
Comparison of conventional method and perforated balloon treatment in no-reflow phenomenon following percutaneous coronary intervention
No-reflow management with perforated balloon
Authors
Abstract
Aim Cardiovascular diseases are among the leading causes of mortality and morbidity worldwide. The coronary no-reflow phenomenon refers to reperfusion damage in myocardial tissue without visible blockage in coronary arteries. It is associated with increased rates of heart failure, cardiogenic shock, and mortality. This study aimed to propose an alternative approach to conventional therapy for managing this condition.
Methods This single-center retrospective study included 81 patients who met the inclusion criteria. All patients underwent PCI (Percutaneous Coronary Intervention), and those who developed no-reflow were divided into three groups. Group 1 received perforated balloon-mediated therapy (PBT), Group 2 received intracoronary tirofiban, and Group 3 received intracoronary tirofiban-adenosine. The groups were compared based on TIMI flow grade outcomes.
Results TIMI-3 flow grade was significantly higher in the PBT group, as indicated by triple test analysis (p=0.033). Pairwise comparisons revealed a significant difference between the PBT and tirofiban-adenosine groups (p=0.005). In regression analyses, treatment type was significant in single-variable regression (p=0.02) but not in multi-variable regression (p=0.07). Vascular diameter showed significance in single-variable (p=0.009) and was identified as an independent predictor in multi-variable regression analysis (p=0.019). A negative correlation between vascular diameter and TIMI flow grade was observed.
Conclusion The combination of tirofiban, adrenaline, and glyceryl trinitrate, administered with PBT, appears to offer a promising alternative to conventional therapy. However, limitations include the single-center retrospective design and a relatively small sample size. Further randomized controlled trials are necessary to validate these findings.
Keywords
Introduction
Percutaneous coronary intervention (PCI) therapy constitutes the basis for treatment in many acute coronary syndrome (ACS) patients.1 With advancements in technology, the success rate of PCI has increased. However, procedure-related complications may be seen.2 One of the complications that develops during PCI and which affects prognosis is the no-reflow phenomenon.3 In guidelines, there is no clear information concerning the treatment of the no-reflow phenomenon. Various pharmacological methods are administered via the intracoronary route for the treatment of the no-reflow phenomenon. However, adequate clinical studies and the level of evidence for these methods are missing. These are adenosine, glycoprotein (GP) 2b 3a inhibitors, calcium channel blockers, Beta (β)-2 receptor agonists, fibrinolytic agents.4 In previous studies, adenosine has been administered as intracoronary perforated balloon-mediated treatment.5 In our study, it was aimed to use adrenaline, glyceryl trinitrate, and GP 2b 3a inhibitors via intracoronary perforated balloon and to compare the same with conventional therapy.
In this context, a better understanding will be provided for no-reflow treatment, and its treatment and complications will be managed better. Our hypothesis is that coronary no-reflow and TIMI scoring will improve with this PBT (Perforated Balloon Mediated Therapy) treatment.
Materials and Methods
Our study was designed as a single-center, retrospective study. Patients who were administered percutaneous coronary intervention (PCI) in our hospital between March 2019 and April 2023 were screened. In this group, patients who had developed no-reflow phenomenon were included in our study. Ages, genders, chronic conditions, laboratory results, coronary angiogram, and PCI images and data were recorded in-hospital information system.
Patients with diabetes mellitus (DM) consisted of patients who had previously been diagnosed with DM. Patients with HBa1c value ≥ 6.5 or patients who had not been diagnosed with DM and whose fasting blood glucose (FBG) levels had been measured twice as 126 mg/dL or over or post-prandial glucose level measured twice as 200 mg/dL or over, were identified as diabetic. Hypertensive patients were defined as patients with systolic blood pressure 140 mmHg or over and diastolic blood pressure 90 mmHg or over.
Included patients:
• Patients ≥ 18 years of age
• Patients who had been administered PCI
Exclusion criteria were:
• Patients with active infection
• Patients who had undergone major surgery within the last month
• Active malignity
• Patients with substance addiction
• Patients with familial hyperlipidemia
No-reflow patients, who had satisfied the inclusion criteria, were included in the study. The ethics committee application for the dissertation has been approved by our hospital ethics committee on May 26, 2023.
In our study, the no-reflow phenomenon has been identified according to TIMI grading and patients with scores of 2 or less were enrolled. The patient flow chart is shown in Figure 1.
Patients were divided into three groups:
• Patients, administered intracoronary tirofiban (n = 35)
• Patients, administered intracoronary tirofiban–adenosine (n = 25)
• Patients, treated with perforated balloon-mediated therapy (PBT)(n = 21)
In our study, the perforated balloon-mediated therapy (PBT) was performed using balloons originally utilized for pre-dilatation during PCI. These balloons were inflated to a pressure of up to 12 atm using an indeflator, and then punctured carefully with the tip of an insulin needle to create perforations. After puncturing, all air was thoroughly evacuated from the balloon to avoid air embolism.
The modified balloon was then advanced to a distal location beyond the lesion. It was inflated gently to 2–3 atm and then slowly pulled back toward the lesion site to administer the therapeutic agents locally.
Regarding the drug mixture:
• Adrenaline (1 mg/mL, 1:1000 concentration) was first diluted by taking 1 mL of the stock solution and diluting it to 10 mL with saline, resulting in a concentration of 100 mcg/mL.
• Then, 1 mL of this diluted solution (containing 100 mcg adrenaline) was further diluted to 10 mL, yielding a final concentration of 10 mcg/mL adrenaline.
• This final 1 mL solution (10 mcg adrenaline) was loaded into the deflator for administration through the perforated balloon.
Additionally, glyceryl trinitrate (250 mcg) was diluted in saline and combined with the adrenaline solution as above, to create the drug mixture used in PBT.
Tirofiban was prepared at a concentration of 0.0125 mg/kg for intracoronary administration through the perforated balloon.
In the control groups:
• Intracoronary adenosine was administered at doses of 100 mcg or 200 mcg.
• Intracoronary tirofiban was administered at 0.025 mg/kg via the guiding catheter.
All medication dosages and administration details were extracted from the hospital information system.
TIMI flow grades were assessed by two experienced interventional cardiologists independently, using coronary angiography.
Primary endpoint of our study was the improvement in TIMI flow grade.
This study was conducted in accordance with the principles of the Declaration of Helsinki. And no artificial intelligence [AI]-assisted technologies, including large language models [LLMs] or chatbots, were used in the generation of the content or writing of this manuscript.
Baseline differences between groups, particularly in age and laboratory parameters, were evaluated and addressed using multivariate logistic regression analysis. Due to the retrospective design and limited sample size, additional statistical adjustments such as stratification or sensitivity analyses were not feasible.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Bilkent City Hospital (Date: 26.05.2023, Decision No: E2-23-4159)
Statistical AnalysisFor statistical analysis, SPSS 21.0 for Windows Statistics Package Software (SPSS Inc., Chicago, IL, USA) was used. Continuous variables were shown as mean ± standard deviation or median (interquartile range), and categoric variables were shown as a figure and percentage. In order to test the normality of distribution, the Kolmogorov-Smirnov test was applied. In continuous parameters with normal distribution, the One-Way ANOVA test was used to show the inter-group differences. Türkiye test was used for intergroup post-hoc analysis. In the comparison of more than two groups without normal distribution Kruskal-Wallis test was used, and in case of statistical significance, the Mann-Whitney U test was used for non-matched groups. Differences between treatment groups to categorical variables were analyzed using the chi-square test. Spearman correlation analysis was made to investigate the relationship between TIMI flow and vascular diameter. Logistic regression analysis was used to investigate the relationship between TIMI flow grade 3 and other variables. Variables with a p value of < 0.1 in single-variable logistic regression analysis were included in the multivariable logistic regression model. p<0.05 was deemed statistically significant. Normally distributed data are shown as mean ± standard deviation, and non-normally distributed data are shown as median (interquartile range).
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Our study included 81 patients treated with PCI, consisting of 22 (27.2%) females and 59 (72.8%) males. The mean age was 64.1 ± 11 years. Comorbidities included hypertension in 35 (43.2%), diabetes mellitus in 35 (43.2%), and coronary artery disease in 31 (38.3%) patients.
Patients were divided into three groups: 21 received perforated balloon-mediated therapy (PBT), 35 received intracoronary tirofiban via guiding catheter, and 25 received intracoronary tirofiban-adenosine via guiding catheter. The mean age in the PBT group was significantly higher (69.3 ± 11.7 years) compared to the tirofiban (62.5 ± 9.7; p=0.023) and tirofiban-adenosine (61.9 ± 11.2; p=0.035) groups. No significant age difference was found between the tirofiban and tirofiban-adenosine groups.
Albumin levels differed significantly between the PBT and tirofiban groups (median.[IQR], 39.5.[35.5–41.7] vs 42.[40–43]; p=0.005), whereas no other significant intergroup differences were observed. Similarly, triglyceride levels differed significantly between the PBT and tirofiban groups (85.[71.5–95.5] vs 122.[91–190]; p=0.007), while no significant differences were found in the other comparisons.
Patient comorbidities, as presented in Table 1, were similar among the groups, and no statistically significant differences were observed with respect to the other baseline characteristics (p>0.05). Detailed baseline laboratory characteristics are presented in Supplementary Table 1.
The angiographic characteristics of the patients are presented in (The detailed data are provided in Supplementary Table 2). Median stent length was significantly greater in the PBT group compared with the other groups (36.[24–47] vs 29.[20–38], p=0.048; and 36.[24–47] vs 24.[20–32], p=0.006).
We have detected a negative correlation between vascular diameter and TIMI flow grade. Shown in Figure 2.
Single- and multi-variable regression analysis of TIMI-3 flow predictor parameters is given in (The detailed data are provided in Supplementary Table 3). Among the patients, there was a significant difference with respect to vascular diameter in single-variable regression analysis (p=0.009). Vascular diameter was also found as an independent predictor in multivariable regression analysis (p=0.019).
TIMI-3 flow was found to be higher in the PBT group among patients (p=0.033). In regression analyses, while the form of treatment showed a significant difference in singular regression analysis (p=0.02), in multi-variable regression analysis, it was not determined as an independent predictor (p=0.07).
Discussion
In our study, PCI patients who developed no-reflow were compared between those treated with intracoronary tirofiban and those treated with intracoronary adenosine-tirofiban via PBT. The PBT group showed higher rates of TIMI 2 and TIMI 3 flow, which are generally considered success criteria in no-reflow treatment.
Previous studies, such as Khan et al., reported intracoronary adrenaline to be more effective and safer than adenosine for no-reflow in ACS patients, with 90% achieving TIMI-3 flow in the adrenaline group versus 78% in the adenosine group.6 Stoel et al. demonstrated improved no-reflow indices with high-dose intracoronary adenosine compared to placebo in STEMI patients.7 Our adrenaline dose in PBT was similar.
Patel et al. applied PBT in no-reflow patients with TIMI ≤2, administering adenosine initially and using PBT if TIMI-3 flow was not reached, achieving TIMI III flow in 87.6% of patients without complications.5 Rezkalla et al. emphasized pharmacological treatments like nitroprusside and calcium blockers, alongside thrombectomy, tailored to the dominant mechanism of no-reflow.8 Nitroprusside showed improvements in TIMI flow during PCI but lacked conclusive clinical outcome data.9,10 In our PBT group, nitroprusside was dosed cautiously (3 mcg/kg, max 350 mcg).
Gibson et al. showed that GP IIb/IIIa inhibitor eptifibatide improved microvascular perfusion post-stent implantation.11 A meta-analysis confirmed intracoronary tirofiban’s efficacy over conventional drugs but highlighted bleeding risks.12 Our tirofiban dosing adhered to PCI guidelines.
Lim et al. compared intracoronary adenosine alone versus combined with nicorandil for no-reflow treatment, showing the combination was safe and more effective in improving TIMI scores and reducing in-hospital death and heart failure.13 Huang et al. found nicardipine effective and safe retrospectively but called for more data.14
Mitochondrial reperfusion injury plays a key role in no-reflow. Piot et al. demonstrated that ciclosporin A reduced infarct size in STEMI patients, though it had no significant effect on no-reflow clinically; animal studies showed benefits on microcirculation.15,16 Small studies by Taniyama et al. and Werner et al. suggested intracoronary verapamil improves microvascular function and reverses no-reflow.17,18
Advanced age is known to increase endothelial dysfunction and arterial stiffness, impairing coronary flow.19 In our study, the mean age was higher in the PBT group compared to the others. Despite this, the PBT group showed greater improvement in TIMI flow, suggesting that PBT may have a potential benefit even in elderly patients.
We found a negative correlation between vessel diameter and TIMI-3 flow grade. Although literature lacks direct data on this, we believe it relates to post-dilatation. Post-dilatation, commonly performed after stent implantation to improve stent expansion, can cause distal embolization—one of the main mechanisms of no-reflow and thus increase no-reflow risk.20,21,22
While TIMI flow grade is a widely used endpoint in coronary reperfusion studies, it remains a somewhat subjective measure. More objective angiographic parameters, such as myocardial blush grade or TIMI frame count, were not assessed in this retrospective study. Furthermore, clinical outcomes, including mortality and reinfarction rates, were not included as endpoints.
Given the single-center, retrospective design and relatively small sample size, our findings should be interpreted with caution. These results are exploratory and hypothesis-generating, warranting confirmation in larger, prospective, and ideally randomized multicenter studies.
Limitations
This study was limited by its single-center retrospective design and relatively small sample size.
Conclusion
To our knowledge, our study is the first to compare the combination of tirofiban, adrenaline, and glyceryl trinitrate given in combination with PBT with other conventional treatments for the no-reflow phenomenon. Our study showed that the combination of tirofiban, adrenaline, and glyceryl trinitrate administered with PBT may be a better alternative to other conventional no-reflow phenomenon treatments in the treatment of no-reflow phenomenon in patients undergoing percutaneous coronary intervention. High incidence of age-related development of no-reflow phenomenon following PCI and high rate of success of PBT treatment in the advanced age group also showed that PBT therapy could be administered safely in this patient group. In addition, since an increase in vascular diameter would yield a post-dilatation requirement during and after the procedure, we showed that it could be a factor to increase the risk of the no-reflow phenomenon.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
The single-center and retrospective design of our study and the small number of patients are among the limitations of our study. More randomized controlled studies are required on this subject. The retrospective and observational design of this study inherently limits control over group comparability and potential confounding variables. Although multivariate regression was employed to adjust for observed baseline imbalances, especially in age and laboratory values, additional methods such as stratification or sensitivity analyses could not be performed due to the sample size and design constraints. These factors should be taken into account when interpreting the findings. Therefore, larger prospective and randomized studies are warranted to confirm and extend our results. In addition, the use of TIMI flow grade as the primary endpoint represents a subjective measure of reperfusion. More objective angiographic and clinical endpoints, such as myocardial blush grade, TIMI frame count, mortality, and reinfarction, were not evaluated and should be incorporated in future prospective studies.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures involving human participants were performed in accordance with institutional and national ethical standards and with the Declaration of Helsinki and its later amendments.
Informed Consent
Due to the retrospective design of the study, informed consent was waived by the ethics committee.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: O.O., A.C.Ö., A.G.E.
Methodology: O.O., A.C.Ö.
Formal analysis: O.O., İ.E.Y.
Investigation: O.O., M.A.E., Ç.Y.
Data curation: İ.E.Y., M.A.E.
Writing – original draft: O.O.
Writing – review & editing: A.B.A., A.G.E.
Supervision: A.G.E.
Abbreviations
ACS: Acute coronary syndrome
DM: Diabetes mellitus
FBG: Fasting blood glucose
GP: Glycoprotein
LLM: Large language model
PCI: Percutaneous coronary intervention
PBT: Perforated balloon-mediated therapy
SPSS: Statistical Package for the Social Sciences
TIMI: Thrombolysis in Myocardial Infarction
References
-
Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022;327(7):662-675. doi:10.1001/jama.2022.0358
-
Chen D, Jepson N. Coronary stent technology: a narrative review. Med J Aust. 2016;205(6):277-281. doi:10.5694/mja16.00444
-
Schwartz BG, Kloner RA. Coronary no reflow. J Mol Cell Cardiol. 2012;52(4):873-882. doi:10.1016/j.yjmcc.2011.06.009
-
Case BC, Satler LF. The challenges of the coronary no-reflow phenomenon. Catheter Cardiovasc Interv. 2021;97(4):612-613. doi:10.1002/ccd.29571
-
Patel T, Shah S, Gulati R, Kwan T, Cohen MG, Pancholy S. Perforated balloon technique: a simple and handy technique to combat no-reflow phenomenon in the coronary system. Catheter Cardiovasc Interv. 2018;92(5):890-894. doi:10.1002/ccd.27477
-
Khan KA, Qamar N, Saghir T, et al. Comparison of intracoronary epinephrine and adenosine for no-reflow in normotensive patients with acute coronary syndrome: COAR trial. Circ Cardiovasc Interv. 2022;15(2):e011408. doi:10.1161/circinterventions.121.011408
-
Stoel MG, Marques KM, de Cock CC, et al. High dose adenosine for suboptimal myocardial reperfusion after primary PCI: a randomized placebo-controlled pilot study. Catheter Cardiovasc Interv. 2008;71(3):283-289. doi:10.1002/ccd.21334
-
Rezkalla SH, Dharmashankar KC, Abdalrahman IB, et al. No-reflow phenomenon following percutaneous coronary intervention for acute myocardial infarction: incidence, outcome, and effect of pharmacologic therapy. J Interv Cardiol. 2010;23(5):429-436. doi:10.1111/j.1540-8183.2010.00561.x
-
Pasceri V, Pristipino C, Pelliccia F, et al. Effects of the nitric oxide donor nitroprusside on the no-reflow phenomenon during coronary interventions for acute myocardial infarction. Am J Cardiol. 2005;95(11):1358-1361. doi:10.1016/j.amjcard.2005.01.082
-
Airoldi F, Briguori C, Cianflone D, et al. Frequency of slow coronary flow following successful stent implantation and effect of nitroprusside. Am J Cardiol. 2007;99(7):916-920. doi:10.1016/j.amjcard.2006.10.057
-
Gibson CM, Cohen DJ, Cohen EA, et al. Effect of eptifibatide on coronary flow reserve following coronary stent implantation: an ESPRIT substudy. Am J Cardiol. 2001;87(11):1293-1295. doi:10.1016/s0002-9149(01)01524-7
-
Qin T, Xie L, Chen MH. Meta-analysis of randomized controlled trials on the efficacy and safety of intracoronary administration of tirofiban for the no-reflow phenomenon. BMC Cardiovasc Disord. 2013;13(1):1-7.
-
Lim SY, Bae EH, Jeong MH, et al. Effect of combined intracoronary adenosine and nicorandil on no-reflow phenomenon during percutaneous coronary intervention. Circ J. 2004;68(10):928-932. doi:10.1253/circj.68.928
-
Huang RI, Patel P, Walinsky P, et al. Efficacy of intracoronary nicardipine in the treatment of no-reflow during percutaneous coronary intervention. Catheter Cardiovasc Interv. 2006;68(5):671-676. doi:10.1002/ccd.20885
-
Piot C, Croisille P, Staat P, et al. Effect of cyclosporine on reperfusion injury in acute myocardial infarction. N Engl J Med. 2008;359(5):473-481. doi:10.1056/nejmoa071142
-
Zalewski J, Claus P, Bogaert J, et al. Cyclosporine A reduces microvascular obstruction and preserves left ventricular function deterioration following myocardial ischemia and reperfusion. Basic Res Cardiol. 2015;110(1):1-17.
-
Taniyama Y, Ito H, Iwakura K, et al. Beneficial effect of intracoronary verapamil on microvascular and myocardial salvage in patients with acute myocardial infarction. J Am Coll Cardiol. 1997;30(5):1193-1199. doi:10.1016/s0735-1097(97)00277-5
-
Werner GS, Lang K, Kuehnert H, Figulla HR. Intracoronary verapamil for reversal of no-reflow during coronary angioplasty for acute myocardial infarction. Catheter Cardiovasc Interv. 2002;57(4):444-451. doi:10.1002/ccd.10375
-
Celermajer DS, Sorensen KE, Spiegelhalter DJ, et al. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J Am Coll Cardiol. 1994;24(2):471-476. doi:10.1016/0735-1097(94)90305-0
-
Jiang J, Tian NL, Cui HB, et al. Post-dilatation improves stent apposition in patients with ST-segment elevation myocardial infarction receiving primary percutaneous intervention: a multicenter, randomized controlled trial using optical coherence tomography. World J Emerg Med. 2020;11(2):87-92. doi:10.5847/wjem.j.1920-8642.2020.02.004
-
Soylu K, Ataş AE, Yenerçağ M, et al. Effect of routine postdilatation on final coronary blood flow in primary percutaneous coronary intervention patients without angiographic stent expansion problems. J Investig Med. 2018;66(8):1096-1101. doi:10.1136/jim-2018-000725
-
Gao P, Lin W, Wang H, Du F. Application of post-dilation in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention. Int J Clin Exp Med. 2018;11(11):12657-12663. doi:10.1097/md.0000000000012943
Figures
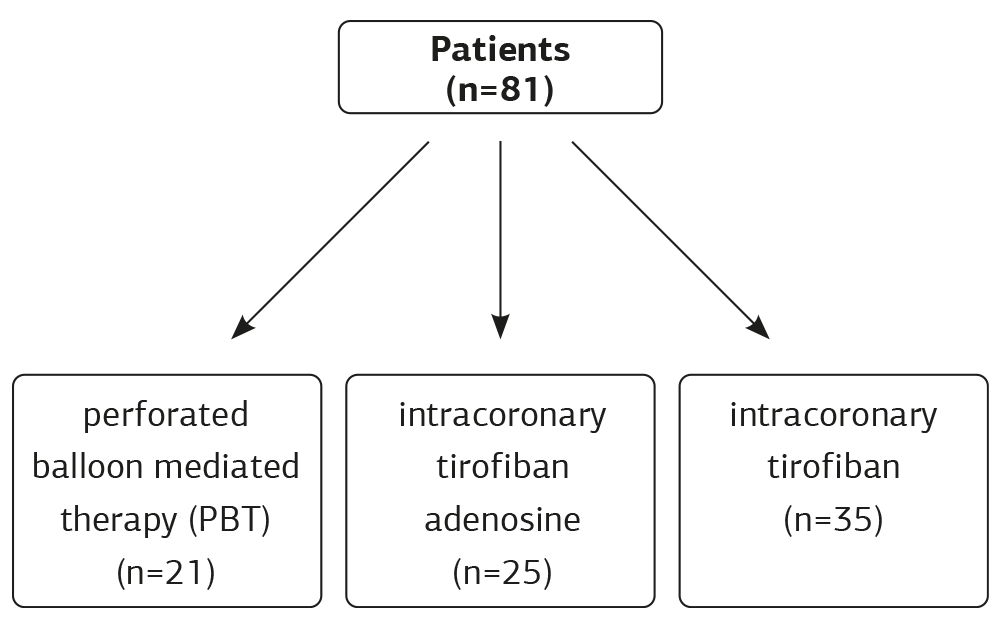
Figure 1. Patient flow chart
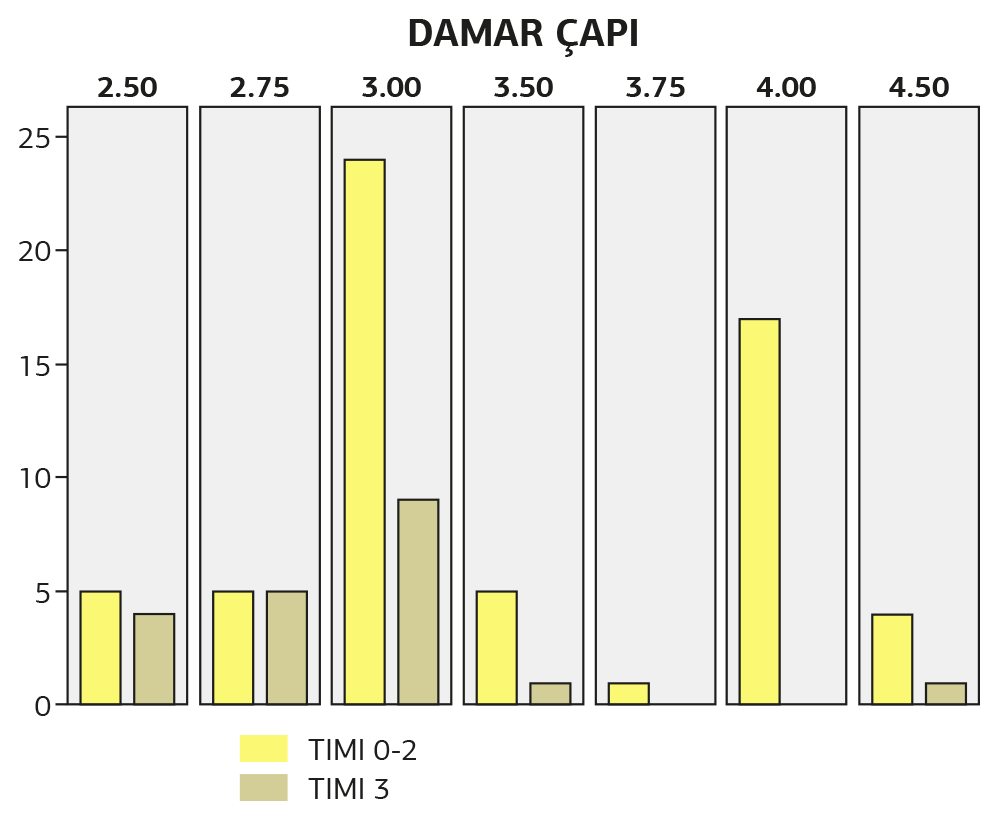
Figure 2. Relationship between TIMI flow and vascular diameter
Tables
Table 1. Comparison of patients’ baseline characteristics between the groups
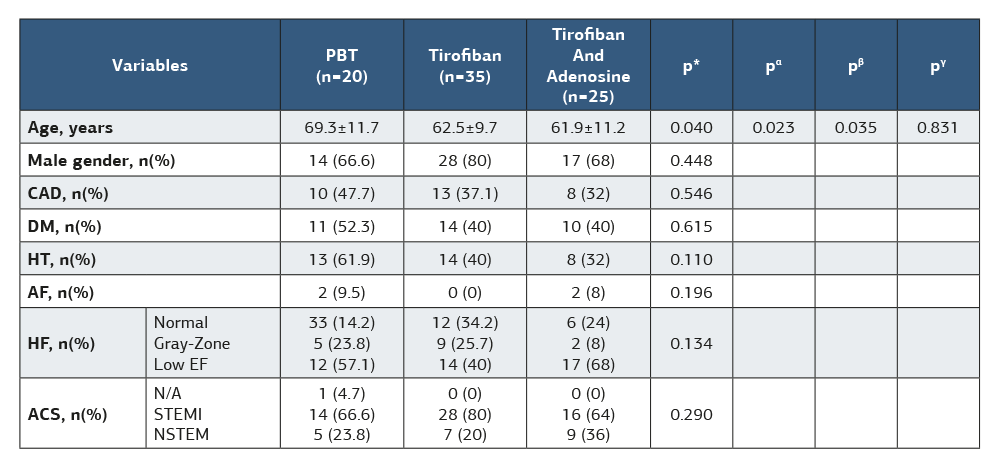
ACS: acute coronary syndrome; AF: atrial fibrillation; DM: diabetes mellitus; EF: ejection fraction; HDL: high-density lipoprotein; HT: hypertension; CAD: history of coronary arterial disease; LDL: low-density lipoprotein. * p-value between all groups α p-value between the PBT group and the tirofiban group β p-value between the PBT group and the tirofiban-adenosine group γ p-value between the Tirofiban group and tirofiban-adenosine group
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozan Oğuz, Ali Can Özkan, İlyas Emre Yakıcı, Mehmet Akif Erdöl, Çağrı Yayla, Adnan Burak Akçay, Ahmet Göktuğ Ertem. Comparison of conventional method and perforated balloon treatment in no-reflow phenomenon following percutaneous coronary intervention. Ann Clin Anal Med 2026;17(6):549-554. doi:10.4328/ACAM.22759
- Received:
- May 29, 2025
- Accepted:
- August 25, 2025
- Published Online:
- August 27, 2025
- Printed:
- July 1, 2026