
The impact of erector spinae plane block on postoperative recovery quality after inguinal hernia repair: a retrospective study
ESP block and quality of recovery
Authors
Abstract
Aim We aimed to investigate whether a unilateral erector spinae plane (ESP) block performed at the end of surgery improves early postoperative recovery in patients undergoing open inguinal hernia repair under spinal anaesthesia.
Methods This retrospective observational study included patients who underwent elective unilateral open inguinal hernia repair with spinal anaesthesia. Patients were divided into two groups according to the use of an ESP block at the end of surgery: ESP block (n = 37) and control (n = 36). The primary outcome was the Quality of Recovery-15 (QoR-15) score at postoperative 24 hours. Secondary outcomes were resting numerical rating scale (NRS) pain scores, rescue analgesic requirement, and time to first mobilisation.
Results Demographic and clinical characteristics were similar between the groups. The 24-hour QoR-15 score was significantly higher in the ESP group (132.2 ± 5.7 vs 117.5 ± 8.95; p < 0.001). NRS pain scores at 4, 8, 12, and 24 hours were lower in patients receiving an ESP block. Most patients in the ESP group (70.3%) required no additional analgesia, whereas rescue analgesics were frequently used in the control group (p < 0.001). Time to mobilisation was shorter in the ESP group (4.62 ± 0.86 vs 6.14 ± 1.25 hours; p < 0.001).
Conclusion A unilateral ESP block performed at the end of surgery was associated with better recovery, less pain, reduced analgesic consumption, and earlier mobilisation. It may be considered a practical component of multimodal analgesia for open inguinal hernia repair.
Keywords
Introduction
Inguinal hernia repair (IHR) is one of the most frequently performed surgical procedures in general surgery practice, with approximately 20 million operations carried out worldwide each year.1 Unfortunately, nearly 40% of patients2 experience moderate to severe acute pain in the early postoperative period, and chronic pain develops in approximately 10-12% of patients2 following open IHR. Inadequate postoperative analgesia not only reduces patient comfort but may also delay early mobilization and adversely affect the overall recovery process.3
In clinical practice, postoperative analgesia for inguinal hernia surgery relies on multimodal strategies that combine systemic agents such as non-steroidal anti-inflammatory drugs, opioids, and intravenous lidocaine with regional anesthesia techniques, most commonly the transversus abdominis plane (TAP) block and the quadratus lumborum block (QLB).4,5,6 Recommendations aimed at reducing pain after IHR were first published by Joshi et al. in 20123 and subsequently updated in 2020 by the Procedure-Specific Postoperative Pain Management (PROSPECT) working group.7 According to the PROSPECT guidelines, the addition of regional techniques-such as local anesthetic infiltration and/or ilioinguinal/iliohypogastric nerve block or TAP block-to multimodal analgesia is recommended.
Since its initial description in 2016,8 the erector spinae plane (ESP) block has attracted considerable interest for postoperative pain management following various surgical procedures. The erector spinae plane block is technically straightforward, can be performed safely with ultrasound guidance, and may provide analgesia across multiple dermatomes.9 On the basis of these characteristics and its reported efficacy in a range of surgical settings, the technique has been described by some authors as a “magic bullet”.9 However, systematic reviews and meta-analyses pooling randomized trials have demonstrated that the magnitude of its effect varies across different surgical fields and that there is substantial heterogeneity in outcomes, suggesting that its efficacy may depend on the type of surgery and the comparator technique used.10,11,12
Nevertheless, randomized controlled trials evaluating the efficacy of the ESP block in inguinal hernia repair remain limited, and the existing literature is insufficient to draw definitive conclusions.13,14,15 In particular, the impact of the ESP block on postoperative recovery and functional outcomes in patients undergoing open IHR under spinal anesthesia has not been adequately investigated.
Although pain is an important component of postoperative recovery, it does not capture all aspects of the patient experience. To obtain a broader view of recovery following surgery, the Quality of Recovery-15 (QoR-15) questionnaire was used in the present study. For this reason, the QoR-15 scale was chosen in the present study to assess the effect of the ESP block on postoperative recovery.16
The aim of this retrospective, controlled study was to evaluate the effects of an ultrasound-guided unilateral ESP block administered at the end of surgery on postoperative quality of recovery and early functional recovery in patients undergoing elective unilateral open inguinal hernia repair under spinal anesthesia. Secondary outcome measures included postoperative pain intensity, rescue analgesic requirements, and time to first mobilization.
Materials and Methods
This study was designed as a retrospective observational study. Patient data were collected from individuals who underwent inguinal hernia repair between 1 January 2025 and 30 November 2025. As the study involved retrospective analysis of routinely collected clinical data without any intervention or direct patient contact, ethics committee approval was obtained after completion of data collection. Owing to the retrospective nature of the study, informed consent was waived. All data were analyzed in an anonymized manner.
Patients aged 18-70 years who underwent elective unilateral open inguinal hernia repair under spinal anesthesia within the specified period were included. Exclusion criteria were incomplete clinical records; use of an anesthetic technique other than spinal anesthesia; emergency or bilateral inguinal hernia surgery; additional surgical procedures performed during the same operation; use of any regional anesthesia technique other than the ESP block in the postoperative period; and inability to perform reliable postoperative assessment due to major postoperative complications.
Patients were divided into two groups according to whether an ESP block was administered in the postoperative period. The ESP block group consisted of patients who received a unilateral ESP block at the end of surgery for postoperative analgesia, whereas the control group included patients who were managed with the standard postoperative analgesia protocol without an ESP block. In both groups, the surgical technique was open inguinal hernia repair, and spinal anesthesia was used in all patients.
Data were obtained from the Hospital Information Management System, anesthesia records, operating theatre forms, and postoperative ward follow-up charts. Recorded demographic variables included age, sex, height, weight, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, and comorbidities. Surgical and anesthetic variables included the duration of surgery and the side of the operation.
Postoperative pain intensity was assessed using the numerical rating scale (NRS) as documented in the clinical records. Pain scores at rest and during movement were recorded separately at postoperative 1, 2, 4, 6, 12, and 24 hours. Postoperative rescue analgesia and administered analgesics were identified from clinical records. QoR-15 scores recorded preoperatively and at 24 hours were used to evaluate recovery, and time to first mobilization was calculated from nursing documentation. Postoperative adverse effects were determined from ward follow-up notes and discharge summaries.
Ethical ApprovalThis study was approved by the Muğla Sıtkı Koçman University Medical and Health Sciences Research Ethics Committee (Date: 28 January 2026, Decision No: 30). Owing to the retrospective nature of the study, informed consent was not required. All data were analyzed in an anonymized manner.
Statistical AnalysisAll analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was checked with the Shapiro-Wilk test. Depending on distribution characteristics, data were summarized as mean ± standard deviation or, when appropriate, as median with interquartile range.
The primary outcome of the study was quality of recovery at 24 hours postoperatively, assessed by the QoR-15 score, and comparisons were made between patients who did and did not receive an ESP block. Continuous variables were compared between groups using the independent samples t-test.
Postoperative pain scores (NRS) at rest and during movement were analyzed at predefined time points. Changes over time and differences between groups were examined using repeated-measures analysis of variance. When the assumption of sphericity was not met, the Greenhouse-Geisser correction was applied. Pairwise comparisons across time points were adjusted using the Bonferroni method.
Categorical variables, including sex, ASA physical status classification, and rescue analgesic requirement, were compared between groups using the Pearson chi-square test or Fisher’s exact test, as appropriate.
All statistical tests were two-sided, and a p-value of less than 0.05 was considered statistically significant. There were no missing data for the analysed variables.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
During the study period, 84 patients who underwent elective unilateral open inguinal hernia repair under spinal anesthesia were retrospectively screened. After applying the inclusion and exclusion criteria, 11 patients were excluded: three due to a body mass index greater than 35 kg/m² and eight because of incomplete clinical records. A total of 73 patients were included in the final analysis. The patient selection process is shown in Figure 1.
Of the included patients, 37 were allocated to the ESP block group and 36 to the control group. Baseline demographic and clinical characteristics are presented in Supplementary Table 1. There were no significant differences between the groups in terms of age, sex distribution, height, weight, body mass index, ASA physical status classification, duration of spinal block, or duration of surgery (all p-values > 0.05), indicating that the groups were comparable at baseline.
Preoperative and postoperative 24-hour quality of recovery scores are summarized in Supplementary Table 1. Preoperative QoR-15 scores were similar between the ESP block and control groups (139.6 ± 3.95 vs 137.5 ± 6.53, respectively; p = 0.109). At 24 hours postoperatively, QoR-15 scores were significantly higher in the ESP block group compared with the control group (132.2 ± 5.7 vs 117.5 ± 8.95; p < 0.001).
Postoperative analgesic requirements and time to first mobilization are presented in Supplementary Table 1. A significant difference was observed between groups regarding rescue analgesic use (p < 0.001). In the ESP block group, 70.3% of patients did not require additional analgesia, whereas only 8.3% of patients in the control group required no rescue analgesic. In contrast, 63.9% and 27.8% of patients in the control group required one and two doses of rescue analgesics, respectively. Time to first mobilization was significantly shorter in the ESP block group than in the control group (4.62 ± 0.86 hours vs 6.14 ± 1.25 hours; p < 0.001).
Postoperative NRS pain scores at rest over time are illustrated in Figure 2, and between-group comparisons at individual time points are detailed in Supplementary Table 2. Pain scores were similar between groups during the early postoperative period (1 and 2 hours). From the 4th postoperative hour onward, resting NRS scores were consistently lower in the ESP block group. Significant differences were observed at 4, 8, 12, and 24 hours, with the largest difference noted at 24 hours (0.41 ± 0.64 in the ESP block group vs 2.14 ± 0.90 in the control group; p < 0.001).
The overall postoperative pain trajectory was further evaluated using repeated-measures analysis of variance. As shown in Supplementary Table 2, there were significant effects of time (p < 0.001), group (p < 0.001), and a significant group × time interaction (p < 0.001), indicating that the pattern of pain reduction over time differed significantly between the ESP block and control groups.
No serious perioperative or postoperative complications were observed in either group. There were no significant differences between groups with respect to postoperative nausea, vomiting, or other recorded adverse effects.
Discussion
In the present study, the application of a unilateral ESP block at the end of surgery was associated with improved early postoperative recovery in patients undergoing open inguinal hernia repair under spinal anaesthesia. Patients who received an ESP block had higher QoR-15 scores, lower postoperative pain scores, reduced need for rescue analgesics, and earlier mobilization compared with those managed with standard postoperative analgesia alone. These findings suggest that the ESP block can contribute positively to both subjective and functional aspects of recovery in this surgical setting.
The available literature on the use of the ESP block in inguinal hernia surgery remains limited. A randomized controlled study in laparoscopic inguinal hernia repair reported lower postoperative pain scores, reduced opioid consumption, and improved QoR-40 scores in patients receiving ESP block compared with controls.13 Although that study involved a minimally invasive approach and a different recovery assessment tool, the overall direction of benefit is consistent with the findings of the present study.
The analgesic role of ESP block has also been explored outside the context of spinal anesthesia. In one randomized trial, ESP block was used as the primary anesthetic technique and was reported to provide surgical conditions comparable to spinal anesthesia, together with lower postoperative pain scores and reduced analgesic requirements.15 While this approach differs from our study design, the postoperative analgesic advantages observed in that trial support the potential role of ESP block as an effective regional technique.
In contrast, studies comparing the ESP block with intrathecal opioid use have shown different results. In open inguinal hernia repair, Mattiazzi et al. reported that intrathecal morphine provided superior postoperative analgesia compared with ESP block, at the cost of a higher incidence of opioid-related side effects such as nausea and pruritus.14 These findings suggest that while ESP block may not provide analgesia as intense as intrathecal opioids, it offers a more favorable side-effect profile, which may be advantageous in selected patient populations.
Recent systematic reviews and meta-analyses further support the use of the ESP block in inguinal hernia surgery, while highlighting variability in its effectiveness depending on the comparator technique and overall analgesic regimen. A recent meta-analysis demonstrated significantly lower early postoperative pain scores, particularly at 6 and 12 hours, as well as a reduced incidence of postoperative nausea and vomiting in patients receiving ESP block.17 However, no consistent differences were observed at 24 hours or in total analgesic consumption. In the present study, the sustained benefit at 24 hours may be related to the absence of intrathecal opioid use in our standard analgesic protocol.
Comparisons between the ESP block and other regional techniques have yielded mixed results. One study reported lower postoperative analgesic consumption with a transversalis fascia plane block compared with the ESP block in a selected patient population.18 In our cohort, however, the ESP block was associated with fewer rescue analgesic requirements and earlier mobilization. While these findings do not establish ESP block as superior to other regional techniques, they support its role as a practical and effective option in open inguinal hernia repair performed under spinal anesthesia, particularly when minimizing postoperative opioid exposure is a priority.
The PROSPECT recommendations for open inguinal hernia repair emphasize the principles of multimodal analgesia rather than endorsing a single superior regional block. In routine clinical practice, more than one regional technique may be used, with the choice often guided by institutional protocols and clinician experience. Although the ESP block is not listed as a standard regional technique in the PROSPECT recommendations, its use has increased in recent years due to its technical simplicity and favorable safety profile. In this context, our findings indicate that the ESP block should not be viewed as a replacement for established regional techniques, but rather as an additional analgesic option in patients undergoing open inguinal hernia repair under spinal anesthesia without intrathecal opioid use.
The present study has several strengths. In contrast to many regional anesthesia studies that focus solely on pain scores, we evaluated postoperative recovery using the validated QoR-15 questionnaire, providing a broader assessment of patient well-being. Objective functional outcomes, including time to first mobilization, were also included. Furthermore, by restricting the cohort to patients undergoing surgery under spinal anesthesia and excluding those with high BMI or bilateral procedures, potential confounding factors were minimized.
Limitations
Several limitations should also be acknowledged. Retrospective and observational design relies on the accuracy of existing medical records and nursing documentation. The single-center nature of the study may limit the generalizability of the findings to other clinical settings. Although the study was adequately powered for the primary outcome, the relatively small sample size suggests that larger, multicenter studies are needed to confirm these results. In addition, only early postoperative outcomes were assessed, and the potential effect of ESP block on the development of chronic post-surgical pain could not be evaluated. Finally, observer bias cannot be fully excluded due to the non-randomized study design.
Conclusion
The ultrasound-guided ESP block significantly improves postoperative quality of recovery following open inguinal hernia repair under spinal anesthesia, proving to be a valuable analgesic addition at the end of the surgical procedure. Beyond its superior analgesic efficacy and substantial opioid-sparing effect, the ESP block facilitates earlier mobilization, which is a cornerstone of modern fast-track surgical protocols. By improving both subjective patient-reported outcomes and objective functional recovery metrics, the ESP block emerges as a highly effective and safe component of multimodal analgesia for this patient population.
Declarations
Ethics Declarations
This study was approved by the Muğla Sıtkı Koçman University Medical and Health Sciences Research Ethics Committee (Date: 28 January 2026, Decision No: 30). All procedures were carried out in accordance with the ethical standards of the institutional and national research committees and with the principles of the Declaration of Helsinki. Patient data were analyzed anonymously, and confidentiality was strictly maintained.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.Y., B.A.
Methodology: E.Y., B.A.
Formal Analysis: E.Y.
Investigation: E.Y., A.C.
Data Curation: E.Y., A.C.
Writing – Original Draft Preparation: E.Y., B.A.
Writing – Review & Editing: B.A., M.K.T.
Supervision: M.K.T.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
AI Usage Disclosure
Artificial intelligence tools were used only for language editing and improvement of grammar and readability. The scientific content, data analysis, interpretation of results, and conclusions were developed entirely by the authors.
Abbreviations
ASA: American Society of Anesthesiologists
BMI: Body Mass Index
ESP: Erector Spinae Plane
IHR: Inguinal Hernia Repair
NRS: Numerical Rating Scale
PROSPECT: Procedure-Specific Postoperative Pain Management
QLB: Quadratus Lumborum Block
QoR-15: Quality of Recovery-15
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
TAP: Transversus Abdominis Plane
References
-
Köckerling F, Simons MP. Current concepts of inguinal hernia repair. Visc Med. 2018;34(2):145-150. doi:10.1159/000487278
-
Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618-1625. doi:10.1016/S0140-6736(06)68700-X
-
Joshi GP, Kehlet H. Postoperative pain management in the era of ERAS: an overview. Best Pract Res Clin Anaesthesiol. 2019;33(3):259-267. doi:10.1016/j.bpa.2019.07.016
-
Gao T, Zhang JJ, Xi FC, et al. Evaluation of transversus abdominis plane block in hernia surgery. Clin J Pain. 2017;33(4):369-375. doi:10.1097/AJP.0000000000000412
-
Zhou Y, Chen M, Zhang Y, Zhou H, Yu X, Chen G. Ilioinguinal/iliohypogastric nerve block versus transversus abdominis plane block for pain management following inguinal hernia repair: a systematic review and meta-analysis. Medicine (Baltimore). 2019;98(42):e17545. doi:10.1097/MD.0000000000017545
-
Öksüz G, Bilal B, Gürkan Y, et al. Quadratus lumborum block versus transversus abdominis plane block in children undergoing low abdominal surgery: a randomized controlled trial. Reg Anesth Pain Med. 2017;42(5):674-679. doi:10.1097/AAP.0000000000000645
-
Coppens S, Gidts J, Huynen P, Van de Velde M, Joshi GP. Pain management after open inguinal hernia repair: an updated systematic review and procedure-specific postoperative pain management (PROSPECT/ESRA) recommendations. Acta Anaesthesiol Belg. 2020;71(Suppl 1):45-56.
-
Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621-627. doi:10.1097/AAP.0000000000000451
-
Chin KJ, Barrington MJ. Erector spinae block: a magic bullet for postoperative analgesia? Anesth Analg. 2019;129(1):8-9. doi:10.1213/ANE.0000000000004140
-
Huang W, Wang W, Xie W, Chen Z, Liu Y. Erector spinae plane block for postoperative analgesia in breast and thoracic surgery: a systematic review and meta-analysis. J Clin Anesth. 2020;66:109900. doi:10.1016/j.jclinane.2020.109900
-
Fanelli A, Torrano V, Cozowicz C, Mariano ER, Balzani E. Opioid-sparing effect of erector spinae plane block for various surgeries: a meta-analysis of randomized controlled trials. Minerva Anestesiol. 2021;87(8):903-914. doi:10.23736/S0375-9393.21.15356-8
-
Cai Q, Liu GQ, Huang LS, et al. Effects of erector spinae plane block on postoperative pain and side effects in adult patients undergoing surgery: a systematic review and meta-analysis. Int J Surg. 2020;80:107-116. doi:10.1016/j.ijsu.2020.05.038
-
Altınsoy S, Özkan D, Akelma FK, Ergil J. Analgesic efficacy of ultrasound-guided unilateral erector spinae plane block for laparoscopic inguinal hernia repair: a randomized controlled study. Turk J Med Sci. 2022;52(3):631-640. doi:10.55730/1300-0144.5355
-
Sakae TM, Mattiazzi APF, Fiorentin JZ, Brandao J, Benedetti RH, Takaschima AKK. Ultrasound-guided erector spinae plane block for open inguinal hernia repair: a randomized controlled trial. Braz J Anesthesiol. 2022;72(1):49-54. doi:10.1016/j.bjane.2021.04.032
-
Kaçmaz M, Bolat H, Erdoğan A. Comparison of spinal anesthesia and erector spinae plane block in unilateral inguinal hernia surgery: a randomized clinical trial. J Minim Access Surg. 2024;20(2):154-162. doi:10.4103/jmas.jmas_367_22
-
Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, Dennis A. Minimal clinically important difference for quality of recovery scales. Anesthesiology. 2016;125(1):39-45. doi:10.1097/ALN.0000000000001158
-
Pompeu BF, Marcolin P, Silva MP, et al. Erector spinae plane block following inguinal hernia repair in adults: a systematic review and meta-analysis. Hernia. 2025;29(1):141. doi:10.1007/s10029-025-03333-8
-
Çelik HK, Tulgar S, Bük ÖF, et al. Comparison of the analgesic efficacy of ultrasound-guided transversalis fascia plane block and erector spinae plane block in patients undergoing open inguinal hernia repair under spinal anesthesia. Korean J Anesthesiol. 2024;77(2):255-264. doi:10.4097/kja.23404
Figures
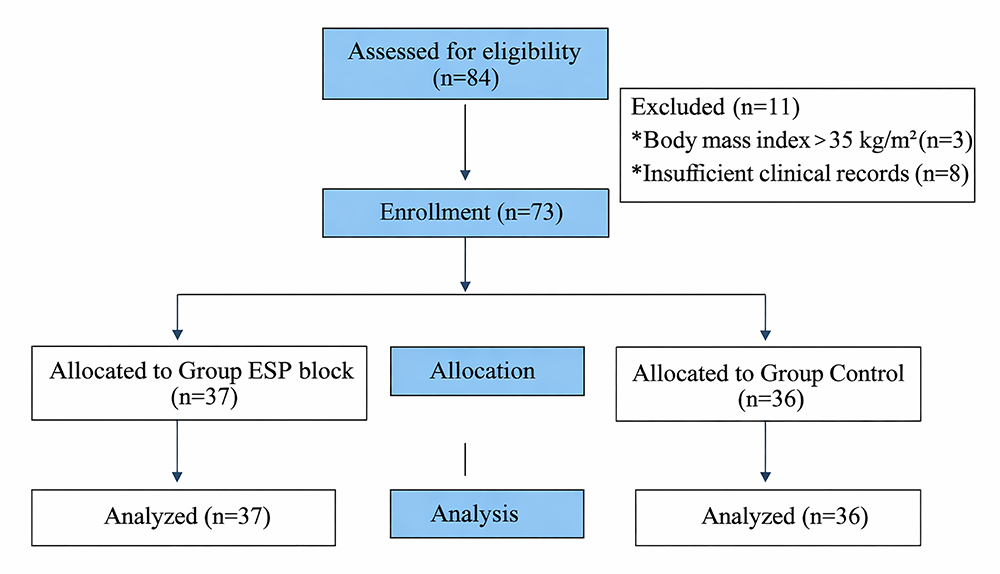
Figure 1. Flowchart of patient inclusion and exclusion The diagram illustrates patient screening, exclusion criteria, group allocation, and final analysis
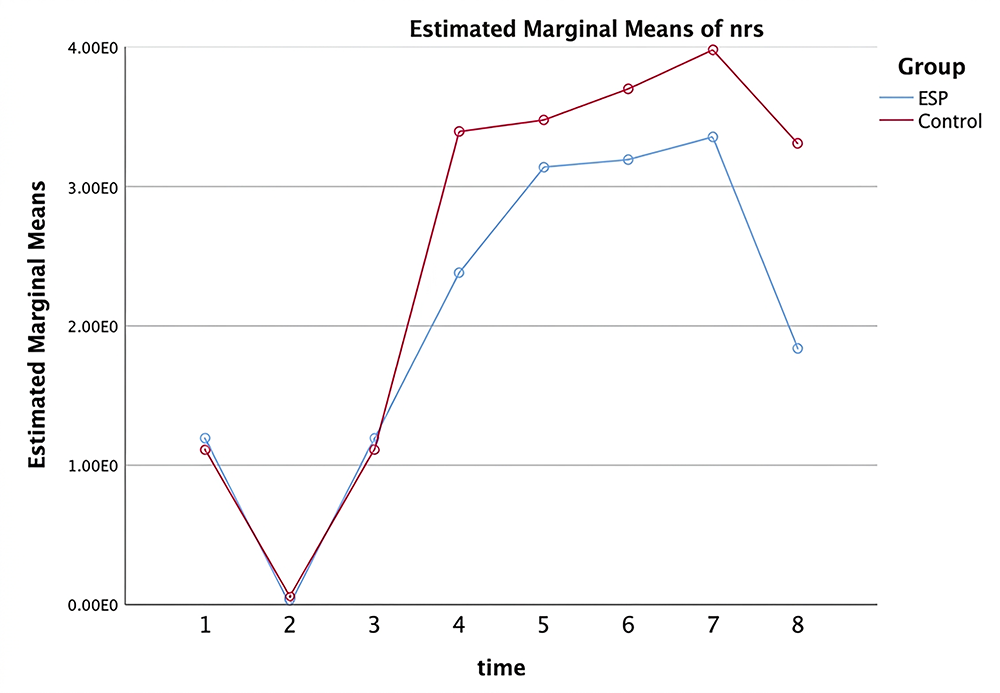
Figure 2. Postoperative Numerical Rating Scale (NRS) pain scores at rest over time in the ESP block and control groups Pain scores were recorded at predefined postoperative time points. From the 4th postoperative hour onward, NRS scores were significantly lower in the ESP block group compared with the control group
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Eylem Yaşar, Başak Altıparmak, Ali Çiftçi, Melike Korkmaz Toker. The impact of erector spinae plane block on postoperative recovery quality after inguinal hernia repair: a retrospective study. Ann Clin Anal Med 2026;17(Suppl 2):S172-176. doi:10.4328/ACAM.50068
- Received:
- February 5, 2026
- Accepted:
- March 16, 2026
- Published Online:
- March 16, 2026
- Printed:
- March 20, 2026