
Abstract
Aim Dermatoporosis is a chronic syndrome of cutaneous insufficiency that occurs as the protective function of the skin diminishes with age. This loss of skin function can result in complications such as atrophy, bleeding, and necrosis. This study aimed to investigate the characteristics of patients with dermatoporosis at dermatology outpatient clinics in a tertiary hospital.Methods This study included patients aged ≥ 60 years who were diagnosed with dermatoporosis and visited dermatology outpatient clinics between August 2024 and August 2025.Results Of the 126 patients, 46% (n = 58) were women and 54% (n = 68) were men. The most common comorbidities were hypertension (55.6%), type 2 diabetes mellitus (38.1%), and hyperlipidemia (41.3%). Fifty-two patients (41.3%) used oral anticoagulants, with acetylsalicylic acid being the most commonly used (72.5%, n = 37). The most frequently diagnosed dermatological condition was dermatitis. Thirty-three patients (26.2%) used topical steroids and 13 (10.3%) used oral corticosteroids. The average duration of topical steroid use was 12.4 ± 17.9 weeks, and that of oral corticosteroid use was 16.0 ± 33.0 weeks. The most common stage of dermatoporosis was stage 1 (n = 97, 77%). There was no significant difference in dermatoporosis stages based on sex (p = 0.36). The most prevalent sites of dermatoporosis were the forearms, dorsal aspect of the hands, lower legs, and dorsal aspect of the feet.Conclusion Research on dermatoporosis is essential to delay advanced skin aging and increase awareness among health care professionals. Ultimately, this will lead to improved treatment outcomes for affected patients in the future.
Keywords
Introduction
The term "dermatoporosis" first appeared in the literature in the early 2000s to emphasize the medical issues resulting from premature skin aging, beyond just aesthetic concerns.1 Individuals with dermatoporosis have thinner and more delicate skin that is prone to tearing, and in advanced stages, they may develop deep dissecting hematomas, which require immediate medical attention.1
Similar to osteoporosis, in which bone mass gradually decreases, dermatoporosis results from the gradual loss of the main structural elements of the skin.2 Dermatoporosis, also known as chronic cutaneous insufficiency syndrome, is a skin fragility syndrome.3 It is characterized by localized purple patches on the extensor surfaces of the upper extremities in elderly individuals, as well as skin and subcutaneous tissue atrophy.3 Symptoms may include senile purpura, actinic purpura, or Bateman's purpura.3 Morphological signs of dermatoporosis usually appear between 70 and 80 years of age. By the time an individual reaches 80 years of age, the clinical effects of dermatoporosis, such as skin fragility and related complications, become more pronounced.2 Studies have shown that dermatoporosis is highly prevalent among the elderly, with women being more susceptible than men.1 Nowadays, with the increasing number of elderly patients over the age of 80, there has been a growing discussion about an epidemic of dermatoporosis.2
Currently, there are limited studies on dermatoporosis. This study aimed to investigate the features of dermatoporosis in patients aged >60 years at dermatology outpatient clinics in a tertiary hospital.
Materials and Methods
This study included patients aged ≥60 years who were diagnosed with dermatoporosis and visited dermatology outpatient clinics between August 2024 and August 2025. Demographic information of all patients was collected, including medical history, Fitzpatrick skin type, body mass index, sunscreen use, sun exposure, smoking and alcohol habits, coffee consumption history (drinking less than one cup per day), current medications, history and duration of oral and systemic steroid use, and details on menstruation, pregnancy, childbirth, and breastfeeding for female patients. The presence and severity of dermatoporosis and its location on the body were recorded.
Patients’ evaluation of the clinical stage of dermatoporosis:4
• Stage 1: Skin thinning, senile purpura, pseudoscars
• Stage 2: Skin thinning, senile purpura, pseudoscars, skin laceration (<10)
• Stage 3: Skin thinning, senile purpura, pseudoscars, skin lacerations (≥ 10)
• Stage 4: Skin thinning, senile purpura, pseudoscars, skin laceration (≥10), dissecting hematomas
Patients who met the following criteria were excluded from the study:
• Psychiatric illness
• Malignancy
• Human immunodeficiency virus (HIV) infection
• Dementia or Alzheimer's diseaseEthical ApprovalThe study was approved by Ankara Etlik City Hospital Scientific Research Evaluation and Ethics Committee (Date: 2024-07-10, No: AEŞH-BADEK-2024-565).Statistical AnalysisAll analyses were conducted using Jamovi version 2.3.28 software. Descriptive analyses were performed to determine the means, standard deviations, frequencies, and minimum and maximum values of the variables. We assessed the normal distribution of the data using the Shapiro-Wilk and Kolmogorov-Smirnov tests. We used the chi-square (χ2) test to compare the differences between the categorical variables. A p-value of less than 0.05 was considered statistically significant, based on a 95% confidence interval.Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
A total of 126 patients were included in this study. Of the patients, 46.0% were women (n = 58), and 54% were men (n = 68). The mean age of the patients was 69.1 ± 6.48 years. The mean body mass index (BMI) of the patients was 27.8 ± 4.42. Of the patients with BMI < 25, 73% were men and 27% were women. Of those with BMI > 30, 72.2% were men and 27.8% were women. According to the Fitzpatrick skin type, 58 patients (46.0%) had type 3 skin, 50 patients (39.7%) had type 2 skin, 15 patients (11.9%) had type 4 skin, and 3 patients had type 1 skin. The comorbidities included hypertension in 70 patients (55.6%), hyperlipidemia in 52 (41.3%), type 2 diabetes mellitus in 48 (38.1), hypothyroidism in 10 (7.9%), and chronic kidney disease in 6 (4.8%). A total of 53.2% (n = 67) of the patients were active smokers. Six patients (4.8%) consumed alcohol, and 45 (35.7%) had a history of coffee consumption. Nineteen patients (15.1%) used sunscreen, and 34 (27%) had a history of excessive sun exposure (continuous exposure, such as occupational sun exposure, or short and intense sun exposure, such as sunbathing). Thirty-three patients (26.2%) received topical steroids. Fifteen patients (45.5%) used topical betamethasone dipropionate, 15 (45.5%) used topical mometasone furoate, two (6.1%) used topical clobetasol propionate, and one (3.0%) used topical methylprednisolone. Thirteen patients (10.3%) were treated with oral corticosteroids. The mean duration of topical steroid use was 12.4 ± 17.9 weeks, and that of oral corticosteroid use was 16.0 ± 33.0 weeks. A significant difference was found between dermatoporosis stages according to oral and topical steroid use (p<0.001 and p<0.001, respectively) (Tables 1 and 2). The mean age at the first menstruation was 10.1 ± 0.97 years, and the mean age at the last menstruation was 50.5 ± 3.16 years. The mean age at the first pregnancy was 19.4 ± 4.13 years, and the mean age at the last pregnancy was 29.0 ± 5.99 years. The mean number of pregnancies in 55 patients was 3.60 ± 1.91, and the mean number of abortions in 29 patients with a history of abortion was 1.46 ± 0.50. Seven patients underwent cesarean sections, and the mean number of cesarean sections was 1.57 ± 0.78 (1-3). 53 patients had a history of breastfeeding, and the mean duration of breastfeeding was 22.3 ± 16.5 months. No differences were found in dermatoporosis stages based on sex (p = 0.36) (Table 3). Fifty-two patients (41.3%) used oral anticoagulants, and acetylsalicylic acid was the most commonly used medication (72.5%, n = 37). The most common dermatological condition diagnosed during outpatient clinic visits was dermatitis. The assessment of dermatoporosis revealed that the most common stage was stage 1 (n = 97, 77%), followed by stage 2 (n = 23, 18.3%), and stage 3 (n = 6, 4.8%), in descending order of frequency. The most common locations for dermatoporosis were the forearms, dorsal aspect of the hands, lower legs, and dorsal aspect of the feet. The detailed data are provided in Supplementary Tables 1 and 2.Discussion
Prevalence studies on dermatoporosis are being conducted in several countries.5 In a study conducted in France, the Index Dermatoporosis Assessment (IDA) was developed for the self-diagnosis of dermatoporosis with contributions from dermatologists.5 This survey was administered to individuals aged ≥65 years, and 173 individuals were evaluated by a dermatologist for dermatoporosis.5 Dermatologists identified dermatoporosis in 46% of the cases.5 A survey of 533 individuals found a dermatoporosis prevalence of 37.5%.5 This study demonstrated that questionnaires can successfully detect and raise awareness of dermatoporosis; however, the presence of dermatoporosis is not defined in the clinical stage.5 In our study, we found that the majority of dermatoporosis cases, a condition already known to be highly prevalent, were at stage 1.
Researchers found that dermatoporosis was detected in 30.7% of 176 outpatients aged ≥60 years who presented to a university dermatology clinic.6 The mean age of the patients in the study was 76.6 years, and lesions were mostly located on the upper extremities (over 90%), with stage 1 being the most common (approximately 75%).6 This study found that dermatoporosis affected the upper extremities (94%), lower extremities (48%), upper trunk (23%), and facial (4%) regions.6 Furthermore, the incidence of dermatoporosis was higher in patients with bullous pemphigoid.6 This may be due to the presence of multiple comorbidities and medications, as well as the fact that patients are elderly and frail, often taking potent corticosteroids and oral steroids for an extended period.6 It was also found that patients with dermatoporosis were statistically significantly older and had a lower glomerular filtration rate.6 However, a significant association has been shown between dermatoporosis and the regular use of ultra-potent topical corticosteroids, oral steroids, concurrent corticosteroid therapy, and anticoagulant use.6
In another study, Mengeaud et al. investigated dermatoporosis in patients aged ≥60 years in geriatric settings.7 They found that the upper extremities were the most common site of dermatoporosis.7 Additionally, researchers have discovered that stage 1 (found in the forearms, legs, and hands) is the most prevalent stage.7 Stages 2 and 3 were observed with decreasing frequency, whereas stage 4 was not detected.7 In the present study, unlike in the previous one, the most common location of dermatoporosis was found to be in the upper and lower extremities in more than half of the patients. We observed that most patients had a combination of dermatoporosis rather than it being isolated to a single site, and that it also occurred on the scalp of some patients.
A retrospective study of 32 patients with deep dissecting hematomas (DDH), a manifestation of advanced dermatoporosis, showed that the most commonly affected patients were women with an average age of over 80 years.8 All patients underwent surgical debridement and were affected by the lesions.8 All but two patients were elderly and received long-term corticosteroid therapy.8 Furthermore, approximately 50% of patients were on anticoagulants.8 The clinical findings included erythema, swelling, pain, and skin necrosis.8 Unlike the literature, there was no significant difference between men and women in terms of dermatoporosis stage; however, no patient was included in stage 4, where DDH is observed. Considering that other stages can potentially progress, closer follow-up and early diagnosis, especially in women over 80 years of age who are on steroids, could reduce morbidity. Furthermore, the relatively younger average age of the patients in the present study may have impacted the lack of difference between dermatoporosis stage and sex. Additionally, there was a significant difference between dermatoporosis stages according to oral and topical steroid use, which is consistent with the literature.
A study conducted in Mexico evaluated the factors related to dermatoporosis.9 The study found that individuals over the age of 75 years with a history of severe sun exposure, use of anticoagulant medications, oral steroid use, last pregnancy at over 40 years, breastfeeding for more than seven months during pregnancy, and total breastfeeding duration of more than 18 months were at a higher risk for dermatoporosis.9 Additionally, the study reported that an age at first pregnancy under 20 years and menopause after age 45 were associated with the absence of dermatoporosis.9 The risk factors associated with this study included excessive sun exposure, oral and topical steroid use, and breastfeeding for more than 18 months. However, neither the mean age of 75 years nor the mean age at first and last pregnancies was associated with any risk factors.
One of the basic measures that can be taken to reduce dermatoporosis is to minimize sun exposure (for primary dermatoporosis) and to use topical and systemic corticosteroids carefully, considering both their benefits and risks (for secondary dermatoporosis).10
It is important to take measures to address dermatoporosis when caring for elderly patients.11 This includes educating patients and caregivers about wearing skin-protective clothing and socks, especially for tibial protection.8,11 Creating a safe living space by implementing protective measures to prevent friction or trauma from surrounding hard furniture is also crucial.11,12 Other important steps include not smoking, avoiding sunlight exposure, consuming adequate nutrition and fluids, moisturizing the skin at least twice a day, taking oral vitamin C supplements, and applying various topical products containing a combination of hyaluronic acid, retinaldehyde, epidermal growth factor, and ascorbic acid, as needed.11,13-14-15-16-17-18-19-20-21-22-23
Early diagnosis and intervention are crucial for preventing dermatoporosis progression and reducing morbidity, particularly in high-risk elderly individuals.
Limitations
One of the limitations of our study is that it was conducted at a single center and included a relatively small number of patients. Additional randomized controlled studies are necessary to gain a more comprehensive understanding of dermatoporosis.
Conclusion
Future research on dermatoporosis will be crucial in delaying the onset of advanced skin aging and increasing awareness and knowledge among healthcare professionals, including dermatologists, geriatricians, and family physicians, to better treat patients affected by this condition.
Declarations
Author Contributions (CRediT Taxonomy)
Conceptualization: D.M., L.E., H.K., S.P.K.
Methodology: D.M., L.E., H.K., S.P.K.
Formal Analysis: D.M., L.E., H.K., S.P.K.
Investigation: D.M., L.E., H.K., S.P.K.
Data Curation: D.M., L.E., H.K., S.P.K.
Writing – Original Draft Preparation: D.M.
Writing – Review & Editing: D.M., L.E., H.K., S.P.K.
Supervision: D.M., S.P.K.
Abbreviations
BMI: Body mass index
DDH: Deep dissecting hematoma
HIV: Human immunodeficiency virus
IDA: Index Dermatoporosis Assessment
References
- Kaya G, Kaya A, Sorg O, Saurat JH. Dermatoporosis, a prevalent skin condition affecting the elderly: current situation and potential treatments. Clin Dermatol. 2019;37(4):346-350. doi:10.1016/j.clindermatol.2019.04.006
- Kaya G. New therapeutic targets in dermatoporosis. J Nutr Health Aging. 2012;16(4):285-288. doi:10.1007/s12603-012-0041-0
- Bortolozo F, Rinaldi M, Souza P, Schütz Paschoal Â, Lemperle G. Dermatoporosis in upper limbs treated with polymethylmethacrylate microspheres using the BioSculpt® technique. Cureus. 2023;15(8):e43789. doi:10.7759/cureus.43789
- Kaya G, Saurat JH. Dermatoporosis: a chronic cutaneous insufficiency/fragility syndrome. Clinicopathological features, mechanisms, prevention and potential treatments. Dermatology. 2007;215(4):284-294. doi:10.1159/000107621
- Saurat JH, Mengeaud V, Georgescu V, Coutanceau C, Ezzedine K, Taïeb C. A simple self-diagnosis tool to assess the prevalence of dermatoporosis in France. J Eur Acad Dermatol Venereol. 2017;31(8):1380-1386. doi:10.1111/jdv.14240
- Kluger N, Impivaara S. Prevalence of and risk factors for dermatoporosis: a prospective observational study of dermatology outpatients in a Finnish tertiary care hospital. J Eur Acad Dermatol Venereol. 2019;33(2):447-450. doi:10.1111/jdv.15240
- Mengeaud V, Dautezac-Vieu C, Josse G, Vellas B, Schmitt AM. Prevalence of dermatoporosis in elderly French hospital in-patients: a cross-sectional study. Br J Dermatol. 2012;166(2):442-443. doi:10.1111/j.1365-2133.2011.10534.x
- Kaya G, Jacobs F, Prins C, Viero D, Kaya A, Saurat JH. Deep dissecting hematoma: an emerging severe complication of dermatoporosis. Arch Dermatol. 2008;144(10):1303-1308. doi:10.1001/archderm.144.10.1303
- Castillo-Cruz UDR, Cortés-García JD, Castanedo-Cázares JP, Hernández-Blanco D, Torres-Álvarez B. Factors associated with dermatoporosis in a sample of geriatric patients in Mexico. Gac Med Mex. 2023;159(1):49-54. doi:10.24875/GMM.M22000737
- Kaya G, Kaya A, Sorg O, Saurat JH. Dermatoporosis: a further step to recognition. J Eur Acad Dermatol Venereol. 2018;32(2):189-191. doi:10.1111/jdv.14777
- Vanzi V, Toma E. Update on dermatoporosis: what nurses need to know. J Dermatol Nurses Assoc. 2020;12(6):293-297. doi:10.1097/JDN.0000000000000578
- Vanzi V, Toma E. Recognising and managing age-related dermatoporosis and skin tears. Nurs Older People. 2018;30(3):26-31. doi:10.7748/nop.2018.e1022
- McKnight B, Seidel R, Moy R. Topical human epidermal growth factor in the treatment of senile purpura and the prevention of dermatoporosis. J Drugs Dermatol. 2015;14(10):1147-1150.
- Nikolic DS, Ziori C, Kostaki M, Fontao L, Saurat JH, Kaya G. Hyalurosome gene regulation and dose-dependent restoration of skin atrophy by retinaldehyde and defined-size hyaluronate fragments in dermatoporosis. Dermatology. 2014;229(2):110-115. doi:10.1159/000362594
- Kaya G, Tran C, Sorg O, et al. Hyaluronate fragments reverse skin atrophy by a CD44-dependent mechanism. PLoS Med. 2006;3(12):e493. doi:10.1371/journal.pmed.0030493
- Humbert P, Fanian F, Lihoreau T, Jeudy A, Pierard GE. Bateman purpura (dermatoporosis): a localized scurvy treated by topical vitamin C - double-blind randomized placebo-controlled clinical trial. J Eur Acad Dermatol Venereol. 2018;32(2):323-328. doi:10.1111/jdv.14525
- Lawton S. Maintaining skin health in older people. Nurs Older People. 2018;30(7):42-48. doi:10.7748/nop.2018.e1082
- Carville K, Leslie G, Osseiran-Moisson R, Newall N, Lewin G. The effectiveness of a twice-daily skin-moisturising regimen for reducing the incidence of skin tears. Int Wound J. 2014;11(4):446-453. doi:10.1111/iwj.12326
- Kluger N. Dermatoporosis and vitamin C deficiency. J Eur Acad Dermatol Venereol. 2018;32(10):e383. doi:10.1111/jdv.14982
- Kirkland-Kyhn H, Zaratkiewicz S, Teleten O, Young HM. Caring for aging skin. Am J Nurs. 2018;118(2):60-63. doi:10.1097/01.NAJ.0000530249.91452.4e
- Krutmann J, Bouloc A, Sore G, Bernard BA, Passeron T. The skin aging exposome. J Dermatol Sci. 2017;85(3):152-161. doi:10.1016/j.jdermsci.2016.09.015
- Wollina U. Smoking and the skin. Skinmed. 2017;15(3):197-202.
- Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. Skin anti-aging strategies. Dermatoendocrinol. 2012;4(3):308-119. doi:10.4161/derm.22804
Tables
Table 1. Stages of dermatoporosis according to topical steroid use
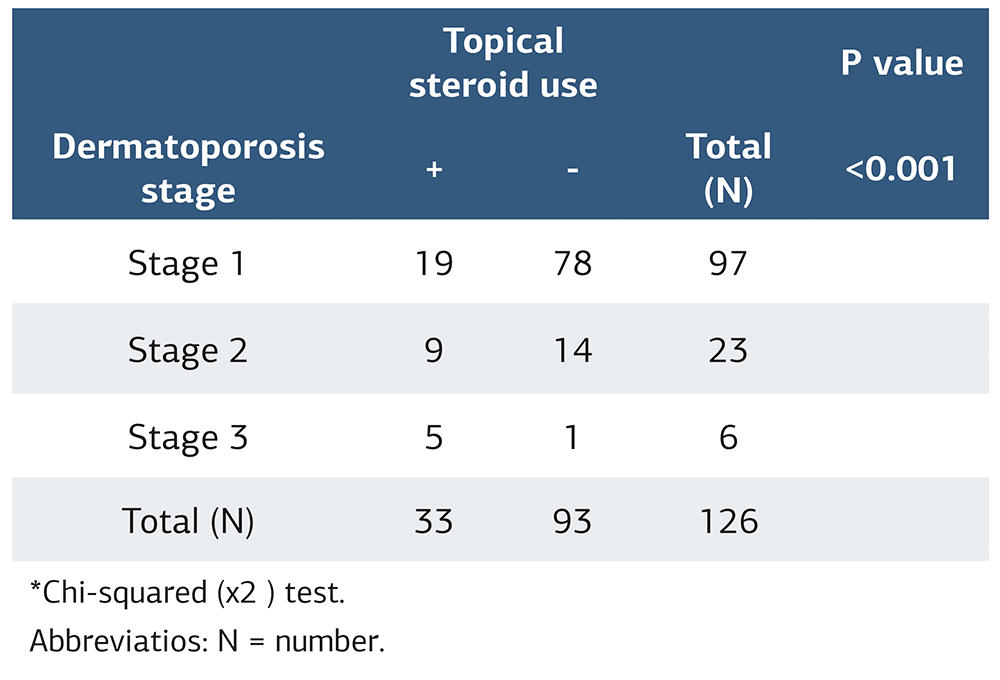
*Chi-squared (χ2 ) test. Abbreviatios: N = number.
Table 2. Stages of dermatoporosis according to oral steroid use
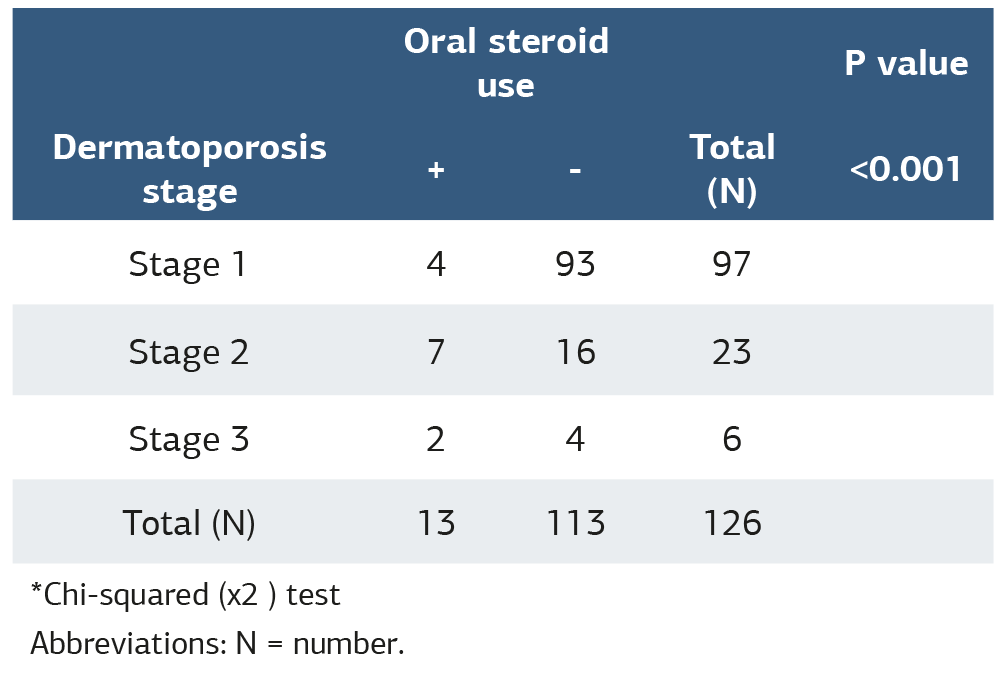
*Chi-squared (χ2 ) test Abbreviations: N = number.
Table 3. Stages of dermatoporosis according to patient sex
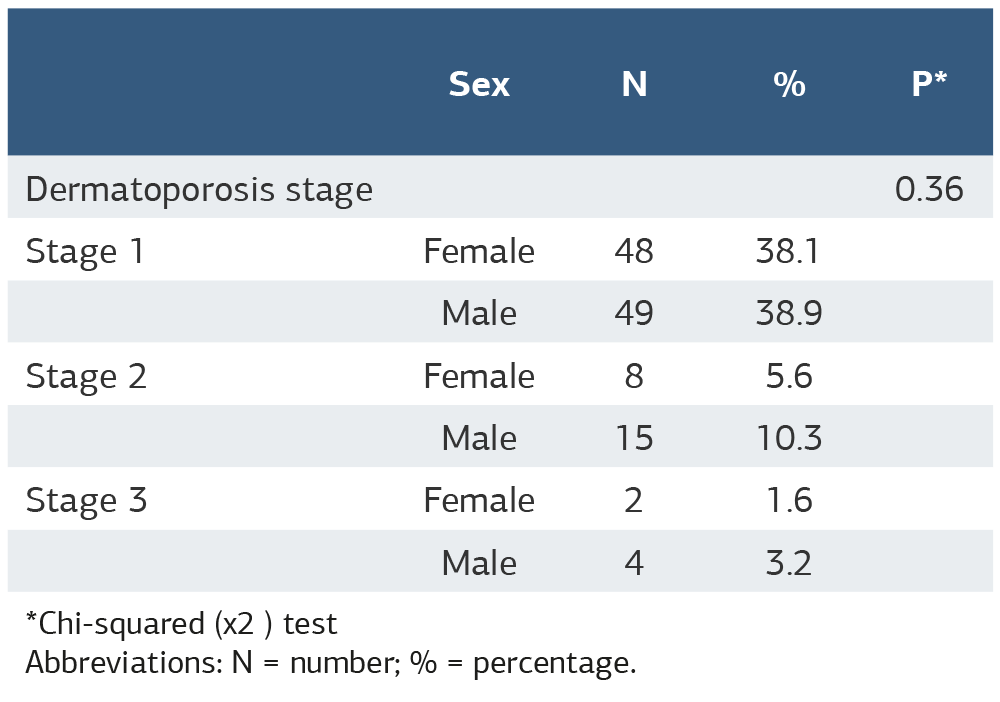
*Chi-squared (χ2 ) test Abbreviations: N = number; % = percentage.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Dilek Menteşoğlu, Laden Elkıran, Hanife Karataş, Selda Pelin Kartal. The hidden burden of dermatoporosis in elderly outpatients: evidence from a tertiary care hospital. doi:10.4328/ACAM.50064
Publication History
- Received:
- 04.02.2026
- Accepted:
- 18.03.2026
- Published Online:
- 18.03.2026
- Printed:
- 20.03.2026