
Morbidity, mortality, and ICU stay after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
CRS-HIPEC: morbidity, mortality, and ICU stay
Authors
Abstract
AimCytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) is a comprehensive treatment approach for primary peritoneal cancers and peritoneal metastases from colorectal, appendiceal, ovarian, gastric, and other malignancies. This study aimed to evaluate clinical outcomes, perioperative complications, and their impact on morbidity and mortality in patients undergoing CRS and HIPEC.
MethodsA retrospective analysis was conducted on patients who underwent CRS and HIPEC. Demographic characteristics, primary diagnoses, comorbidities, laboratory findings, surgical details, and chemotherapeutic agents were recorded. Perioperative hemodynamic changes, fluid and blood product use, need for postoperative intensive care and mechanical ventilation, and renal injury were assessed. ICU stay duration and mortality rates were documented.
ResultsA total of 41 patients were included. The most common primary diagnosis was ovarian cancer (65.9%), followed by colon cancer (17.1%) and mesothelioma (14.6%). Chemotherapeutic agents administered included cisplatin (78%), paclitaxel (46.3%), doxorubicin (14.6%), oxaliplatin (14.6%), and 5-FU (12.2%). Most patients (87.8%) were extubated postoperatively, and 90.2% required ICU follow-up. The mean ICU stay was 4.3 ± 1.5 days. Acute kidney injury occurred in 21.9% of patients. One-month postoperative mortality was 12.2%, and total mortality at 15 months was 24.4%.
ConclusionCRS and HIPEC are associated with significant perioperative physiological changes. Successful outcomes require meticulous perioperative management, particularly in terms of hemodynamic stability and organ function support.
Keywords
Introduction
Peritoneal carcinomatosis is an aggressive pattern of invasion that is associated with high-grade malignancies and has a low cure rate with standard systemic chemotherapies. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) are a comprehensive treatment option for both primary peritoneal cancers and peritoneal surface malignancies with secondary peritoneal metastases of colorectal, appendix, ovarian, gastric, and other malignancies. Cytoreductive surgery is the surgical removal of visible tumors from the intra-abdominal area, including peritoneal surfaces and abdominopelvic organs. It can range from omentectomy alone to more extensive abdominal resection, including removal of the gastrointestinal tract, pancreas, spleen, gallbladder, uterus, ovaries, part of the liver, and lymph nodes larger than 2.5 mm.1 This technique has been shown to increase the duration and quality of life of patients with peritoneal carcinomatosis originating from different cancers, such as colorectal, gastric, ovarian, and peritoneal mesothelioma. This procedure is followed by HIPEC, which involves administering highly concentrated chemotherapy agents (cisplatin, mitomycin) heated to 41°C-43°C into the peritoneal cavity.2 In the 6th workshop on peritoneal surface cancers held in 2008, it was recommended that CRS and HIPEC techniques be used in experienced centers as a routine treatment method in the management of peritoneal carcinomatosis. The factors that increase mortality and morbidity rates are prolonged surgical time; major intravascular and extravascular volume loss and protein loss, which affect body thermoregulation; and chemotherapeutic agents such as cisplatin used during HIPEC, which may cause acute kidney injury. The morbidity rates of the HIPEC procedure range from 12% to 67.6%, and mortality rates range from 0% to 9%.3 Due to the physiological and metabolic changes during the administration of this multimodal therapy, the perioperative period should be managed carefully, considering the high risk of complications. Although there are many studies related to CRS+HIPEC in the literature, comprehensive data on perioperative hemodynamic management, renal function, and the need for postoperative intensive care are still limited.
The primary aim of this study was to analyze the clinical outcomes of patients undergoing CRS+HIPEC, detail the complications encountered during the perioperative period, and assess their effect on morbidity and mortality.
Materials and Methods
After obtaining ethical approval, the medical records of 41 patients who underwent CRS+HIPEC between 01.01.2018 and 30.09.2020 were retrospectively analyzed. Patient data were recorded by analyzing anesthesia consultation forms, anesthesia observation forms, and epicrisis documents in the electronic system. In the preoperative period, demographic data (age, height, weight, gender, body mass index (BMI)), American Society of Anaesthesiologists (ASA) scores, comorbidities, preoperative laboratory values, and primary diagnosis were recorded from the patient files. Intraoperative procedures, duration of surgery (CRS+HIPEC), blood and blood product replacement needs, use of vasopressors and inotropes, type and amount of fluids administered, and chemotherapeutic agents used in the HIPEC phase were recorded. In the postoperative period, extubation rate, intensive care requirement, length of stay in the intensive care unit (ICU), mortality, use of vasopressors and inotropes in the ICU, need for invasive mechanical ventilation (re-intubation status), need for non-invasive mechanical ventilation, blood and blood product replacement, and laboratory values at the 24th postoperative hour were recorded. Acute Kidney Injury Network (AKIN) criteria were used to assess acute kidney injury.4
Primary and Secondary OutcomesThe primary outcomes of this study were morbidity rates (perioperative complications, including acute kidney injury, hemodynamic instability, respiratory complications, and need for re-intubation), mortality rates (early [1-month] and overall follow-up mortality), and duration of postoperative intensive care unit (ICU) stay. Secondary outcomes included postoperative intensive care requirements (need for ICU admission, use of vasopressors and inotropes, invasive and non-invasive mechanical ventilation), perioperative hemodynamic changes (hypotension, large fluid shifts, blood product transfusion, electrolyte imbalances), renal outcomes (acute kidney injury assessed according to the AKIN criteria and requirement for dialysis), respiratory outcomes (postoperative extubation in the operating room and re-intubation rates), as well as surgical and chemotherapeutic parameters (duration of CRS+HIPEC procedure, type of chemotherapeutic agents administered, perioperative bleeding, and extent of organ resections).
Ethical ApprovalThis study was approved by the Ethics Committee of Firat University (Date: 01.10.2020, Decision No: 2020/13-15).
Statistical AnalysisThe analyses were performed using SPSS (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL) 22 package program. Descriptive data were presented as n, % values for categorical data and mean ± standard deviation values for continuous data. Chi-square analysis (Pearson Chi-square) was used to compare categorical variables between groups. The suitability of continuous variables for normal distribution was evaluated by the Kolmogorov-Smirnov Test. An Independent Samples t-test was used to compare variables that were normally distributed between two groups. A paired-samples t-test was used to compare the measured data from dependent groups. The statistical significance level was accepted as p<0.05 in the analyses.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
A total of 41 patients, 34 (82.9%) females and 7 (17.1%) males, were included in the study. The mean age of the patients was 57.4 ± 10.9 years, and the mean BMI was 25.6 ± 4.5 kg/m2. When the patients' ASA scores were evaluated, 4 (9.8%) were ASA 2, 36 (87.8%) were ASA 3, and 1 (2.4%) was ASA 4. Comorbidities were observed in 27 (65.9%) patients; 12 (29.3%) had cardiovascular system comorbidity, 8 (19.5%) had diabetes mellitus, 3 (7.3%) had respiratory system comorbidity, and 22 (53.7%) had other comorbidities (Table 1).
During HIPEC, 32 (78%) patients received cisplatin, 19 (46.3%) paclitaxel, 6 (14.6%) doxorubicin, 6 (14.6%) oxaliplatin, and 5 (12.2%) 5-FU. The mean duration of the CRS+HIPEC procedure was 308.5 ± 101 min. The primary diagnoses consisted of ovarian cancer in 27 (65.9%), colon cancer in 7 (17.1%), mesothelioma in 6 (14.6%), and pelvic mass in 1 (2.4%) patient. In the intraoperative period, 13 (31.7%) patients received erythrocyte suspension (ES), 20 (48.8%) fresh frozen plasma (FFP), 19 (46.3%) vasopressors + inotropes, and 26 (63.4%) human albumin (HA). Postoperatively, of patients in the ICU, 21 (51.2%) received ES, 18 (43.9%) received TDP, and 12 (29.3%) received HA replacement (Table 2).
Thirty-six (87.8%) of the patients were extubated. Of the patients, 37 (90.2%) were followed in the postoperative ICU, and the mean length of hospital stay was 4.3 ± 1.5 days. Vasopressors and inotropes were used in 8 patients (19.5%) in the ICU. Two (4.9%) of the patients followed up in the ICU were reintubated and received invasive mechanical ventilation, and non-invasive mechanical ventilation was provided to 3 patients (7.3%) (Table 3).
Postoperative acute kidney injury developed in 9 patients (21.9%), and according to the AKIN criteria, analysis revealed that 4 patients (44.4%) were Stage I, 2 patients (22.2%) were Stage II, and 3 patients (33.3%) were Stage III. Two patients at stage III received haemodialysis on postoperative day 2, and one patient at stage I received haemodiafiltration on postoperative day 7. Five patients (12.2%) died within 1 month postoperatively. In the postoperative 15-month period, a total of 10 patients (24.4%) died.
Discussion
Although cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) has been shown to improve survival in patients with peritoneal carcinomatosis, morbidity and mortality rates remain high, ranging between 12–67.6% and 0–9%, respectively.3 Previous studies have reported perioperative mortality between 0–12% and morbidity between 12–56%.5 These findings highlight the need for a multidisciplinary approach in managing this complex patient population.
Our study demonstrated that the requirement for postoperative intensive care is considerable, and effective management of complications is essential. Despite advances in surgical techniques, anesthetic management, and accumulated surgical experience, patients frequently experience significant hemodynamic, hematological, metabolic, and respiratory alterations. Intraoperative challenges such as large fluid shifts, electrolyte imbalances, hypotension, coagulopathy, and hemodynamic instability directly influence postoperative outcomes and may contribute to the high morbidity and mortality associated with CRS+HIPEC. Therefore, appropriate patient selection and complete cytoreduction remain critical for improving clinical outcomes. Reported risk factors for morbidity include patient age, disease burden, surgical extent, number of resected organs, duration of surgery, and perioperative blood loss.6
Despite its increasing use, there is still no consensus on anesthetic management. Comprehensive preoperative evaluation, including a detailed systemic examination with attention to chemotherapeutic agents used intraoperatively, is essential. Comorbidities must be carefully assessed, and adequate preparation undertaken. Anticipation of intraoperative blood loss and coagulation disturbances necessitates central venous access and availability of appropriate blood products. During CRS+HIPEC, patients are prone to substantial intravascular and extravascular fluid and protein losses. The main challenges in this period are hypovolemia, hypothermia due to prolonged surgical time, and coagulopathy from massive bleeding. Prior to the HIPEC phase, normovolemia should be established with balanced solutions and blood products, while avoiding both hypovolemia and fluid overload, which may damage the endothelial glycocalyx.7 Preserving renal function with optimal volume replacement is crucial, though acute renal failure (ARF) often has multifactorial origins, including hypovolemia, hypotension, nephrotoxic drugs, cisplatin use, and systemic inflammation.8 In our study, inadequate intraoperative fluid replacement and nephrotoxic chemotherapy were associated with ARF development. ARF occurred in 21.9% of patients, with one-third classified as Stage III requiring dialysis, underscoring the importance of careful hemodynamic monitoring and perioperative fluid management. Our findings regarding the multifactorial origins of acute renal failure are consistent with the recent meta-analysis by Chen et al., which demonstrated that advanced age, higher BMI, reduced preoperative renal function, hypertension, and diabetes were significant preoperative risk factors for AKI after CRS+HIPEC. Furthermore, intraoperative factors such as cisplatin-based perfusion and hypotension (systolic blood pressure <100 mmHg) were strongly associated with postoperative AKI, while mitomycin C appeared protective.9 These results support our observation that inadequate intraoperative fluid replacement and nephrotoxic agents contribute substantially to renal complications, underlining the necessity of vigilant hemodynamic monitoring, tailored chemotherapeutic regimens, and individualized perioperative fluid management strategies. Previous studies have identified risk factors for ARF, such as advanced age, high BMI, hypertension, and prior chemotherapy.10,11 Similarly, we observed that postoperative intensive care duration and mechanical ventilation requirements were closely related to preoperative patient characteristics, including high ASA scores.12 Consistent with Kaplan et al.,13 our findings indicate that elderly patients with higher ASA scores and comorbidities are more likely to require ICU admission. Functional decline with age, decreased stress tolerance, and comorbidity burden further increase complication risk.14,15 Moreover, obesity was significantly associated with higher ICU requirements in our study, aligning with the literature that identifies obesity as a risk factor for cardiovascular and metabolic comorbidities.16
Chemotherapeutic agents also contribute to perioperative complications. In patients receiving oxaliplatin with 5% dextrose as a carrier solution, postoperative hyperglycemia and hyponatremia were observed, consistent with reports that dilutional hyponatremia increases morbidity and mortality by causing cerebral edema.16 Cisplatin-induced hypomagnesemia may trigger intraoperative arrhythmias;17 in our series, one patient developed an intraoperative arrhythmia requiring medical management.
Surgical factors, including large peritoneal surface resections and multiorgan involvement, also impact postoperative outcomes through fluid and electrolyte imbalances. However, in our study, there was no significant difference in 1-month mortality across surgical types. While previous studies linked bowel resections to increased morbidity in advanced ovarian cancer,18 we observed no significant variation in short- term mortality by diagnosis. Our mean survival time for ovarian cancer patients was 44 months, with 6- and 12-month survival rates of 70.4%, consistent with published reports of median survival ranging between 22–64 months and improved outcomes with complete cytoreduction.19
The mean surgical duration in our series was 308.5 ± 101.0 minutes, with no significant correlation to 1-month mortality. However, patients requiring vasopressors and inotropes in the ICU had a higher 1-month mortality (37.5%), suggesting that perioperative hypotension and hemodynamic instability significantly increase postoperative risk. Blood transfusion, while sometimes unavoidable, was also associated with poorer outcomes, reinforcing the importance of early bleeding control and coagulopathy management.20
Regarding postoperative respiratory outcomes, we achieved a higher-than-reported extubation rate in the operating room (87.8% vs 42–62%).21 Nonetheless, 4.9% required reintubation, which was strongly associated with increased morbidity and mortality, consistent with existing evidence.22 This highlights the importance of early but safe extubation strategies.
Finally, the mean ICU stay in our cohort was 4.3 ± 1.5 days, similar to previous reports,23 and not significantly associated with 1-month mortality.
Limitations
This study has certain limitations. Its retrospective design, relatively small number of patients, and lack of calculation of the cytoreduction score, an important parameter for surgical prognosis, are among the limitations.
Conclusion
CRS+HIPEC is a difficult surgical procedure to manage with high morbidity and mortality. Our study shows that optimal patient selection, intraoperative fluid management, and postoperative intensive care processes should be managed carefully. To reduce the risk of ARF, intraoperative fluid management strategies should be developed, patients requiring postoperative respiratory support should be determined early, and mechanical ventilation management should be optimized. Our study emphasizes the importance of a multidisciplinary approach in CRS+HIPEC applications. In the future, large- scale studies will provide guidance for the development of perioperative management strategies.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: R.P., A.Y.A.
Methodology: R.P., A.Y.A., G.A.
Investigation: R.P., A.Y.A., G.A., S.Ö., F.Ç., O.D.
Data Curation: R.P., G.A., S.Ö.
Formal Analysis: R.P., A.Y.A.
Writing – Original Draft: R.P.
Writing – Review & Editing: A.Y.A., G.A., S.Ö., F.Ç., O.D.
Supervision: A.Y.A.
AI Usage Disclosure
No artificial intelligence tools were used in the preparation of this manuscript.
Abbreviations
AKIN: Acute Kidney Injury Network
ASA: American Society of Anaesthesiologists
BMI: Body mass index
CRS: Cytoreductive surgery
HIPEC: Hyperthermic intraperitoneal chemotherapy
ICU: Intensive care unit
References
-
van de Vaart PJ, van der Vange N, Zoetmulder FA, et al. Intraperitoneal cisplatin with regional hyperthermia in advanced ovarian cancer: pharmacokinetics and cisplatin-DNA adduct formation in patients and ovarian cancer cell lines. Eur J Cancer. 1998;34(1):148-154. doi:10.1016/s0959-8049(97)00370-5
-
Sugarbaker PH. Peritonectomy procedures. Ann Surg. 1995;221(1):29-42. doi:10.1097/00000658-199501000-00004
-
Elias D, Honoré C, Ciuchendéa R, et al. Peritoneal pseudomyxoma: results of a systematic policy of complete cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Br J Surg. 2008;95(9):1164-1171. doi:10.1002/bjs.6235
-
Helderman RFCPA, Löke DR, Kok HP, et al. Variation in clinical application of hyperthermic intraperitoneal chemotherapy: a review. Cancers (Basel). 2019;11(1):78. doi:10.3390/cancers11010078
-
Canda AE, Sokmen S, Terzi C, et al. Complications and toxicities after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2013;20(4):1082-1087. doi:10.1245/s10434-012-2853-x
-
Kusamura S, Younan R, Baratti D, et al. Cytoreductive surgery followed by intraperitoneal hyperthermic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer. 2006;106(5):1144-1453. doi:10.1002/cncr.21708
-
Rehm M, Zahler S, Lötsch M, et al. Endothelial glycocalyx as an additional barrier determining extravasation of 6% hydroxyethyl starch or 5% albumin solutions in the coronary vascular bed. Anesthesiology. 2004;100(5):1211-1223. doi:10.1097/00000542-200405000-00025
-
Chappell D, Jacob M, Hofmann-Kiefer K, Conzen P, Rehm M. A rational approach to perioperative fluid management. Anesthesiology. 2008;109(4):723-740. doi:10.1097/aln.0b013e3181863117
-
Chen D, Ma Y, Li J, et al. Risk factors for postoperative acute kidney injury after cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy: a meta-analysis and systematic review. World J Surg Oncol. 2025;23(1):40. doi:10.1186/s12957-025-03657-w
-
Solanki SL, Mukherjee S, Agarwal V, et al. Society of Onco-Anaesthesia and Perioperative Care consensus guidelines for perioperative management of patients for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC). Indian J Anaesth. 2019;63(12):972-987. doi:10.4103/ija.ija_765_19
-
Bakrin N, Bereder JM, Decullier E, et al. Peritoneal carcinomatosis treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for advanced ovarian carcinoma: a French multicentre retrospective cohort study of 566 patients. Eur J Surg Oncol. 2013;39(12):1435-1443. doi:10.1016/j.ejso.2013.09.030
-
Rodgers A, Walker N, Schug S, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321(7275):1493. doi:10.1136/bmj.321.7275.1493
-
Kaplan C, Araz C, Candan S, et al. Evre III-IV over kanseri nedeniyle sitoredüktif cerrahi geçiren hastalarda postoperatif yoğun bakım gereksiniminin ön belirleyicileri [Predictors of intensive care unit admission following cytoreductive surgery for stage III-IV ovarian carcinoma]. Turk J Intensive Care. 2012;8(3):102-109. doi:10.4274/tybdd.205
-
Brooks SE, Ahn J, Mullins CD, Baquet CR. Resources and use of the intensive care unit in patients who undergo surgery for ovarian carcinoma. Cancer. 2002;95(7):1457-1462. doi:10.1002/cncr.10872
-
Margulies DR, Lekawa ME, Bjerke HS, Hiatt JR, Shabot MM. Surgical intensive care in the nonagenarian: no basis for age discrimination. Arch Surg. 1993;128(7):753-756. doi:10.1001/archsurg.1993.01420190043006
-
Berchtold P, Jörgens V, Finke C, Berger M. Epidemiology of obesity and hypertension. Int J Obes. 1982;5(suppl 1):1-7.
-
Rueth NM, Murray SE, Huddleston SJ, et al. Severe electrolyte disturbances after hyperthermic intraperitoneal chemotherapy: oxaliplatin versus mitomycin C. Ann Surg Oncol. 2011;18(1):174-180. doi:10.1245/s10434-010-1210-1
-
Cheatham ML, White MW, Sagraves SG, Johnson JL, Block EF. Abdominal perfusion pressure: a superior parameter in the assessment of intra-abdominal hypertension. J Trauma. 2000;49(4):621-626. doi:10.1097/00005373-200010000-00008
-
Leath CA 3rd, Kendrick JE 4th, Numnum TM, et al. Outcomes of gynecologic oncology patients admitted to the intensive care unit following surgery: a university teaching hospital experience. Int J Gynecol Cancer. 2006;16(5):1766-1769. doi:10.1111/j.1525-1438.2006.00702.x
-
Deraco M, Baratti D, Laterza B, et al. Advanced cytoreduction as surgical standard of care and hyperthermic intraperitoneal chemotherapy as promising treatment in epithelial ovarian cancer. Eur J Surg Oncol. 2011;37(1):4-9. doi:10.1016/j.ejso.2010.11.004
-
Dixon E, Datta I, Sutherland FR, Vauthey JN. Blood loss in surgical oncology: neglected quality indicator? J Surg Oncol. 2009;99(8):508-512. doi:10.1002/jso.21187
-
Acheampong D, Guerrier S, Lavarias V, et al. Unplanned postoperative reintubation following general and vascular surgical procedures: outcomes and risk factors. Ann Med Surg (Lond). 2018;33:40-43. doi:10.1016/j.amsu.2018.08.013
-
Kamal JM, Elshaikh SM, Nabil D, Mohamad MA. The perioperative course and anesthetic challenge for cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Egypt J Anaesth. 2013;29:311-318. doi:10.1016/j.egja.2013.05.005
Tables
Table 1. Demographic characteristics and comorbidities of CRS+HIPEC patients

*Patients with more than one comorbidity. CVS: cardiovascular system, DM: diabetes mellitus, CRS: cytoreductive surgery, HIPEC: hyperthermic intraperitoneal chemotherapy.
Table 2. Primary diagnoses of CRS+HIPEC patients and the distribution of blood product replacements in their ICU stay
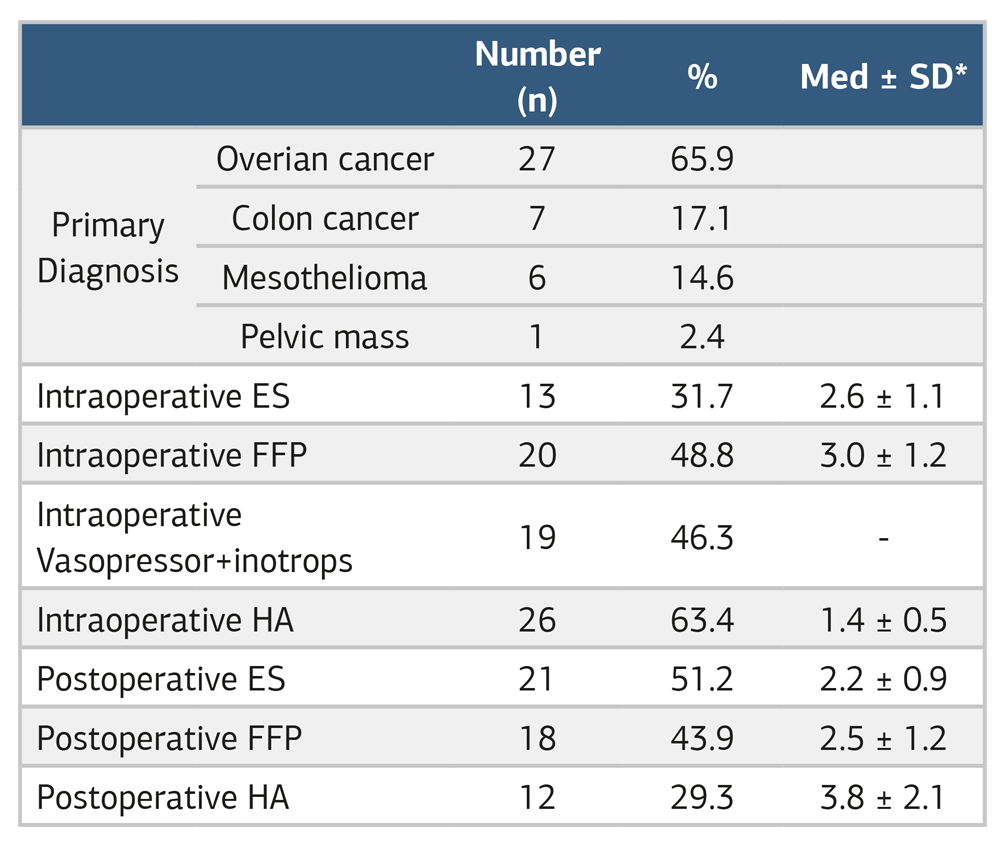
*Med ± SD (Median ± Standart Deviation): Mean of ES, FFP, and colloid used intraoperatively.
Table 3. Characteristics of CRS+HIPEC patients admitted to the postoperative ICU
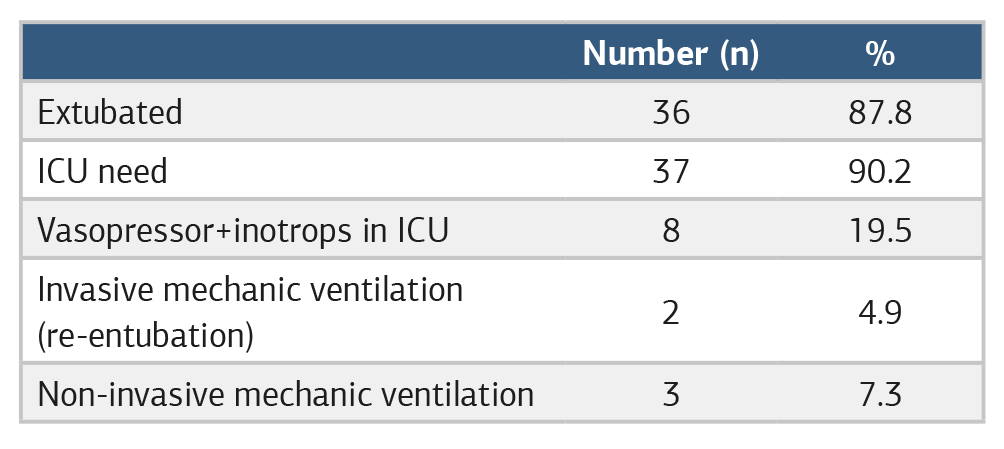
CRS: cytoreductive surgery, HIPEC: hyperthermic intraperitoneal chemotherapy, ICU: intensive care unit.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Rüstem Payam, Aysun Yıldız Altun, Gülsüm Altuntaş, Sibel Özcan, Fatma Çelik, Oğuzhan Demirel. Morbidity, mortality, and ICU stay after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Clin Anal Med 2026;17(7):724-728. doi:10.4328/ACAM.22819
- Received:
- July 21, 2025
- Accepted:
- September 29, 2025
- Published Online:
- December 22, 2025
- Printed:
- July 1, 2026