
The impact of gestational diabetes in Saudi Arabia: epidemiology, risk factors, and management strategies
The impact of gestational diabetes
Authors
Abstract
Gestational diabetes mellitus (GDM) is a major public health concern worldwide, and its prevalence has been steadily increasing in Saudi Arabia. This review aims to provide a comprehensive overview of the epidemiology, risk factors, and management strategies associated with GDM in Saudi Arabia.
Epidemiologically, the incidence of GDM in Saudi Arabia is rising, with estimates ranging from 10% to 30% of pregnancies, reflecting a shift toward urbanization, lifestyle changes, and increasing rates of obesity and diabetes.
Lifestyle modifications, including dietary adjustments and physical activity, are recommended as first-line interventions. In more severe cases, pharmacological treatments such as insulin therapy or oral hypoglycemic (antihyperglycemic )agents may be necessary.
This review emphasizes the importance of promoting early detection and implementing preventive strategies to curb the rising incidence. Enhanced healthcare infrastructure, maternal education, and government policies are vital in improving outcomes for women and children affected by GDM in Saudi Arabia.
Keywords
Gestational diabetes mellitus (GDM) is defined as any degree of glucose intolerance that is first identified during pregnancy. GDM is among the most common complications of pregnancy, and its prevalence increases with increasing rates of obesity and older maternal age worldwide.1,2
Moreover, the GDM ‘continuum’ may increase the risk of pregnancy complications, such as preeclampsia, stillbirth, birth injury, preterm birth, large size for gestational age, and newborn hypoglycemia. Outside of the pregnancy spectrum, mothers may be at increased risk of type 2 diabetes, and their offspring may be at increased risk of obesity, type 2 diabetes (T2DM), and other metabolic disorders. The prevalence of GDM globally varies between 1% and 30% and several researchers around the world correlate with the prevalence of increasing obesity, sedentary lifestyle, and T2DM.1,2,3
According to the Saudi Medical Journal 2020, “The prevalence of GDM in Saudi Arabia is high compared to other countries.4 In a cohort study in Riyadh’s capital of 9723 women recruited between 2013 and 2015, 24.2% had GDM.5 GDM can impose various burdens on both the mother and the healthcare system and some key aspects of the burden associated with GDM include stillbirth, preterm birth, and large for gestational age babies.6
Despite the high prevalence, limited data are available in Saudi Arabia that describe gestational diabetes and its impact on the health of mothers and offspring. Thus, this review aims to provide a comprehensive overview of the epidemiology, risk factors, and management strategies associated with GDM in Saudi Arabia.
Definition and Diagnostic CriteriaGestational diabetes mellitus (GDM) is an important global health issue, and it is crucial to conduct screening for GDM in early pregnancy to decrease the risk of pregnancy complications.4,7 Gestational diabetes mellitus is defined as any carbohydrate intolerance with varying severity first recognition during pregnancy, excluding long-standing cases of type 1 diabetes and type 2 diabetes.8
Two potential methods are used in current diagnostic methods for GDM, which are illustrated in Figure 1. Fasting glucose measurement: fasting blood glucose level in venous plasma is ≥ 92mg/dl (5.1mmol/l), a second measurement is recommended. According to the International Association of the Diabetes and Pregnancy Study Groups (IAPDSG) and World Health Organization (WHO) endorsements, a hemoglobin A1C (HbA1C) value of ≥ 5.9% indicates GDM. Table 1 illustrates the GDM screening and diagnosis guidelines provided by various widely recognized organizations.
Physiopathology of GDMGDM is a multifactorial disease whose pathogenesis is not fully understood, but several researchers revealed that dysfunction of β-cells and pregnancy-induced insulin resistance are the most important factors leading to GDM.9 The incapacity of pancreatic β-cells characterizes GDM to respond to the raised demand for insulin during pregnancy, leading to hyperglycemia. During pregnancy, the placenta produces several hormones that are supposed to hinder the action of insulin, which is responsible for regulating blood sugar levels.10
During pregnancy, beta cells undergo hyperplasia and hypertrophy to meet the increased metabolic demands of pregnancy, but if β-cells are unable to meet the increased demands of pregnancy, leading to hyperglycemia. On the other hand, several studies have shown that insulin resistance develops during pregnancy, and the cell’s response to insulin is reduced, which leads to GDM.11 Many observational studies revealed that β-cells, blood sugar, and insulin sensitivity return to normal after the delivery, but they may also lead to T2DM.12,13
Epidemiology of Gestational DiabetesGestational diabetes mellitus (GDM) is a significant global health issue because of its impact adverse on both maternal and neonatal health. The prevalence of GDM varies significantly worldwide, ranging from 1% to >30% 3. A recent report yielded that GDM prevalence was a 6.79-fold increase in obese and 2.29-fold in overweight women.14 Another study from Africa reported a prevalence of 13.6% (95% CI 11-16.2%).15 However, The International Federation of Gynaecology and Obstetrics (FIGO) Initiative on gestational diabetes estimates the prevalence of GDM is 14.5% in the Eastern Mediterranean region.16
In a recent Systematic of the Middle East, the crude GDM prevalence was estimated to be about 11.0% and the most prevalent countries for diabetes mellitus are Iran (32.3%) and Saudi Arabia (24.2%) followed by Qatar (9.7%).17 Whereas, a population-based study in Bahrain reported the prevalence of GDM as 13.5% (n=10495).18 A retrospective study assessed pregnant Omani women with GDM or PGDM and found 581 diabetic women had GDM (90.9%) and only 58 (9.1%) had PGDM.19
Significant variations in GDM prevalence exist worldwide, and such variations may be due to different screening tools and diagnostic criteria, attributed to variations in risk factors, such as overweight/obesity or advanced maternal age.
Prevalence Rates in Saudi ArabiaAccording to the Saudi Medical Journal 2020, “The prevalence of GDM in Saudi Arabia is high compared to other countries. In another cohort study in the Riyadh capital of 9723 women recruited between 2013 and 2015, 24.2% had GDM.5
The prevalence of 19.6% based on the ADA criteria in the capital city Riyadh in KSA may be explained by dietary habits, and by the reasoning that the metabolism is in overdrive during pregnancy, which can exacerbate glucose intolerance and lead to GDM. Another cross-sectional investigation from Riyadh of 13,627 pregnant women selected randomly showed that the prevalence of GDM was 36.6%.20 Another prospective study showed that 39.4% had GDM.21 Table 2 depicts the prevalence rate of different regions of Saudi Arabia.
3.2 Risk Factors for Gestational Diabetes in Saudi ArabiaThe factors influencing the onset of insulin resistance during pregnancy are multifaceted, involving environmental, genetic, and, hormonal factors. Despite the considerable high prevalence of GDM in Saudi Arabia, the pathophysiology of GDM remains incompletely understood.
Several risk factors have been involved in the development of GDM, such as increased maternal age, obesity, ethnic background, family history of T2DM, and a previous history of GDM. In addition, other risk factors such as the previous history of a macrosomic baby, previous adverse pregnancy outcome, glycosuria, polyhydramnios, or large fetus in present pregnancy.17,20,21,22 Among these risk factors, increased maternal weight is the most commonly evaluated reversible risk factor.
Impact/ Complications of Gestational Diabetes in Saudi ArabiaVarious studies from all over the world confirm that maternal and fetal complications are associated with GDM. The fetal complications include macrosomia, neonatal hypoglycemia, polycythemia, shoulder dystocia, hyperbilirubinemia, neonatal respiratory distress syndrome, increased perinatal mortality, and hypocalcemia. Maternal complications include preeclampsia, increased risk of developing diabetes mellitus, and, increased risk of cesarean delivery.23,24
In a retrospective study of Riyadh, researchers found that Saudi pregnant women with higher HbA1c (p=0.0077) had significantly higher blood pressure, and proteinuria (p<0.0001), and were multiparous (p=0.0269). Also, the study revealed significantly shorter gestational periods (p=0.0002), more preterm labor (p<0.0001), more perineal tears (p=0.0406), more miscarriages (p<0.0001), and more operative deliveries (p<0.0001) associated with GDM.25 Another study found a significantly higher incidence of pre-eclampsia (p<0.0001); macrosomia (p=0.0186)preterm delivery (p=0.0226); cesarean section (p=0.0019); higher mean birth weight (p<0.0001) of babies; induction of labor (p<0.0001); large for gestational age infants (p=0.0011); and admission to the neonatal intensive care unit (p=0.0003), compared with the control group.26
However, a cross-sectional study from the Al-Baha region of Saudi Arabia indicated a significant association between GDM and the development of eclampsia (OR = 8.296, 95%CI: 4.353-15.810, p<0.001), as well as an increased risk of thyroid diseases (OR = 2.723, 95%CI: 1.428-5.193, p=0.002).27
A retrospective study of Jeddah city revealed that Postpartum prediabetes was independently predicted by age category ≥45 years (OR=39.94, 95%CI = 4.62-345.06), history of GDM (OR=0.18, 95%CI = 0.03 - 0.97), and A2GDM (OR=6.96, 95%CI = 1.91-25.42).13 Additionally, another recent study found that fetal birth weight and postpartum BMI were significantly higher in the early-onset GDM group.28
Similar results were also revealed by another Riyadh study, that women with GDM were delivered by emergency cesarean section (CS) (odds ratio (OR) 1.30, 95% confidence intervals (CI) (1.02-1.66)), or elective CS (OR 1.72, 95% CI 1.22-2.44, P<0.001). The neonates of the mothers with GDM were significantly heavier and more frequently macrosomia (OR 1.75, 95% CI 1.14-2.71, p<0.001).29 Several studies conclude that glucose intolerance during pregnancy is associated with gestational hypertension and hyperlipidemia as a risk factor for PE.30,31,32
Saudi women’s GDM knowledge and awarenessVarious studies assessed knowledge and awareness of Saudi women’s GDM and revealed that the majority demonstrated ‘poor’ knowledge about GDM.24,33,34,35,36,37 However, A study from Tabuk City found that Saudi women showed good knowledge of GDM and its risk factors, as well as a good attitude regarding the management of GDM and lifestyle modification to reduce its complications.4
Current Guidelines in Saudi ArabiaThe most recent Saudi guidelines for the definition, diagnosis, and management of GDM were published in the Saudi Medical Journal in 20204 and the Saudi National Diabetes Centre (SNDC)(First Edition 2021)(Saudi Diabetes Clinical Practice Guidelines (SDCPG) Saudi National Diabetes Centre (SNDC) (Alsaedi et al. 2020).
Management Strategies for Gestational DiabetesNonpharmacologic approaches include increased physical activity, dietary changes, and glucose monitoring. In patients with GDM is 30 minutes of moderate-intensity aerobic exercise at least 5 days a week or a minimum of 150 minutes per week. Additionally, postprandial exercise is often recommended as this has been shown to help control glucose levels for up to 3 hours after eating.4
Dietary modifications and gestational weight gainGeneral dietary modifications include consuming 3 meals, small to moderate, and 2 to 3 snacks comprised of whole-grain carbohydrates, protein, and unsaturated fats. Figure 2 depicts the management strategy of GDM. Several studies have also revealed that a combination of complex carbohydrates with proteins can help reduce postprandial hypoglycemia. A high-protein snack is also recommended at bedtime to prevent ketosis at night, which can affect fetal neurodevelopment.38,39
Pharmacologic TherapiesInsulin therapy and Oral agents are recommended if the patient’s glycemic control is not controlled by Nonpharmacologic approaches.
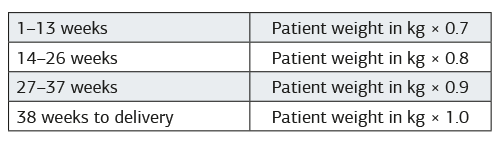
Insulin therapyInsulin dosages must be individualized based on glucose monitoring. Table 3 shows the calculation of the initial total daily Insulin requirement for Gestational Diabetes. Insulin dose is divided into half, with one half recommended as basal insulin at bedtime and the other half divided between 3 meals and given as rapid-acting or regular insulin before meals.40
Oral hypoglycaemic agentsThe oral hypoglycaemic agents include metformin and glyburide. The initial dosage of metformin is typically 500 mg a day for 1 week, increased to twice a day with a maximum dosage of 2,500 to 3,000 mg. Several studies revealed that Metformin has adverse effects, including preterm birth and maternal abdominal pain, diarrhea, macrosomia, neonatal hypoglycemia, or cesarean delivery.39
Glyburide can be initiated at 2.5 mg daily and a maximum dosage of 20 mg. Earlier, glyburide was thought not to cross the placental barrier, but several contemporary study results nullify this belief and reveal that it is associated with an increased risk of neonatal intensive care admission, respiratory distress syndrome, hypoglycemia, and birth injury, as well as possible fetal insulin stimulation. Therefore, glyburide is not recommended by ACOG as a first-line therapy.39
Application of Medical Nutrition Therapy in GDMThe management of GDM includes a personalized medical nutrition therapy plan that aims to ensure sufficient calorie/Nutrient intake to support the health of both the fetus/neonate and the mother, achieve glycemic targets, and bring into line with the weight gain recommendations.41
Standard dietary management of gestational diabetes involves recommendations to choose low glycemic index foods, avoid high glycemic index foods, and encourage increased intake of nutrient-rich foods such as vegetables.42,43
Both ADA and ACOG recommend nutritional counseling by a registered dietician and developing a personalized plan for the patient according to BMI to meet the patient’s caloric demand and avoid excessive weight gain.44,45
Restriction of Energy IntakeStudies have shown that adjusting caloric intake to meet weight gain during pregnancy may be beneficial in reducing the mother’s blood sugar and insulin levels without producing abnormalities in other metabolic disorders.38,41,43 Studies also suggested that severe low-calorie intake during pregnancy may induce maternal ketone production and is adverse to the growth and development of the fetus. Several updated guidelines highlight that whole-diet interventions can be useful tools to improve clinical outcomes.38,41,43,46
Low GI and High Quality of CarbohydratesSeveral studies showed that a low GI diet also had a significant positive effect on pregnancy weight gain and maternal glucose intolerance.41 Both the American College of Obstetricians and Gynaecologists (ACOG) and the Canadian guideline recommend limiting carbohydrate intake to 35% to 45% of the total daily energy intake.
Good Dietary ProteinThe ADA suggested that women with GDM should consume at least 71 g of protein daily during pregnancy to meet pregnancy needs. Although studies have found that a high-protein diet may affect glucose homeostasis by promoting insulin resistance and increasing glucose allogenesis (gluconeogenesis).41 Numerous studies have shown the quality of protein and the risk of GDM and found that intake of animal protein with plant protein may reduce the risk of GDM.10,47
Dietary FatThe ADA recommended that fat intake should account for 30~40% of total energy intake.41,43,48 Several studies demonstrated risk of GDM was lower when plant fat was substituted for carbohydrates, and dietary cholesterol intake was associated with an increased risk of GDM.16,41,43,46,49
Vitamin and Mineral SupplementsDuring pregnancy, a high intake of vitamins and minerals is required, to ensure the needs of both the mother and the fetus. Although vitamin D plays a functional role in insulin secretion and maintenance of glucose metabolic homeostasis, this may be part of the reason for the increased prevalence of GDM caused by vitamin D deficiency.16
However, studies also suggest iodine deficiency and iodine excess are related to the occurrence of GDM, the correlation between iodine concentration and GDM risk may show a U-shaped result.48
Ethical ApprovalNot applicable.
Statistical AnalysisNo statistical analysis was performed because this study is a narrative review based on previously published literature.
Reporting GuidelinesNot applicable.
Limitations
This review is limited by heterogeneity among the included studies, differences in diagnostic criteria for gestational diabetes mellitus, and reliance on regional data from Saudi Arabia. In addition, variations in study design and potential publication bias may affect the generalizability of the findings.
Conclusion
The present study highlights the growing prevalence of this condition and its significant implications for maternal and neonatal health in Saudi Arabia. The epidemiological data indicate an increasing incidence of GDM, which correlates with rising rates of obesity, sedentary lifestyles, and poor dietary habits in the population. Key risk factors such as advanced maternal age, family history of diabetes, and ethnic background, along with environmental and lifestyle factors, are crucial in understanding the patterns of GDM in Saudi women.
Management strategies for GDM in Saudi Arabia emphasize the need for early detection, regular monitoring, and lifestyle modifications, including dietary counseling and physical activity. However, gaps remain in terms of widespread public awareness, healthcare infrastructure, and timely interventions. Enhanced research efforts into the genetic and environmental factors influencing GDM in this population will also contribute to more personalized and effective prevention and treatment strategies.
Declarations
Ethics Declarations
Not applicable for this narrative review.
Animal and Human Rights Statement
Not applicable for this narrative review.
Informed Consent
Not applicable.
Data Availability
No new data were generated or analyzed in this study.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.U., Ö.G.
Methodology: A.U., Ö.G.
Formal Analysis: A.U.
Investigation: A.U., Ö.G.
Data Curation: A.U.
Writing – Original Draft Preparation: A.U.
Writing – Review & Editing: Ö.G.
Supervision: Ö.G.
Abbreviations
AITFL: Anterior inferior tibiofibular ligament
ATFL: Anterior talofibular ligament
AUC: Area under the curve
CI: Confidence interval
CFL: Calcaneofibular ligament
MRI: Magnetic resonance imaging
NPV: Negative predictive value
PPV: Positive predictive value
ROC: Receiver operating characteristic
References
-
Eades CE, Cameron DM, Evans JMM. Prevalence of gestational diabetes mellitus in Europe: a meta-analysis. Diabetes Res Clin Pract. 2017;129:173-181. doi:10.1016/j.diabres.2017.03.030
-
Behboudi-Gandevani S, Amiri M, Bidhendi Yarandi R, Ramezani Tehrani F. The impact of diagnostic criteria for gestational diabetes on its prevalence: a systematic review and meta-analysis. Diabetol Metab Syndr. 2019;11(2):11. doi:10.1186/s13098-019-0406-1
-
Li L, Huang L, Tobias DK, Zhang C. Gestational diabetes mellitus among Asians: a systematic review from a population health perspective. Front Endocrinol (Lausanne). 2022;13:84-331. doi:10.3389/fendo.2022.840331
-
Alsaedi SA, Altalhi AA, Nabrawi MF, Aldainy AA, Wali RM. Prevalence and risk factors of gestational diabetes mellitus among pregnant patients visiting National Guard primary health care centers in Saudi Arabia. Saudi Med J. 2020;41(2):144-150. doi:10.15537/smj.2020.2.24842
-
Wahabi H, Fayed A, Esmaeil S, Mamdouh H, Kotb R. Prevalence and complications of pregestational and gestational diabetes in Saudi women: analysis from Riyadh mother and baby cohort study (RAHMA). Biomed Res Int. 2017;2017(1):1-9. doi:10.1155/2017/6878263
-
Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743-754. doi:10.1016/j.tem.2018.09.004
-
AlJahdali EA, AlSinani NS. Pregnancy outcomes at advanced maternal age in a tertiary hospital, Jeddah, Saudi Arabia. Saudi Med J. 2022;43(5):491-499. doi:10.15537/smj.2022.43.5.20220023
-
Abualhamael S, Mosli H, Baig M, Noor AM, Alshehri FM. Prevalence and associated risk factors of gestational diabetes mellitus at a university hospital in Saudi Arabia. Pak J Med Sci. 2019;35(2):325-329. doi:10.12669/pjms.35.2.498
-
Martín-Estal I, Castorena-Torres F. Gestational diabetes mellitus and energy-dense diet: what is the role of the insulin/IGF axis? Front Endocrinol (Lausanne). 2022;13:916042. doi:10.3389/fendo.2022.916042
-
Hod M, Kapur A, McIntyre HD. Evidence in support of the International Association of Diabetes in Pregnancy Study Groups’ criteria for diagnosing gestational diabetes mellitus worldwide in 2019. Am J Obstet Gynecol. 2019;221(2):109-116. doi:10.1016/j.ajog.2019.01.206
-
Kampmann U, Knorr S, Fuglsang J, Ovesen P. Determinants of maternal insulin resistance during pregnancy: an updated overview. J Diabetes Res. 2019;2019(1):5320156. doi:10.1155/2019/5320156
-
Napoli A, Sciacca L, Pintaudi B, et al. Screening of postpartum diabetes in women with gestational diabetes: high-risk subgroups and areas for improvements—the STRONG observational study. Acta Diabetol. 2021;58(9):1187-1197. doi:10.1007/s00592-021-01707-9
-
Ghamri KA. Insulin requiring gestational diabetes: risk factors and correlation with postpartum diabetes and prediabetes. Pak J Med Sci. 2023;39(5):1260-1267. doi:10.12669/pjms.39.5.7648
-
Paulo MS, Abdo NM, Bettencourt-Silva R, Al-Rifai RH. Gestational diabetes mellitus in Europe: a systematic review and meta-analysis of prevalence studies. Front Endocrinol (Lausanne). 2021;12:691033. doi:10.3389/fendo.2021.691033
-
Muche AA, Olayemi OO, Gete YK. Prevalence and determinants of gestational diabetes mellitus in Africa based on updated diagnostic criteria: a systematic review and meta-analysis. Arch Public Health. 2019;77:1-20.
-
Hod M, Kapur A, Sacks DA, et al. FIGO initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet. 2015;131(Suppl):173-211. doi:10.1016/s0020-7292(15)30007-2
-
Al-Rifai R, Abdo NM, Paulo MS, Saha S, Ahmed LA. Prevalence of gestational diabetes mellitus in the Middle East and North Africa, 2000–2019: a systematic review, meta-analysis, and meta-regression. Front Endocrinol (Lausanne). 2021;12(1):12-14. doi:10.3389/fendo.2021.668447
-
Al Mahroos S, Nagalla DS, Yousif W, Sanad H. A population-based screening for gestational diabetes mellitus in non-diabetic women in Bahrain. Ann Saudi Med. 2005;25(2):129-133. doi:10.5144/0256-4947.2005.129
-
Abu-Heija AT, Al-Bash M, Mathew M. Gestational and pregestational diabetes mellitus in Omani women: comparison of obstetric and perinatal outcomes. Sultan Qaboos Univ Med J. 2015;15(4):e496-e497. doi:10.18295/squmj.2015.15.04.009
-
Al-Rubeaan K, Al-Manaa HA, Khoja TA, et al. A community-based survey for abnormal glucose metabolism among pregnant women (SAUDI-DM). BMJ Open. 2014;4(8):e005906-e005908. doi:10.1136/bmjopen-2014-005906
-
Alfadhli EM, Osman EN, Basri TH, et al. Gestational diabetes among Saudi women: prevalence, risk factors, and pregnancy outcomes. Ann Saudi Med. 2015;35(3):222-230. doi:10.5144/0256-4947.2015.222
-
Teh WT, Teede HJ, Paul E, et al. Risk factors for gestational diabetes mellitus: implications for screening guidelines. Aust N Z J Obstet Gynaecol. 2011;51(1):26-30. doi:10.1111/j.1479-828x.2011.01292.x
-
Lindsay RS, Mackin ST, Nelson SM. Gestational diabetes mellitus: right person, right treatment, right time? BMC Med. 2017;15(1):163-165. doi:10.1186/s12916-017-0925-2
-
Almazyad NS, Jahan S. Awareness of gestational diabetes mellitus among women in Saudi Arabia. Cureus. 2024;16(4):e59345. doi:10.7759/cureus.59345
-
Buhary BM, Almohareb O, Aljohani N, et al. Glycemic control and pregnancy outcomes in patients with diabetes in pregnancy: a retrospective study. Indian J Endocrinol Metab. 2016;20(4):481-490.
-
Gasim T. Gestational diabetes mellitus: maternal and perinatal outcomes in Saudi women. Oman Med J. 2012;27(2):140-144. doi:10.5001/omj.2012.29
-
Osman T, Keshk EA, Alghamdi MA, et al. Prevalence of adverse pregnancy outcomes in women with and without gestational diabetes mellitus. Cureus. 2024;16(1):e52421-e52425. doi:10.7759/cureus.52421
-
Alsulami SS, Ghamri KA. Early-onset versus late-onset gestational diabetes mellitus: a cohort study. Saudi Med J. 2023;44(7):703-710. doi:10.15537/smj.2023.44.7.20230193
-
Wahabi HA, Esmaeil SA, Fayed A, Alzeidan RA. Gestational diabetes mellitus: maternal and perinatal outcomes in Saudi Arabia. J Egypt Public Health Assoc. 2013;88(2):104-108. doi:10.1097/01.epx.0000430392.57811.20
-
Aziz F, Khan MF, Moiz A. Gestational diabetes mellitus, hypertension, and dyslipidemia as risk factors of preeclampsia. Sci Rep. 2024;14(1):6182-6188. doi:10.1038/s41598-024-56790-z
-
Zahra A, Hassan S, Parveen N, Iqbal N, Batool A. Pregnancy-related complications due to obesity and gestational diabetes mellitus. Afr J Reprod Health. 2022;26(2):38-46.
-
Parveen N, Iqbal N, Batool A, et al. Macrosomia predictors and pregnancy outcomes in gestational diabetes. Pak J Med Sci. 2022;38(5):1126-1131. doi:10.12669/pjms.38.5.5809
-
Alharthi AS, Althobaiti KA, Alswat KA. Gestational diabetes mellitus knowledge among Saudi women. Open Access Maced J Med Sci. 2018;6(8):1522-1526. doi:10.3889/oamjms.2018.284
-
Wafa MH, Ayoub AI, Bukhari TA, et al. Knowledge and attitude regarding gestational diabetes mellitus among pregnant women in Saudi Arabia. Cureus. 2023;15(11):e48151-e48155. doi:10.7759/cureus.48151
-
Ali TM, Keshk EA, Almaqadi OM, et al. Awareness of gestational diabetes mellitus among women in Saudi Arabia. Cureus. 2023;15(12):e50163-e50169. doi:10.7759/cureus.50163
-
Abualsaud RM, Baghdadi ES, Bukhari AA, Katib HA. Awareness of gestational diabetes mellitus among females in Saudi Arabia: a cross-sectional study. J Fam Med Prim Care. 2022;11(7):3442-3448. doi:10.4103/jfmpc.jfmpc_2485_21
-
Hakim R, Alqerafi A, Malibari W, et al. Understanding of gestational diabetes mellitus among pregnant women in Saudi Arabia. Cureus. 2023;15(10):e46937-e46943. doi:10.7759/cureus.46937
-
Saud A, Saja A, Saad A, et al. Saudi diabetes clinical practice guidelines. Saudi Health Council. 2021;1(1):1-137.
-
Champion ML, Jauk VC, Biggio JR, et al. Early gestational diabetes screening based on ACOG guidelines. Am J Perinatol. 2024;41(Suppl):e641-e647. doi:10.1055/a-1925-1134
-
Szmuilowicz ED, Josefson JL, Metzger BE. Gestational diabetes mellitus. Endocrinol Metab Clin North Am. 2019;48(3):479-493. doi:10.1016/j.ecl.2019.05.001
-
Vasile FC, Preda A, Ștefan AG, et al. Medical nutrition therapy in gestational diabetes mellitus. J Diabetes Res. 2021;2021(1):5266919-5266920. doi:10.1155/2021/5266919
-
Hernandez TL, Van Pelt RE, Anderson MA, et al. Diet composition and insulin resistance in gestational diabetes mellitus. Diabetes Care. 2016;39(1):39-42.
-
Kintiraki E, Goulis DG. Gestational diabetes mellitus: multidisciplinary treatment approaches. Metabolism. 2018;86:91-101. doi:10.1016/j.metabol.2018.03.025
-
American Diabetes Association Professional Practice Committee. Diagnosis and classification of diabetes: Standards of Care in Diabetes—2024. Diabetes Care. 2023;47(Suppl 1):S20-S42.
-
Caughey AB, ACOG Practice Bulletin No. 190: gestational diabetes mellitus. Obstet Gynecol. 2018;131(2):e49-e64. doi:10.1097/aog.0000000000002501
-
Lipscombe L, Booth G, Butalia S, et al. Pharmacologic glycemic management of type 2 diabetes in adults. Can J Diabetes. 2018;42(Suppl 1):S88-S103. doi:10.1016/j.jcjd.2017.10.034
-
Wu W, Tang N, Zeng J, et al. Dietary protein patterns and risk of gestational diabetes mellitus. Nutrients. 2022;14(8):1623-1624. doi:10.3390/nu14081623
-
Wei X, Zou H, Zhang T, et al. Gestational diabetes mellitus: role of medical nutrition therapy. Nutrients. 2024;16(8):1217-1219. doi:10.3390/nu16081217
-
Feig DS, Corcoy R, Jensen DM, et al. Diabetes in pregnancy outcomes: a systematic review and proposed codification of definitions. Diabetes Metab Res Rev. 2015;31(7):680-690. doi:10.1002/dmrr.2640
Figures
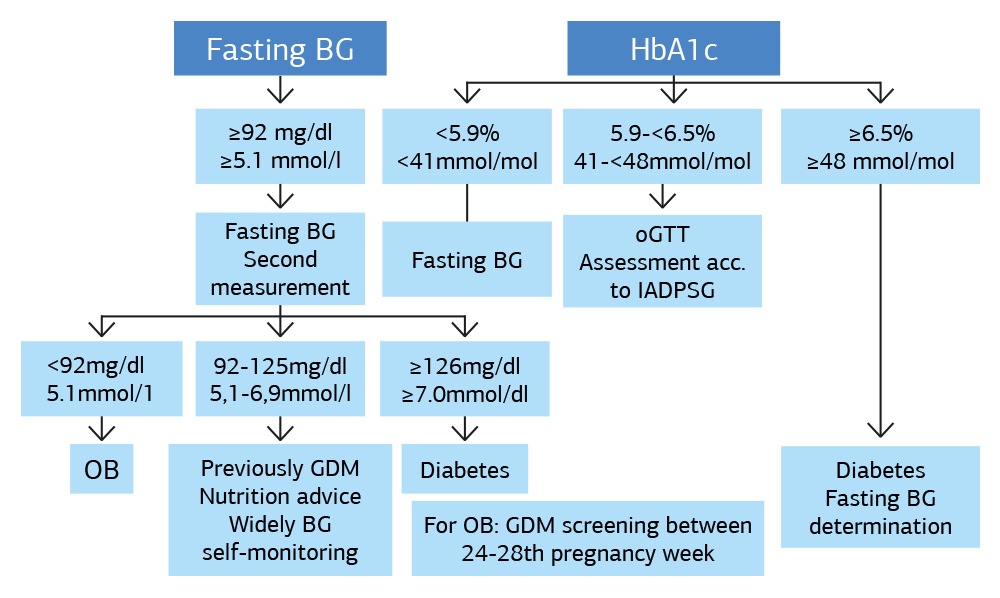
Figure 1. Diagnostic Methods for GDM
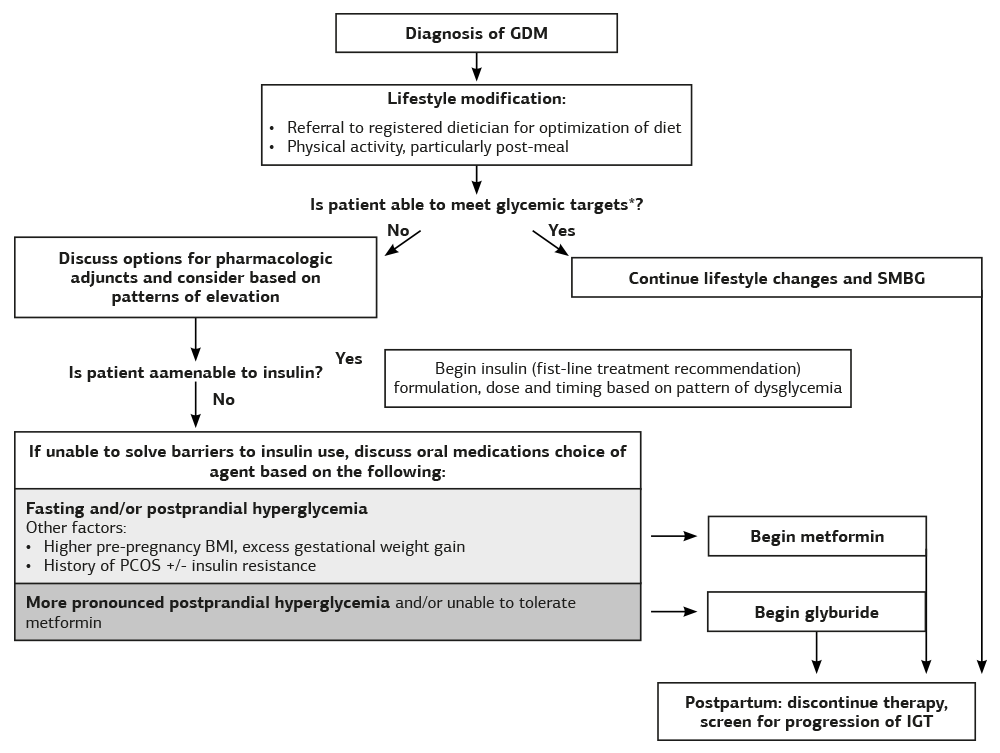
Figure 2. The management strategy of GDM
Tables
Table 1. Guidelines for diagnosis of GDM by different organizations
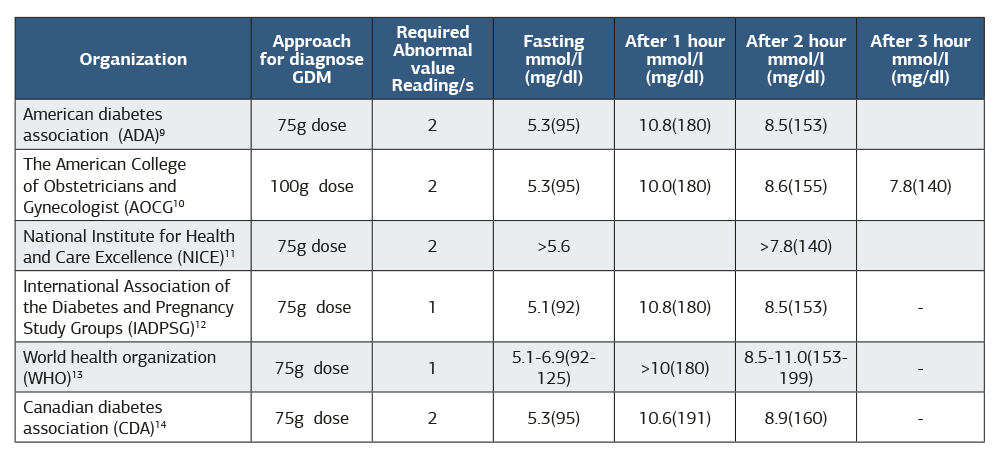
Table 2. Prevalence GDM in Saudi Arabia
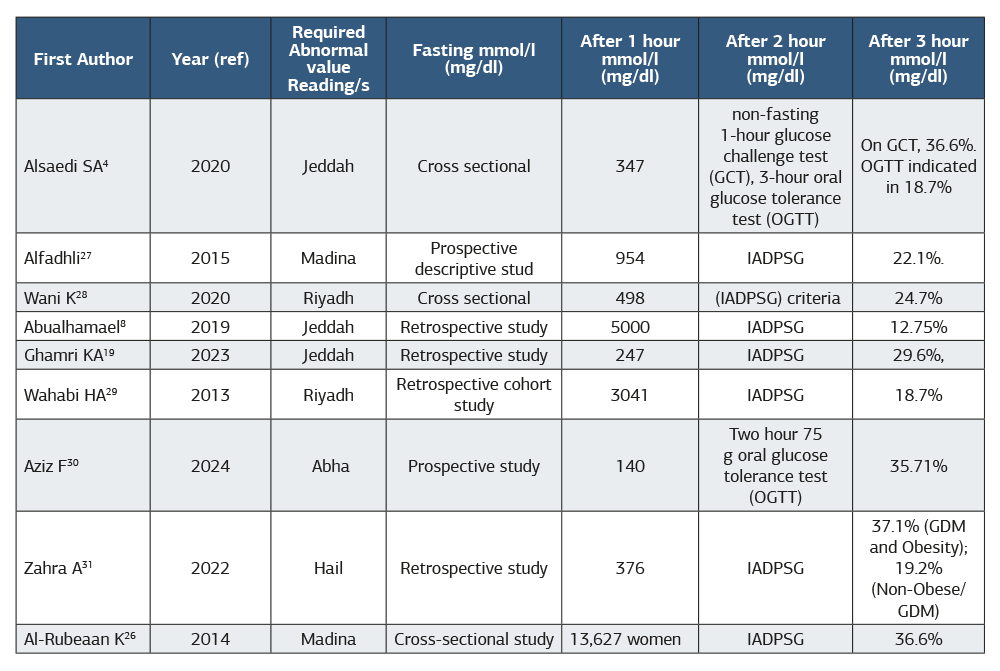
Table 3. Calculation of initial total daily insulin requirement for gestational diabetes
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Fatima Waseem. The impact of gestational diabetes in Saudi Arabia: epidemiology, risk factors, and management strategies. Ann Clin Anal Med 2026;17(6):655-661. doi:10.4328/ACAM.22543
- Received:
- January 3, 2025
- Accepted:
- February 4, 2025
- Published Online:
- February 26, 2025
- Printed:
- June 1, 2026