
Perinatal outcomes of preterm premature rupture of membranes (PPROM) and vaginal culture results
Effect of vaginal culture results on PPROM
Authors
Abstract
Aim This study aimed to investigate the vaginal culture results and maternal and fetal outcomes in pregnancies with premature rupture of membranes.
Methods Between May 2022 and February 2024, the vaginal culture results, as well as obstetric, demographic, laboratory, and neonatal outcomes, of pregnant women diagnosed with preterm premature rupture of membranes who gave birth at a Tertiary Hospital were analyzed.
Results In our study, 82 patients who met the criteria were included. Of these patients, 54 (65.8%) had a positive culture result, while 28 (34.2%) had a negative culture result. The most common finding in the positive culture group was the growth of Lactobacillus (33, 40.2%). It was observed that among those with a positive vaginal culture result, 51.9% were admitted to the neonatal intensive care unit, while 57.1% of those with a negative culture result were admitted to the neonatal intensive care unit.
Conclusion Vaginal infections involved in the etiology of preterm premature rupture of membranes affect maternal and fetal outcomes. In pregnancies with PPROM, the ascending progression of vaginal infection can lead to adverse outcomes, including neonatal intensive care unit admission and possibly death. Early diagnosis and treatment protocols should aim to prevent this situation.
Keywords
Introduction
Prelabor rupture of membranes (PROM) is defined as the rupture of fetal membranes before the onset of uterine contractions. When this occurs before the 37th week of gestation, it is referred to as preterm prelabor rupture of membranes (PPROM). Approximately 3% of pregnancies under 37 weeks are complicated by PPROM. According to gestational age, about 0.5% of PROM cases occur before 27 weeks, 1% between 27 and 34 weeks, and 1% between 34 and 37 weeks.1,2,3 The exact pathogenesis of spontaneous membrane rupture is not fully understood. The strength and integrity of fetal membranes are derived from extracellular membrane proteins, including collagens, fibronectin, and laminin, while matrix metalloproteinases (MMPs) increase collagen degradation, thus reducing membrane strength.4
Risk factors for PPROM include genital tract infections, a history of PPROM, antepartum bleeding, smoking, polyhydramnios, and trauma.
PPROM pregnancies may lead to fetomaternal complications such as chorioamnionitis and placental abruption. Guidelines have been developed to reduce the development of complications and improve fetomaternal outcomes.
In our study, the vaginal culture results and neonatal outcomes in pregnancies with PPROM were analyzed.
Materials and Methods
Our study is a retrospective observational study. It includes pregnant women diagnosed with preterm premature rupture of membranes (PPROM) who were admitted to a tertiary center between May 2022 and February 2024, as well as those who gave birth at the same hospital. The study was conducted by reviewing maternal and fetal data (such as hemoglobin, platelet count, mode of delivery, maternal chronic diseases, gestational age at first hospital admission, gestational age at delivery, perinatal ultrasound, BMI, birth weight, neonatal intensive care unit admission, etc.) recorded in the hospital’s laboratory and clinical follow-up information. The sample size was calculated using the sample size formula. The event frequency was assumed to be 3%, the margin of error was set at 5%, and the sampling error was 0.05, which resulted in a minimum sample size of 45.
The diagnosis of membrane rupture was based on the criteria of cervical examination showing fluid accumulation, a gush of fluid, and positive diagnostic test results.
Exclusion criteria were:
• Pregnant women who were not admitted for treatment at the hospital
• Pregnant women who were not admitted for delivery at the Hospital
For vaginal culture, aerobic and anaerobic microbiota were Gram-stained and cultured.
Ethical ApprovalThis study was approved by the Ethics Committee of the University of Hamidiye, Faculty of Health Science (Date: 14.03.2024, Decision No: 24/210).
Statistical AnalysisThe IBM SPSS 27 package program was used to analyze the data in the study. Continuous data are presented as mean ± standard deviation, and categorical data are presented as frequency and percentage. In comparing differences between categorical variables according to groups, the Pearson chi-square test was used for 2 x 2 and R x C tables where the proportion of cells with the expected value number of 5 or above or below 5 did not exceed 20%. The Fisher Freeman Halton test was used for R x C tables where the proportion of cells with the expected value number of less than 5 exceeded 20%. Statistical significance was accepted as p<0.05 for all analyses.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
In the search conducted for our study, 82 patients who met the inclusion criteria were identified. The gestational age ranged from the earliest at 22 weeks to the latest at 36 weeks, with an average gestational age of 30.5 weeks (Table 1).
Among these patients, 54 had a positive vaginal culture result. Of the 54 patients, 33 (61.1%) had the growth of lactobacillus (Table 2).
All patients with PPROM in our study received corticosteroid treatment. For antibiotic therapy, ampicillin-sulbactam was prophylactically administered to the PPROM patients. Four patients who did not receive antibiotics were identified, and only one patient was started on meropenem (Table 3).
Vaginal cultures were obtained from all PPROM patients. Of the 54 patients with a positive culture, 28 (51.9%) of the newborns were admitted to the neonatal intensive care unit (NICU). Among the 28 patients with negative culture results, 16 (57.1%) of the newborns were admitted to the NICU.
A total of 45 newborns from PPROM pregnancies were admitted to the NICU. The reasons for NICU admission, in order of frequency, were prematurity (29), neonatal jaundice (6), and transient tachypnea of the newborn (TTN) (4) (Table 4).
The average BMI of PPROM patients was found to be 26.69. The mean hemoglobin level was 11.13, the mean white blood cell (WBC) count was 11.27, and the average CRP value before prophylaxis was 11.16.
Although 13 patients had a history of cesarean section, 55 patients delivered via cesarean section in this study. The primary cesarean section rate was 42 / 69 (60.8%). The most common indication for cesarean section was fetal distress (16 cases).
The average gravida was 2.8, the average parity was 1.3, and the average number of abortions was 0.5. All patients diagnosed with PPROM received antibiotic prophylaxis, with only one patient not receiving treatment.
Complications associated with pregnancy were observed in 23 (28%) of the patients, with the most common being gestational diabetes mellitus (GDM) (5 cases). Among the 82 patients with PPROM, 56 (68.3%) had perinatology follow-up, and the most frequent finding after routine monitoring was anhydramnios, observed in 3 (3.7%) cases.
Discussion
In our study, we believe that the follow-up and treatment of pregnancies with PPROM reduced maternal and fetal complications. Out of 21,714 births in these 22 months, 82 pregnancies with PPROM gave birth at our hospital, resulting in a PPROM prevalence rate of 0.3%. This rate is closer to that seen in early PPROM cases in the literature. It is believed that this result is due to the fact that the patients did not give birth at the same hospital and needed to be transferred because there was no neonatal intensive care unit available at the hospital.
A five-year prospective study in which 189 cases of PPROM were identified, yielding a prevalence of 2.8%. The average gestational age was found to be 35.6 weeks. The cesarean section rate was 29.1%, and the gestational diabetes mellitus (GDM) rate was 1.83 (1.14–2.94).5
In a study of pregnancies with PPROM at gestational ages greater than 28 weeks, the cesarean section rate was found to be 22.05%. The most common vaginal culture result was the growth of normal flora, observed in 23.4% of cases.6
In a study on early PPROM (before 24 weeks), the cesarean section rate was 46.2%, while in later PPROM, the cesarean section rate was 36.3%.7
A study conducted on 300 patients with PPROM found an average age of 27 years and an average gestational age of 32.2 weeks (28-36 ± 3).8
In a multi-center study of 160 PPROM patients, the average gestational age was found to be 31.8 weeks. Among 133 live births, 79 (59%) were admitted to the neonatal intensive care unit (NICU), with the most common reasons for admission being early neonatal sepsis (n = 55, 41%) and respiratory distress syndrome (RDS) (n = 40, 30%).9
In a similar study of 190 PPROM pregnancies, the cesarean section rate was observed to be 29.5% (56 cases). Respiratory stress was found in 24.7% (47 cases).10
In another study, the prevalence of PPROM was found to be 4.2% among 94 cases.11
A large-scale study involving 424 cases of PPROM found a prevalence of 13.67%. This prevalence is significantly higher than what is reported in the literature. In this study, the average age was 29.76 years.12
In a similar study of 387 patients, 19 cases of PPROM were observed, with a prevalence of 4.91%.13
A study of 99 singleton pregnancies with PPROM found an incidence of 3.7%, with an average gestational age of 30.1 weeks and a cesarean section rate of 26.8%.14
In a study involving 150 PPROM patients and 150 controls, the most common bacterial growth in vaginal cultures from the PPROM group was Staphylococcus aureus (28%, 42 cases).15
In another study of 101 PPROM patients, the most common microorganism identified in vaginal cultures was Escherichia coli (28.7%, 29 cases).16
In conclusion, PPROM is a serious condition that affects both the mother and the fetus. Complications can worsen the clinical situation. Our responsibility lies in ensuring that the diagnostic and treatment process is conducted in the most appropriate manner. Prophylactic antibiotics, culture tests, and adequate hospital resources can help minimize complications.
Our study aims to contribute to the improvement of healthcare service quality and provide guidance in managing PPROM cases.
Limitations
The limitations of the study are that pregnant women diagnosed with PPROM went to different centers, refused treatment, and had insufficient culture swabs.
Conclusion
Our study and the comparison with the literature also showed that cesarean section rates were high. This was thought to be due to concerns about healthcare services not being legally protected.
Similarly, there is variability in vaginal culture results in the literature. This was thought to result from differences in sociocultural levels.
Prematurity is the leading cause of admission to neonatal intensive care units. It is desirable for every pregnancy to reach term and for every baby to be born healthy.
Declarations
Ethics Declarations
Ethical approval for this study was obtained from the University of Hamidiye, Faculty of Health Sciences Ethics Committee (Approval date: 2024-03-14; Approval number: 24/210).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived due to the retrospective nature of the study and the use of anonymized patient data
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.M., E.T.
Methodology: A.M., N.G.K.
Investigation: A.M., O.G., Ü.E.
Data curation: E.T., N.G.K.
Formal analysis: E.T.
Writing – original draft: A.M., E.T.
Writing – review & editing: N.G.K., O.G., Ü.E.
Supervision: A.M.
Abbreviations
BMI: body mass index;
CNS: coagulase-negative staphylococci;
CRP: C-reactive protein;
ESBL: extended-spectrum beta-lactamase;
GDM: gestational diabetes mellitus;
MMPs: matrix metalloproteinases;
NICU: neonatal intensive care unit;
PPROM: preterm prelabor rupture of membranes;
PROM: prelabor rupture of membranes;
RDS: respiratory distress syndrome;
TTN: transient tachypnea of the newborn;
WBC: white blood cell.
References
-
Mercer BM. Preterm premature rupture of the membranes: current approaches to evaluation and management. Obstet Gynecol Clin North Am. 2005;32(3):411-428. doi:10.1016/j.ogc.2005.03.003
-
van der Heyden JL. Preterm prelabor rupture of membranes: different gestational ages, different problems. Dissertation. Maastricht University; 2014:190. doi:10.26481/dis.20140327jh
-
Smith GN, Rafuse C, Anand N, et al. Prevalence, management, and outcomes of preterm prelabour rupture of the membranes of women in Canada. J Obstet Gynaecol Can. 2005;27(6):547-553. doi:10.1016/S1701-2163(16)30711-3
-
Birkedal-Hansen H. Proteolytic remodeling of extracellular matrix. Curr Opin Cell Biol. 1995;7(5):728-735. doi:10.1016/0955-0674(95)80116-2
-
Bouvier D, Forest JC, Blanchon L, et al. Risk factors and outcomes of preterm premature rupture of membranes in a cohort of 6968 pregnant women prospectively recruited. J Clin Med. 2019;8(11):1987. doi:10.3390/jcm8111987
-
Shivaraju P, Purra P, Bheemagani N, Lingegowda K. Vaginal infections and its relation to preterm labour, PPROM, PROM and its outcome. Int J Reprod Contracept Obstet Gynecol. 2015;4(5):1422-1426. doi:10.18203/2320-1770.ijrcog20150723
-
Manuck TA, Varner MW. Neonatal and early childhood outcomes following early vs later preterm premature rupture of membranes. Am J Obstet Gynecol. 2014;211(3):308.e1-308.e6. doi:10.1016/j.ajog.2014.05.030
-
Abouseif H, Mansour A, Hassan S, Sabbour S. Prevalence and outcome of preterm premature rupture of membranes (PPROM) among pregnant women attending Ain Shams maternity hospital. Egypt J Community Med. 2018;36(2):99-107. doi:10.21608/ejcm.2018.11055
-
Abebe TA, Nima DD, Mariye YF, Leminie AA. Determinants for perinatal adverse outcomes among pregnant women with preterm premature rupture of membrane: a prospective cohort study. Front Reprod Health. 2022;4:1052827. doi:10.3389/frph.2022.1052827
-
Rajan R, Menon V. Preterm premature rupture of membranes: correlates and pregnancy outcome in a tertiary care setting. Int J Res Med Sci. 2016;4(8):3310-3316. doi:10.18203/2320-6012.ijrms20162285
-
O TC, Enwereji J, Okoro O, Adiri C, Ezugwu E, Agu P. The incidence and management outcome of preterm premature rupture of membranes (PPROM) in a tertiary hospital in Nigeria. Am J Clin Med Res. 2014;2(1):14-17. doi:10.12691/ajcmr-2-1-4
-
Addisu D, Melkie A, Biru S. Prevalence of preterm premature rupture of membrane and its associated factors among pregnant women admitted in Debre Tabor General Hospital, North West Ethiopia: institutional-based cross-sectional study. Obstet Gynecol Int. 2020;2020:4034680. doi:10.1155/2020/4034680
-
Pisoh DW, Mbia CH, Takang WA, et al. Prevalence, risk factors and outcome of preterm premature rupture of membranes at the Bamenda Regional Hospital. Open J Obstet Gynecol. 2021;11(3):233-251. doi:10.4236/ojog.2021.113023
-
Mercer BM, Crocker LG, Pierce WF, Sibai BM. Clinical characteristics and outcome of twin gestation complicated by preterm premature rupture of the membranes. Am J Obstet Gynecol. 1993;168(5):1467-1473. doi:10.1016/S0002-9378(11)90783-2
-
Karat C, Madhivanan P, Krupp K, et al. The clinical and microbiological correlates of premature rupture of membranes. Indian J Med Microbiol. 2006;24(4):283-285. doi:10.4103/0255-0857.29388
-
Abdel-Hakeem AK, Shawky HE-D, Mohamed AM, Mohamed KG, Elbadawy AA. Prevalence of microorganisms associated with preterm premature rupture of membranes in Minia University Hospital: prospective study. Minia J Med Res. 2024;35(1):80-85.
Tables
Table 1. Demographic findings (PPROM: Preterm Prelabor Rupture of Membranes)
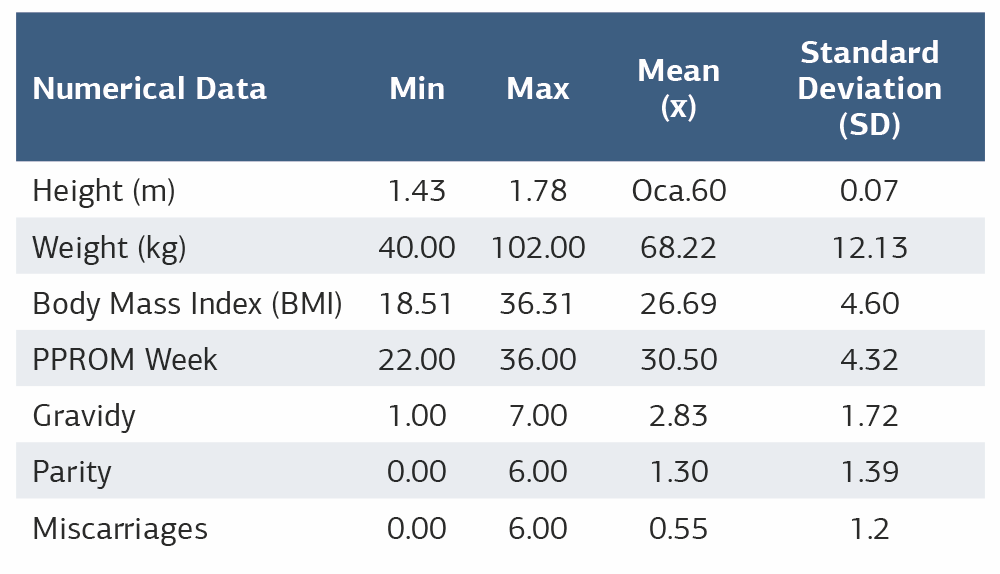
Table 2. Vaginal culture results
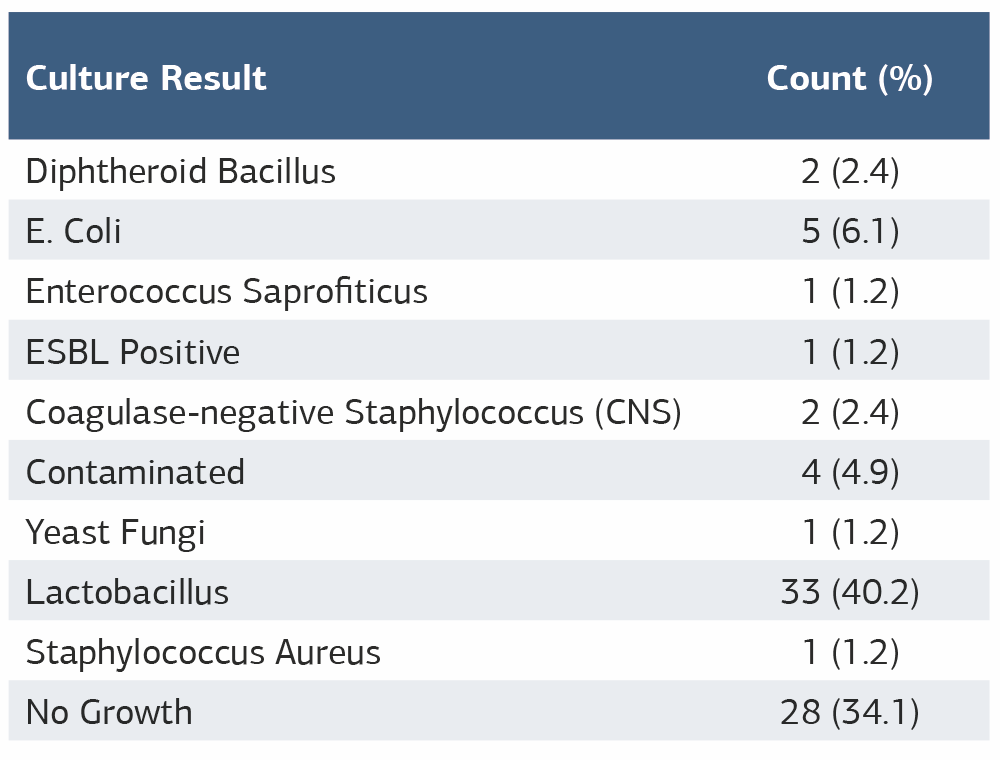
Table 3. Newborn complications
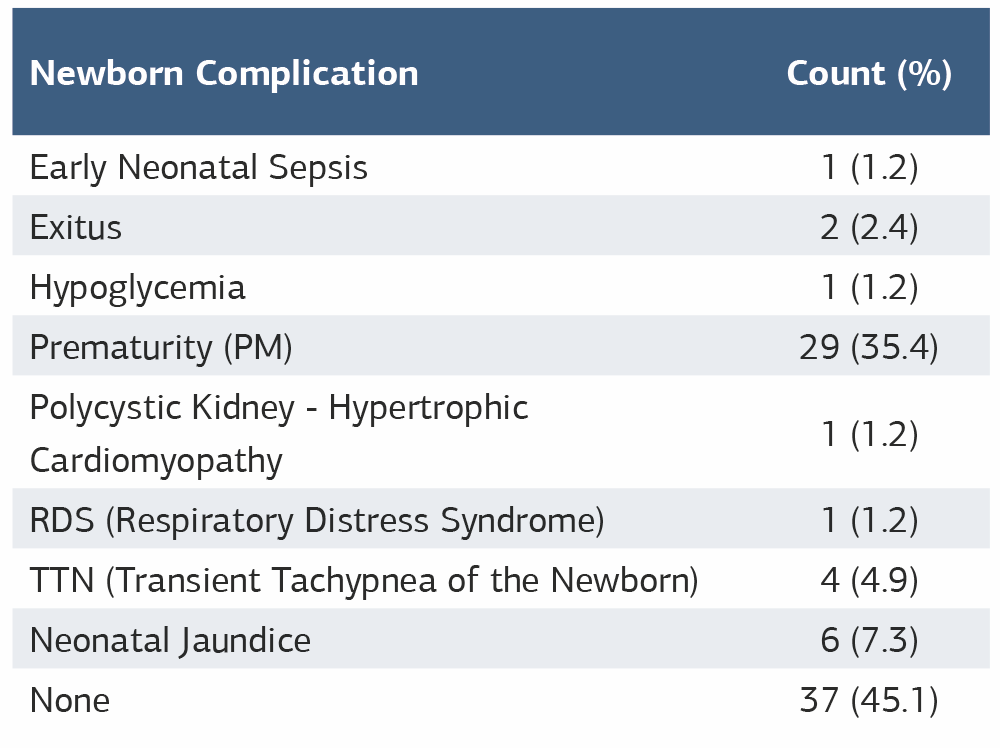
Table 4. Effect of vaginal culture results on neonatal outcomes
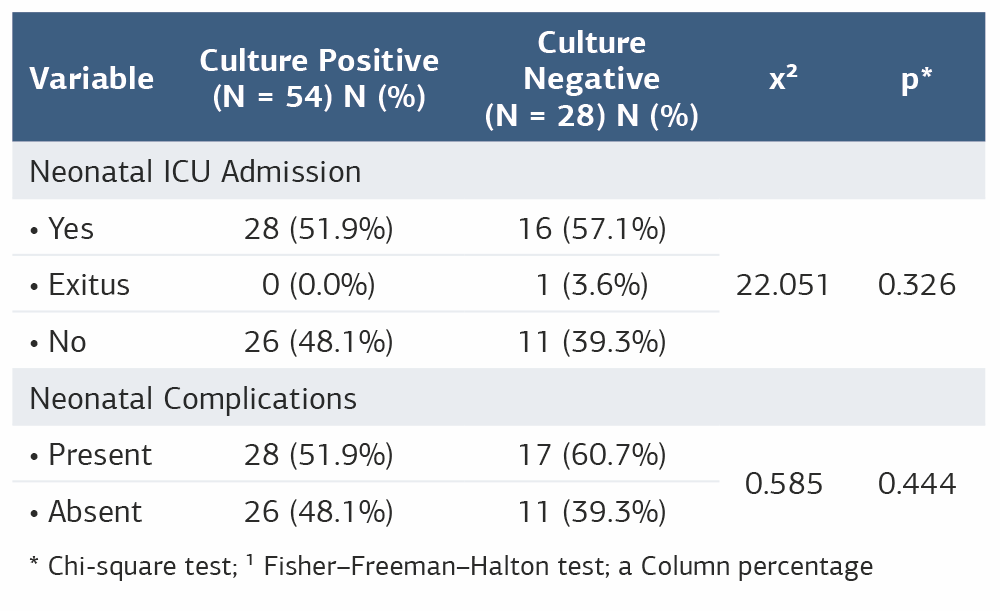
* Chi-square test; ¹ Fisher–Freeman–Halton test; a Column percentage
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Abdurrahman Mert, Erzat Toprak, Nur Gözde Kulhan, Oğuzhan Günenc, Ümmügülsüm Esenkaya. Perinatal outcomes of preterm premature rupture of membranes (PPROM) and vaginal culture results. Ann Clin Anal Med 2026;17(3):219-222. doi:10.4328/ACAM.23007
- Received:
- November 27, 2025
- Accepted:
- January 12, 2026
- Published Online:
- January 20, 2026
- Printed:
- March 1, 2026