. Intraclass correlation coefficients (ICC) were calculated to assess intra-examiner reliability, with values greater than 0.90 interpreted as excellent reproducibility. A P value < .05 was considered statistically significant for all analyses, and effect sizes along with 95% confidence intervals were reported to provide additional context regarding the magnitude and precision of observed differences.Reporting GuidelinesNo specific reporting guideline was applicable to this in vitro experimental study.
Results
A total of 160 digital scans were obtained from 20 bracketed dental models using the four intraoral scanners. All scans were successfully completed without technical errors, and no dataset required exclusion. The reference scanner produced high- resolution surface meshes that served as the trueness standard for all comparisons.
Linear trueness analysis demonstrated distinct differences in bracket-position accuracy among the four intraoral scanners, as summarized in Table 1 and shown in Figure 1. Primescan showed the highest overall trueness, with mean mesiodistal, occlusogingival, and buccolingual deviations of 0.06 ± 0.02 mm, 0.07 ± 0.03 mm, and 0.05 ± 0.02 mm, respectively. Trios 4 performed similarly well, with corresponding deviations of 0.07 ± 0.03 mm, 0.08 ± 0.03 mm, and 0.06 ± 0.03 mm, remaining consistently within the ± 0.10 mm clinical threshold. In contrast, iTero Element 5D demonstrated larger deviations—0.10 ± 0.05 mm, 0.12 ± 0.06 mm, and 0.11 ± 0.05 mm—while Medit i700 exhibited the highest linear errors, reaching 0.11–0.13 mm across all three axes. Statistical analyses confirmed significant differences among scanners (P < .001 for all parameters) (Table 1, Figure 1).
Angular deviation analysis revealed clear performance differences among the scanners, consistent with the values presented in Table 2. Primescan demonstrated the smallest angular discrepancies, with mean torque and tip deviations of 0.58±0.24° and 0.62±0.21°, respectively, both well within the clinically acceptable ± 1° threshold. Trios 4 showed slightly higher but still clinically reliable angular values, with torque deviations of 0.71 ± 0.28° and tip deviations of 0.75 ± 0.31°. In contrast, iTero Element 5D showed larger angular discrepancies, with torque deviations reaching 1.12 ± 0.48 ° and tip deviations of 1.25 ± 0.52°, often exceeding clinical tolerance. Medit i700 exhibited the greatest angular inaccuracy, with torque and tip deviations of 1.29 ± 0.55° and 1.41 ± 0.58°, respectively (Table 2). Precision analyses revealed notable differences in intra-scanner repeatability across the four systems. Primescan demonstrated the highest repeatability, with mean repeat- scan deviations of 0.03 ± 0.01 mm for linear measurements and 0.28 ± 0.14° for angular parameters. Trios 4 followed closely, showing repeatability values of 0.04 ± 0.02 mm and 0.32 ± 0.15°, respectively. iTero Element 5D exhibited moderate repeatability, with linear deviations of 0.07 ± 0.03 mm and angular deviations of 0.49 ± 0.22°, whereas Medit i700 showed the greatest variability, with corresponding values of 0.08 ± 0.04 mm and 0.53 ± 0.25°. Despite these differences, all scanners demonstrated excellent intra-examiner reliability, with intraclass correlation coefficients (ICCs) exceeding 0.90 (Primescan: 0.96; Trios 4: 0.95; iTero: 0.92; Medit: 0.90) (Table 3).
Clinically acceptable deviation rates were calculated using thresholds of ± 0.10 mm for linear measurements and ± 1° for angular measurements. Primescan demonstrated the highest overall compliance, with 92.5% of all measurements falling within acceptable limits, followed closely by Trios 4 at 88.1%. iTero Element 5D showed satisfactory performance in linear parameters, with 76.4% of mesiodistal, occlusogingival, and buccolingual deviations meeting clinical criteria; however, its angular precision was notably lower, with only 58.3% of torque and tip values remaining within the ± 1° threshold. Medit i700 exhibited the lowest clinical acceptability, with an overall rate of 62.7%, and demonstrated the highest proportion of deviations exceeding both linear and angular limits. These discrepancies were particularly pronounced in posterior regions, where bracket reflectivity and scanning access appeared to compound measurement error, as presented in Figure 2.
Discussion
The present in-vitro study evaluated and compared the trueness and precision of four commonly used intraoral scanners— Primescan, Trios 4, iTero Element 5D, and Medit i700—in capturing the three-dimensional position of orthodontic brackets. The findings demonstrate clear performance differences among systems, particularly in their ability to reproduce small, reflective, and geometrically complex bracket surfaces. Primescan and Trios 4 consistently exhibited superior linear and angular accuracy, whereas iTero Element 5D and Medit i700 showed greater deviations, especially in angular measurements.
The high accuracy observed for Primescan and Trios 4 aligns with previous studies reporting their strong performance in full-arch scans and implant-level trueness evaluations.4,6 Active triangulation (Primescan) and structured-light projection (Trios) appear better suited to capturing small metallic surfaces, likely due to improved light-control algorithms and higher image-capture frequencies. This supports earlier reports suggesting that scanner hardware configuration—including light source, frame rate, and reconstruction algorithms—plays a critical role in data quality.7-8
In contrast, the larger linear and angular deviations observed for iTero Element 5D and Medit i700 are consistent with prior research indicating that confocal imaging and certain structured-light systems may be more susceptible to noise when scanning reflective orthodontic appliances.9 Metallic brackets have been shown to pose unique challenges due to specular reflection and loss of edge fidelity, which may compromise mesh reconstruction accuracy.3 Our findings further reinforce this limitation: iTero and Medit exhibited the largest errors in torque and tip measurements, which are particularly sensitive to surface detail loss and pixel-level misregistration.
From a clinical standpoint, these results carry meaningful implications. Angular bracket deviations beyond ± 1° may lead to unintended tooth movements and require additional wire adjustments or repositioning.10-11 While Primescan and Trios 4 maintained angular deviations within acceptable limits, the frequent exceedance of this threshold by iTero Element 5D and Medit i700 suggests that these systems may be less suitable for workflows demanding high-precision bracket capture, such as digital indirect bonding or robotic archwire fabrication.
Precision analysis further showed that repeatability varied across scanners, with Primescan demonstrating the lowest intra-scanner variability. This aligns with evidence showing that scanners with higher frame acquisition rates and adaptive stitching algorithms yield more stable datasets.12 Although all ICC values exceeded 0.90, indicating excellent examiner reliability, the higher variability observed with iTero and Medit suggests greater sensitivity to operator movement and scanning angle, which may influence clinical reproducibility.
Another noteworthy finding is the scanner-dependent variation in clinically acceptable deviation rates. Primescan and Trios 4 achieved over 85% compliance with clinical thresholds, while iTero Element 5D and Medit i700 fell below 80% and 65%, respectively. The reduced acceptability in the posterior region, particularly for Medit, is consistent with previous studies demonstrating reduced accuracy in areas with limited accessibility and increased reflection from metallic components.13
Limitations
This study was conducted under controlled in-vitro conditions, which do not fully replicate the complexity of the oral environment. Only one bracket type and four intraoral scanners were evaluated, limiting generalizability across different materials and devices. Measurements were performed by a single examiner, and although reliability was high, multi- operator variability was not assessed. Additionally, only slot-center positional and angular deviations were analyzed; other clinically relevant parameters were not included.
Conclusion
In conclusion, this in-vitro study demonstrated that the accuracy of orthodontic bracket capture varies substantially among different intraoral scanners. Primescan and Trios 4 exhibited the highest levels of trueness and precision, maintaining linear deviations within ± 0.10 mm and angular deviations within ± 1°, thereby meeting clinically acceptable thresholds for most measurements. In contrast, iTero Element 5D and Medit i700 showed significantly larger linear and angular discrepancies, particularly in torque and tip measurements, and a lower proportion of clinically acceptable deviations. These findings highlight that scanner selection plays a critical role in digital orthodontic workflows—especially in contexts requiring high- fidelity bracket reproduction, such as indirect bonding, digital setups, or robotically bent archwires. While all scanners tested are suitable for general intraoral scanning, clinicians aiming for maximal accuracy in bracket-specific applications may benefit from using systems with superior trueness and repeatability. Future clinical studies incorporating diverse bracket materials, varied scanning conditions, and larger operator pools are warranted to validate and expand upon these results.
Declarations
Author Contributions (CRediT Taxonomy)
Conceptualization: A.F.K., O.D.O.
Methodology: A.F.K., O.D.O.
Investigation: A.F.K.
Data Curation: A.F.K.
Formal Analysis: A.F.K., O.D.O.
Writing – Original Draft: A.F.K.
Writing – Review & Editing: O.D.O.
Supervision: O.D.O.
Abbreviations
3D: Three-dimensional
ANOVA: Analysis of variance
ICC: Intraclass correlation coefficient
ICP: Iterative closest point
IOS: Intraoral scanner
LED: Light-emitting diode
MBT: McLaughlin, Bennett, and Trevisi
STL: Standard tessellation language
References
- Mangano FG, Veronesi G, Hauschild U, Mijiritsky E, Mangano C. Trueness and precision of four intraoral scanners in oral implantology: a comparative in vitro study. Plos One. 2016;11(9):e0163107. doi:10.1371/journal.pone.0163107
- Palone M, Fazio M, Pellitteri F, et al. CAD/CAM-based 3D-printed and PVS indirect bonding jig system accuracy: a systematic review, meta-analysis, and comparative analysis of hard and soft CAD/CAM transfer trays. Eur J Orthod. 2024;46(1):cjad069. doi:10.1093/ejo/cjad069
- Angelone F, Ponsiglione AM, Ricciardi C, Cesarelli G, Sansone M, Amato F. Diagnostic applications of intraoral scanners: a systematic review. J Imaging. 2023;9(7):134. doi:10.3390/jimaging9070134
- Mangano FG, Hauschild U, Veronesi G, Imburgia M, Mangano C, Admakin O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: a comparative in vitro study. BMC Oral Health. 2019;19(1):101. doi:10.1186/s12903-019-0792-7
- Zhu F, Yu L, Hu M, et al. Influence of 3D printing angles on the accuracy of indirect adhesion transfer models: an in vitro study. Sci Rep. 2025;15(1):9012-9018. doi:10.1038/s41598-025-90328-1
- Eggmann F, Blatz MB. Recent advances in intraoral scanners. J Dent Res. 2024;103(13):1349-1357. doi:10.1177/00220345241271937
- Keul C, Güth J-F. Accuracy of full-arch digital impressions: an in vitro and in vivo comparison. Clin Oral Investig. 2019;24(2):735-745.
- Ortensi L, La Rosa GRM, Ciletta S, Grande F, Pedullà E. Evaluation of the accuracy of digital impressions with different scanning strategies: an in vitro study. J Dent. 2024;151:105433. doi:10.1016/j.jdent.2024.105433
- Palone M, Bellavia M, Floris M, et al. Evaluation of effects of brackets and orthodontic wires on intraoral scans: a prospective in‐vivo study. Orthod Craniofac Res. 2023;27(1):44-54.
- Fafat KKK, Jain D, Pandit SK, Kharbanda R, Trivedy P, Gupta E. Three dimensional evaluation of accuracy of bracket positioning. J Pharm Bioallied Sci. 2023;15(Suppl 2):S1188-1191. doi:10.4103/jpbs.jpbs_167_23
- Schlenz MA, Klaus K, Schmidt A, et al. The transfer accuracy of digital and conventional full-arch impressions influenced by fixed orthodontic appliances: a reference aid–based in vitro study. Clin Oral Investig. 2022;27(1):273-283. doi:10.1007/s00784-022-04721-5
- Falih MY, Majeed MA. Trueness and precision of eight intraoral scanners with different finishing line designs: a comparative in vitro study. Eur J Dent. 2022;17(4):1056-1064.
- Grande F, Mosca Balma A, Mussano F, Catapano S. Effect of implant scan body type, intraoral scanner and scan strategy on the accuracy and scanning time of a maxillary complete arch implant scans: an in vitro study. J Dent. 2025;159:105782. doi:10.1016/j.jdent.2025.105782
Tables
Table 1. Trueness of linear bracket position measurements for the four intraoral scanners
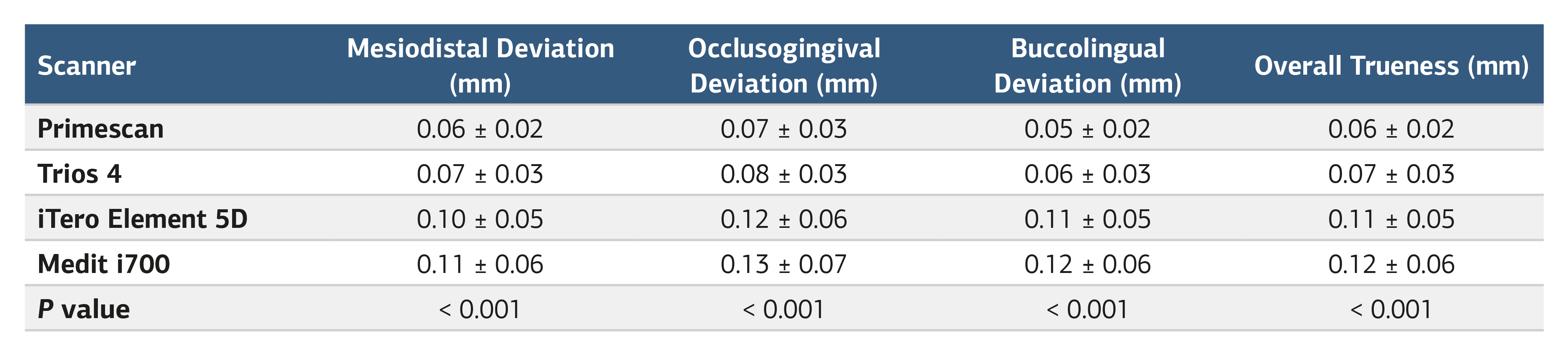
Values represent mean ± standard deviation; deviations relative to reference scanner
Table 2. Angular deviations of orthodontic brackets measured by the four intraoral scanners
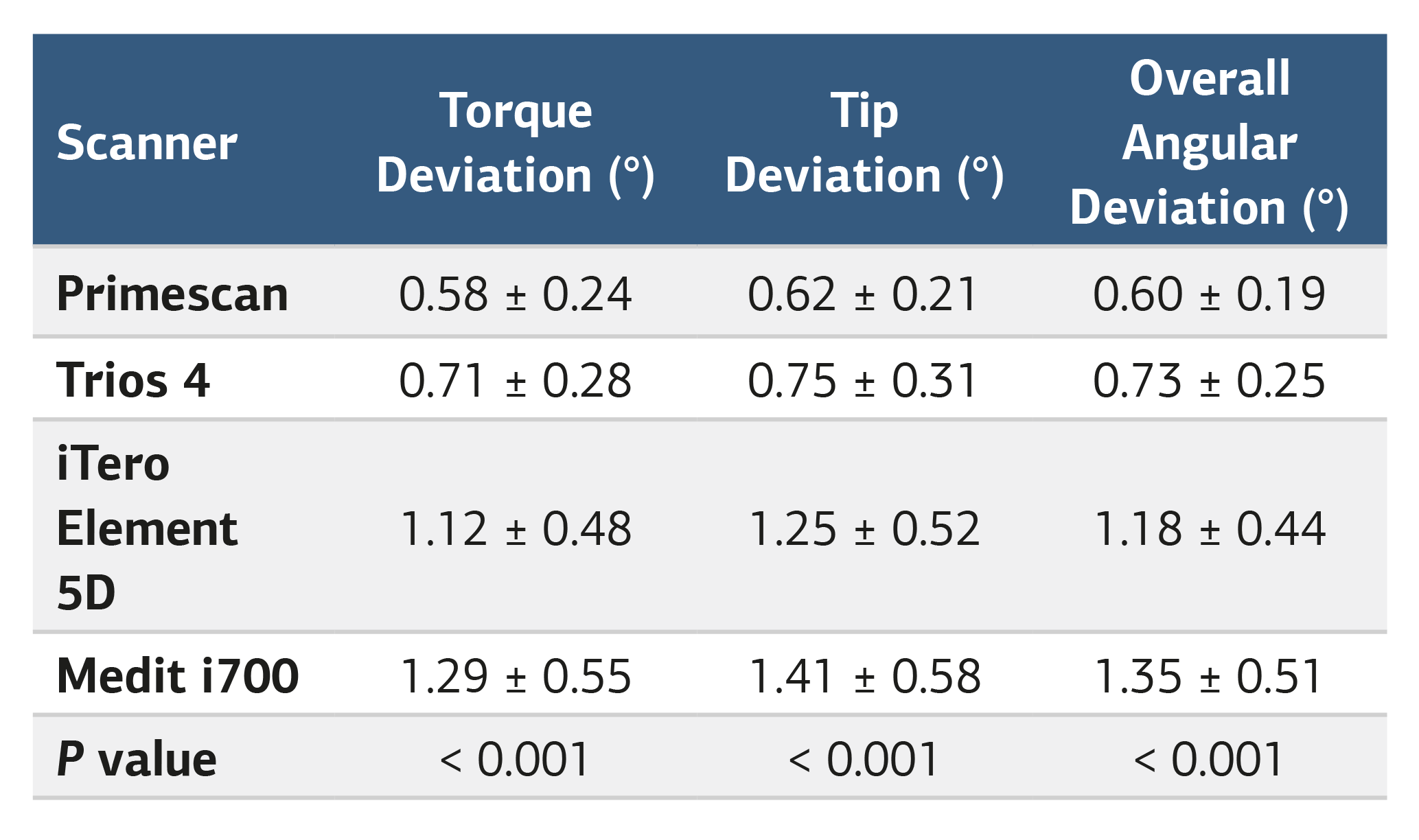
Table 3. Precision and intra-scanner repeatability for the four intraoral scanners
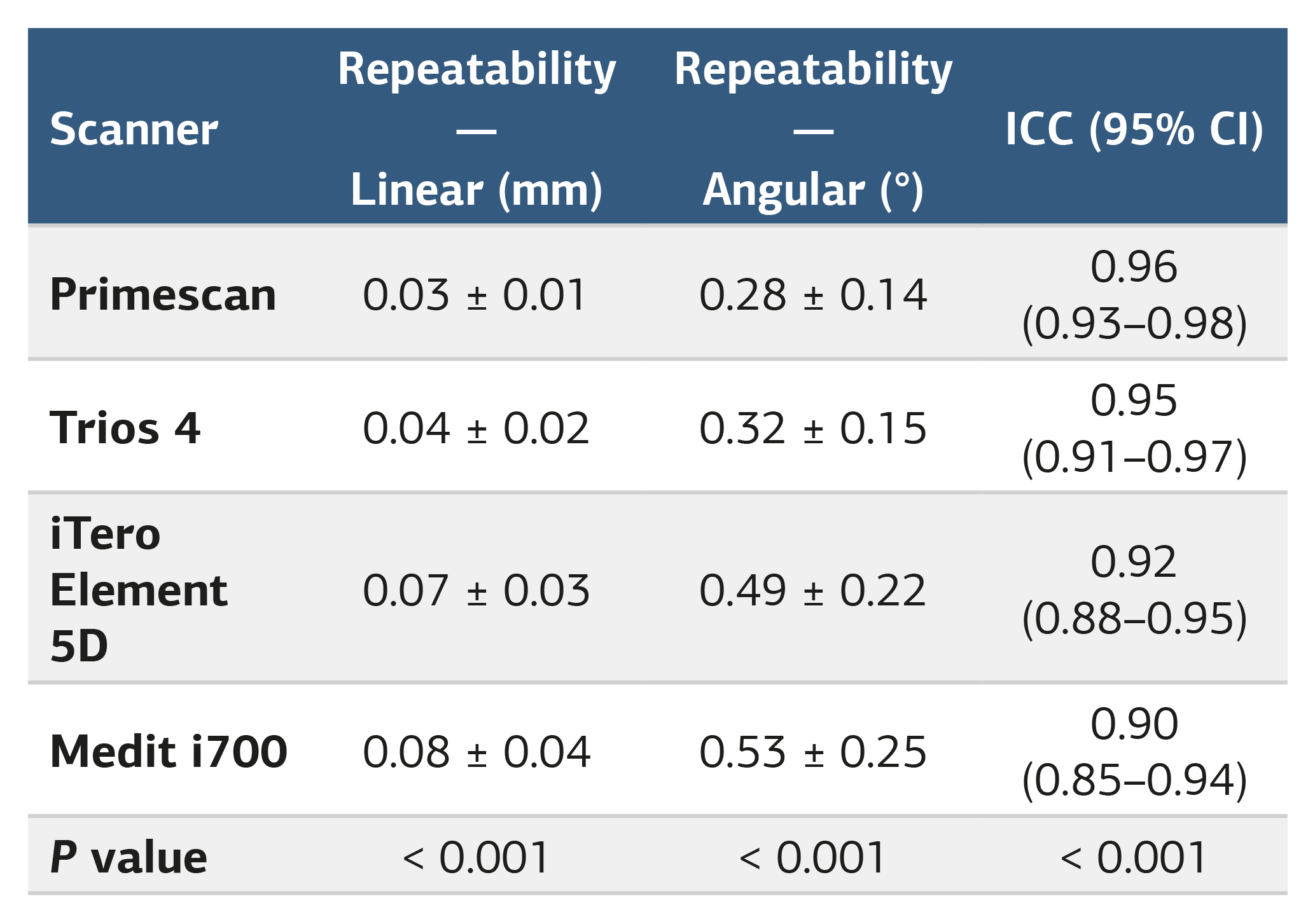
Intra-class correlation coefficient (ICC) and repeat scan deviation
Figures
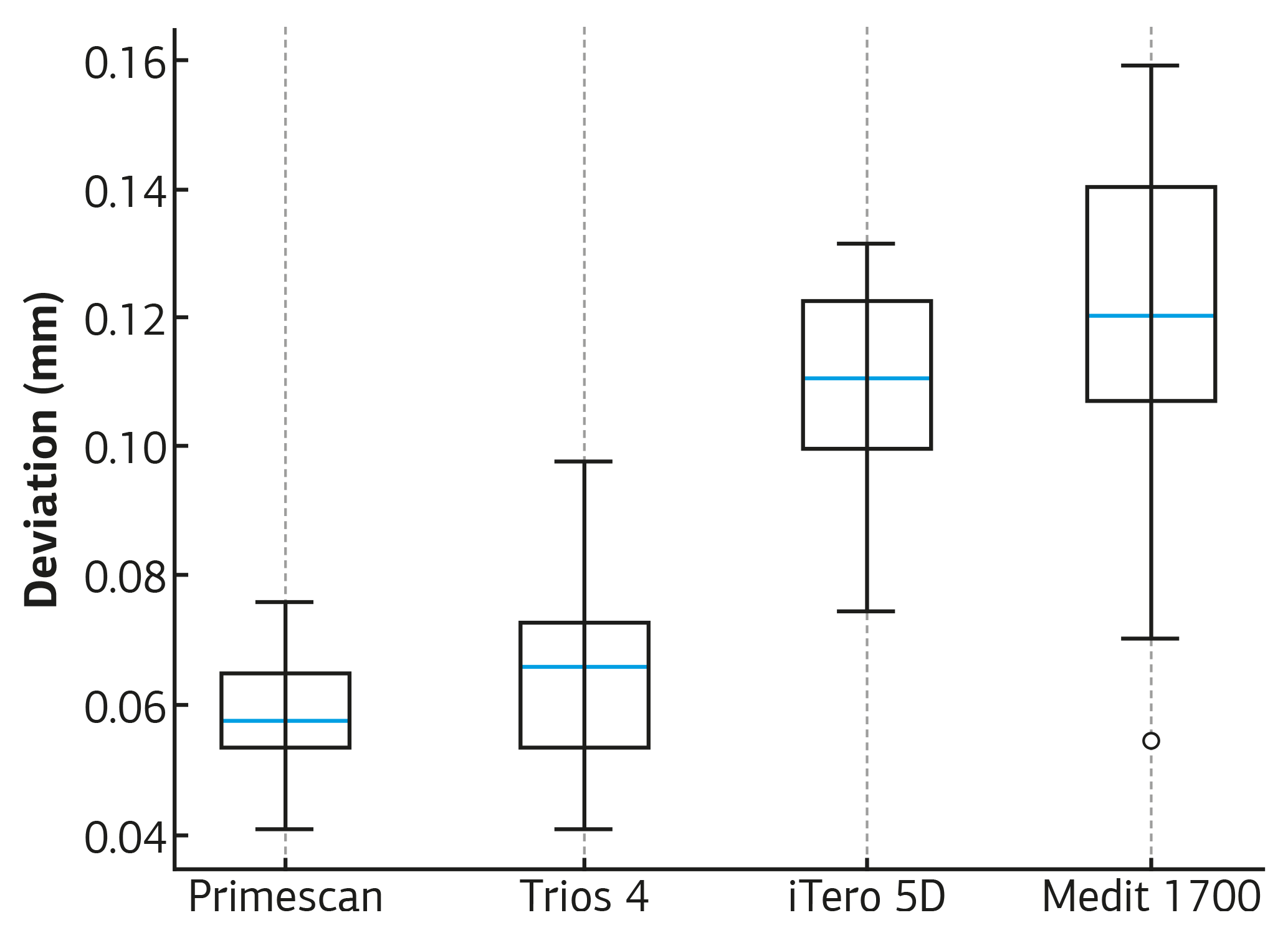
Figure 1. Distribution of linear deviations (Mesiodistal) across scanners
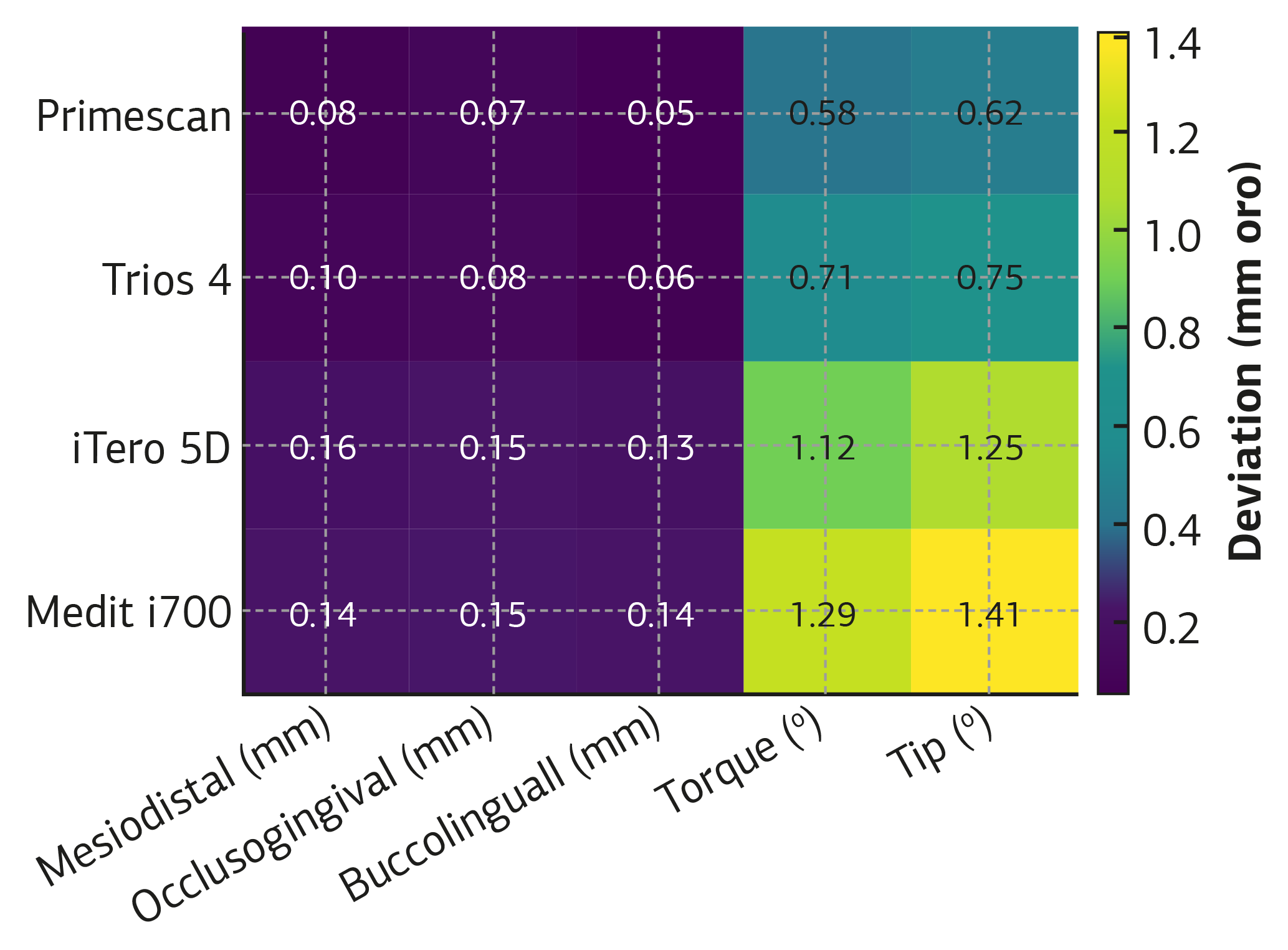
Figure 2. Heatmap of mean linear and angular deviations for each scanner
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ali Furkan Karakoyunlu, Ozum Dasdemir Ozkan. Accuracy comparison of different intraoral scanners in capturing orthodontic bracket positions: an in vitro evaluation. doi:10.4328/ACAM.22994
Publication History
- Received:
- 17.11.2025
- Accepted:
- 05.01.2026
- Published Online:
- 13.01.2026
- Printed:
- 01.08.2026