
Admission serum creatinine as a predictor of renal replacement therapy in crush syndrome after the 2023 Kahramanmaraş earthquake
Admission creatinine and RRT in crush syndrome
Authors
Abstract
AimCrush syndrome–associated acute kidney injury is a major complication following earthquakes and may require renal replacement therapy (RRT). Early identification of patients at high risk for dialysis is essential in disaster settings. This study aimed to evaluate whether admission serum creatinine independently predicts RRT requirement in patients with crush syndrome following the 2023 Kahramanmaraş earthquake.
MethodsThis retrospective single-center study included adult patients admitted with crush syndrome to the nephrology department of a tertiary hospital after the February 2023 earthquake. Admission serum creatinine levels and RRT requirement during hospitalization were recorded. Univariable logistic regression analysis was performed to assess the association between admission creatinine and RRT. Receiver operating characteristic (ROC) curve analysis was used to evaluate discriminative performance.
ResultsAmong 51 eligible patients, 48 had complete data and were included in the analysis. RRT was required in 10 patients (20.8%). Admission creatinine levels were significantly higher in the RRT group compared with the non-RRT group (4.46 [2.84–6.12] vs 0.70 [0.33–2.68] mg/dL; p<0.001). Each 1 mg/dL increase in admission creatinine was associated with a 2.85-fold increase in the odds of requiring RRT (OR, 2.85; 95% CI, 2.29–3.52; p<0.001). ROC analysis demonstrated excellent discriminative performance (AUC=1.00), with an optimal cut-off value of 2.84 mg/dL.
ConclusionAdmission serum creatinine was strongly associated with RRT requirement in patients with crush syndrome after the Kahramanmaraş earthquake. Admission creatinine may serve as a simple and practical early risk indicator in disaster-related crush injuries.
Keywords
Introduction
Crush syndrome (CS) is a severe systemic condition resulting from prolonged compression of skeletal muscle, most commonly observed following earthquakes and large-scale disasters. Extensive muscle injury leads to rhabdomyolysis, which may cause acute kidney injury (AKI) through myoglobin-induced tubular toxicity, intrarenal vasoconstriction, and hypovolemia.1,2
Disaster-related crush-associated AKI remains a major contributor to morbidity and mortality. Previous earthquake cohorts have demonstrated that a considerable proportion of crush victims develop dialysis-requiring AKI, particularly in cases of prolonged entrapment and delayed rescue.3,4 The demand for renal replacement therapy (RRT) during mass casualty events presents significant logistical challenges for nephrology services, emphasizing the importance of early risk stratification.5
Following the February 2023 Kahramanmaraş earthquakes, increased incidence of crush-related AKI and substantial dialysis requirements were reported across multiple centers in Türkiye. In our previously published single-center experience, we demonstrated the high burden of renal complications and dialysis demand in earthquake victims.6 However, although the clinical spectrum of crush-related AKI has been described, data specifically focusing on early predictors of RRT requirement remain limited.
Serum creatinine at admission is a simple and widely available laboratory parameter reflecting renal function. Its independent predictive role for subsequent RRT requirement in disaster-related crush cohorts has not been sufficiently clarified in single-center nephrology populations.
Therefore, the aim of this study was to determine whether admission serum creatinine independently predicts the need for renal replacement therapy in patients with crush syndrome following the February 2023 Kahramanmaraş earthquake.
Materials and Methods
Study Design and SettingThis study was designed as a retrospective observational analysis conducted at a tertiary referral center. The study population consisted of patients admitted following the February 2023 Kahramanmaraş earthquake.
The present study represents a secondary analysis of a previously approved retrospective dataset including crush syndrome patients treated at our center.
Study PopulationAll adult patients diagnosed with crush syndrome and admitted to the nephrology department during the post-earthquake period were evaluated. Crush syndrome was defined based on clinical findings consistent with prolonged muscle compression and laboratory evidence of rhabdomyolysis.
Patients with incomplete data for admission serum creatinine or renal replacement therapy (RRT) status were excluded from regression analysis. A total of 48 patients with complete data were included in the final statistical model.
Data CollectionDemographic characteristics and laboratory parameters at admission were obtained from electronic medical records. The primary laboratory variable of interest was admission serum creatinine level.
The primary outcome of the study was the requirement for renal replacement therapy (intermittent hemodialysis).
Outcome DefinitionRenal replacement therapy (RRT) was defined as the initiation of hemodialysis during hospitalization based on standard clinical indications, including severe metabolic acidosis, refractory hyperkalemia, fluid overload, or uremic complications.
Ethical ApprovalEthical approval was obtained from the Institutional Ethics Committee of Bakirkoy Dr. Sadi Konuk Training and Research Hospital (Date: 17.04.2023, Decision No: 2023-08-06).
Statistical AnalysisContinuous variables were assessed for distribution using visual inspection and descriptive statistics. Data are presented as median (min–max) or mean ± standard deviation where appropriate.
The association between admission serum creatinine and RRT requirement was evaluated using univariable logistic regression analysis. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
The discriminative performance of admission creatinine for predicting RRT requirement was assessed using receiver operating characteristic (ROC) curve analysis. The optimal cut-off value was determined using the Youden index. The area under the ROC curve (AUC) was calculated with 95% confidence intervals.
A complete case analysis approach was applied. Statistical significance was defined as p < 0.05. All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
A total of 51 patients with crush syndrome were evaluated. Of these, 48 patients had complete data for admission serum creatinine and RRT status and were included in the regression analysis. RRT was required in 10 patients (20.8%), while 38 patients (79.2%) did not require dialysis.
Admission serum creatinine levels were significantly higher in patients requiring RRT compared to those who did not. The median admission creatinine level was 4.46 mg/dL (2.84–6.12) in the RRT-positive group and 0.70 mg/dL (0.33–2.68) in the RRT-negative group (p<0.001) (Table 1).
In univariable logistic regression analysis, admission creatinine was strongly associated with the need for RRT. Each 1 mg/dL increase in admission creatinine was associated with a 2.85-fold increase in the odds of requiring RRT (OR, 2.85; 95% CI, 2.29–3.52; p<0.001).
ROC curve analysis demonstrated excellent discriminative performance of admission serum creatinine for predicting RRT requirement, with an AUC of 1.00. The optimal cut-off value determined by the Youden index was 2.84 mg/dL (Figure 1). Although the ROC analysis demonstrated an AUC of 1.00, this result should be interpreted with caution. In small cohorts with a limited number of outcome events, statistical phenomena such as complete separation may occur, potentially leading to overestimation of discriminative performance. The relatively small sample size and limited number of RRT cases in our study may have contributed to the observed perfect discrimination. Therefore, the AUC value likely reflects the specific distribution of creatinine levels within this cohort rather than definitive universal predictive performance. External validation in larger, multicenter populations is necessary to assess the robustness and generalizability of these findings.
Patients with admission creatinine levels above 2.84 mg/dL had a markedly increased likelihood of requiring renal replacement therapy during hospitalization.
Discussion
In this single-center cohort of patients with crush syndrome following the 2023 Kahramanmaraş earthquake, admission serum creatinine was strongly associated with the requirement for RRT. Each 1 mg/dL increase in admission creatinine significantly increased the likelihood of dialysis requirement. Furthermore, admission creatinine demonstrated excellent discriminative performance for predicting RRT. These findings highlight the clinical importance of early renal function assessment in disaster-related crush injuries.
Crush syndrome-associated AKI remains one of the most serious and resource-intensive complications observed after large-scale earthquakes. Previous disaster experiences, including the Bam and Wenchuan earthquakes, have demonstrated substantial dialysis demand among crush victims, particularly in cases of prolonged entrapment and delayed rescue.7,8 In such scenarios, rapid identification of high-risk patients is essential to optimize limited dialysis capacity and improve clinical outcomes.
Although creatine kinase (CK) is widely used as a marker of rhabdomyolysis severity, its ability to predict dialysis requirement is inconsistent. CK levels may peak later during hospitalization and may not adequately reflect early renal functional impairment at presentation.9,10 In contrast, serum creatinine directly represents glomerular filtration status and may capture the cumulative effects of hypovolemia, myoglobin-mediated tubular toxicity, intrarenal vasoconstriction, and systemic inflammatory responses already present at admission.11 Therefore, admission creatinine may serve as an integrated and immediate marker of clinically significant renal injury.
Recent analyses of the 2023 Türkiye-Syria earthquakes have further emphasized the burden of crush-related AKI. Pediatric and adult cohorts from affected regions have demonstrated substantial variability in renal outcomes and dialysis requirements, underscoring the importance of early laboratory indicators in identifying severe cases.12,13 These contemporary reports reinforce the need for practical and readily available predictors that can assist clinicians during disaster response.
From a logistical perspective, disaster nephrology requires efficient triage tools. Sudden increases in dialysis demand may overwhelm institutional capacity, particularly in the early days following mass casualties. Simple and universally available laboratory parameters, such as admission creatinine, may provide critical support for early stratification and monitoring intensity decisions. Unlike complex scoring systems, creatinine measurement is inexpensive, rapidly obtainable, and widely accessible even in resource-constrained environments.
Our findings extend prior descriptive earthquake cohort analyses by focusing specifically on the predictive value of admission creatinine within a nephrology-managed population. While earlier studies have primarily described AKI incidence and overall dialysis rates, fewer have evaluated early independent predictors of RRT requirement in single-center disaster cohorts.8,9 The clear separation observed between RRT and non-RRT groups in our cohort suggests that admission creatinine may have practical prognostic utility.
Taken together, these results support the integration of admission serum creatinine into early evaluation algorithms for crush syndrome patients in disaster settings. Larger multicenter studies are warranted to validate these findings and to determine whether creatinine-based thresholds could contribute to standardized triage protocols in future mass casualty events.
Limitations
This study has several limitations. First, it was conducted at a single tertiary center, which may limit the generalizability of the findings to other institutions or disaster settings. Second, the sample size was relatively small, and the number of RRT events was limited. Although a clear association between admission creatinine and RRT requirement was observed, the discriminative performance should be interpreted cautiously in light of the cohort size. The observed perfect ROC discrimination may partly reflect the limited event number and sample size. Third, due to the retrospective design, residual confounding cannot be excluded. Only admission creatinine was evaluated in the regression model, and other potential predictors of dialysis requirement were not included in multivariable analysis because of the limited number of events. Therefore, the independent predictive role of creatinine should be confirmed in larger cohorts with comprehensive multivariable modeling.
Finally, the study represents a secondary analysis of an existing dataset, and dynamic changes in laboratory parameters during hospitalization were not evaluated. Future prospective and multicenter studies are needed to validate the optimal creatinine threshold for early risk stratification in disaster-related crush syndrome.
Conclusion
In conclusion, admission serum creatinine was strongly associated with renal replacement therapy requirement in patients with crush syndrome following the 2023 Kahramanmaraş earthquake. Admission creatinine demonstrated excellent discriminative ability for predicting dialysis need and may serve as a simple and readily available early risk indicator in disaster settings. Early identification of high-risk patients using routine laboratory parameters may contribute to improved triage strategies and optimized allocation of dialysis resources during mass casualty events.
Declarations
Ethics Declarations
The present study represents a secondary analysis of a previously approved retrospective dataset. No additional patient data were collected. The study was conducted in accordance with the Declaration of Helsinki.
Animal and Human Rights Statement
No animal experiments were performed. This study was conducted using anonymized retrospective human data in accordance with institutional and national ethical standards.
Informed Consent
Due to the retrospective design of the study and the use of anonymized patient data, the requirement for informed consent was waived by the Institutional Ethics Committee.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.E.
Methodology: A.B.D.
Investigation: G.E.
Formal analysis: G.E.
Writing - original draft: G.E.
Writing - review & editing: A.B.D.
Supervision: M.Y.
Abbreviations
AKI: acute kidney injury
AUC: area under the curve
CI: confidence interval
CK: creatine kinase
COVID-19: coronavirus disease 2019
CS: crush syndrome
OR: odds ratio
ROC: receiver operating characteristic
RRT: renal replacement therapy
STROBE: strengthening the reporting of observational studies in epidemiology
References
-
Chavez LO, Leon M, Einav S, Varon J. Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Crit Care. 2016;20(1):135. doi:10.1186/s13054-016-1314-5
-
Petejova N, Martinek A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care. 2014;18(3):224. doi:10.1186/cc13897
-
Sever MS, Vanholder R; RDRTF of ISN Work Group on Recommendations for the Management of Crush Victims in Mass Disasters. Recommendation for the management of crush victims in mass disasters. Nephrol Dial Transplant. 2012;27(Suppl 1):i1-i67. doi:10.1093/ndt/gfs156
-
Vanholder R, Sever MS, De Smet M, Erek E, Lameire N. Intervention of the Renal Disaster Relief Task Force in the 1999 Marmara, Turkey earthquake. Kidney Int. 2001;59(2):783-791. doi:10.1046/j.1523-1755.2001.059002783.x
-
Kellum JA, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders HJ. Acute kidney injury. Nat Rev Dis Primers. 2021;7(1):52. doi:10.1038/s41572-021-00284-z
-
Sezer GE, Dirim AB, Güleç E, Yılmaz M. Single Center Data of Kahramanmaraş earthquake: Bakırköy Dr. Sadi Konuk Training and Research Hospital, nephrology department experience. Med J Bakirkoy. 2024;20:1-6. doi:10.4274/BMJ.galenos.2023.2023.7-1
-
Hatamizadeh P, Najafi I, Vanholder R, et al. Epidemiologic aspects of the Bam earthquake in Iran: the nephrologic perspective. Am J Kidney Dis. 2006;47(3):428-438. doi:10.1053/j.ajkd.2005.11.019
-
Li W, Qian J, Liu X, et al. Management of severe crush injury in a front-line tent ICU after 2008 Wenchuan earthquake in China: an experience with 32 cases. Crit Care. 2009;13(6):R178. doi:10.1186/cc8160
-
Zhang L, Fu P, Wang L, et al. The clinical features and outcome of crush patients with acute kidney injury after the Wenchuan earthquake: differences between elderly and younger adults. Injury. 2012;43(9):1470-1475. doi:10.1016/j.injury.2010.11.036
-
Safari S, Yousefifard M, Hashemi B, et al. The value of serum creatine kinase in predicting the risk of rhabdomyolysis-induced acute kidney injury: a systematic review and meta-analysis. Clin Exp Nephrol. 2016;20(2):153-161. doi:10.1007/s10157-015-1204-1
-
Zager RA. Rhabdomyolysis and myohemoglobinuric acute renal failure. Kidney Int. 1996;49(2):314-326. doi:10.1038/ki.1996.48
-
Döven SS, Tezol Ö, Yeşil E, et al. The 2023 Türkiye-Syria earthquakes: analysis of pediatric victims with crush syndrome and acute kidney injury. Pediatr Nephrol. 2024;39(7):2209-2215. doi:10.1007/s00467-024-06307-7
-
Turgutalp K, Kiykim AA, Oto OA, et al. Analysis of crush syndrome patients with and without acute kidney injury during the 2023 Kahramanmaraş earthquake: experience of a tertiary referral center from Türkiye. Turk J Nephrol. 2024;33(2):161-172. doi:10.5152/turkjnephrol.2024.23639
Figures
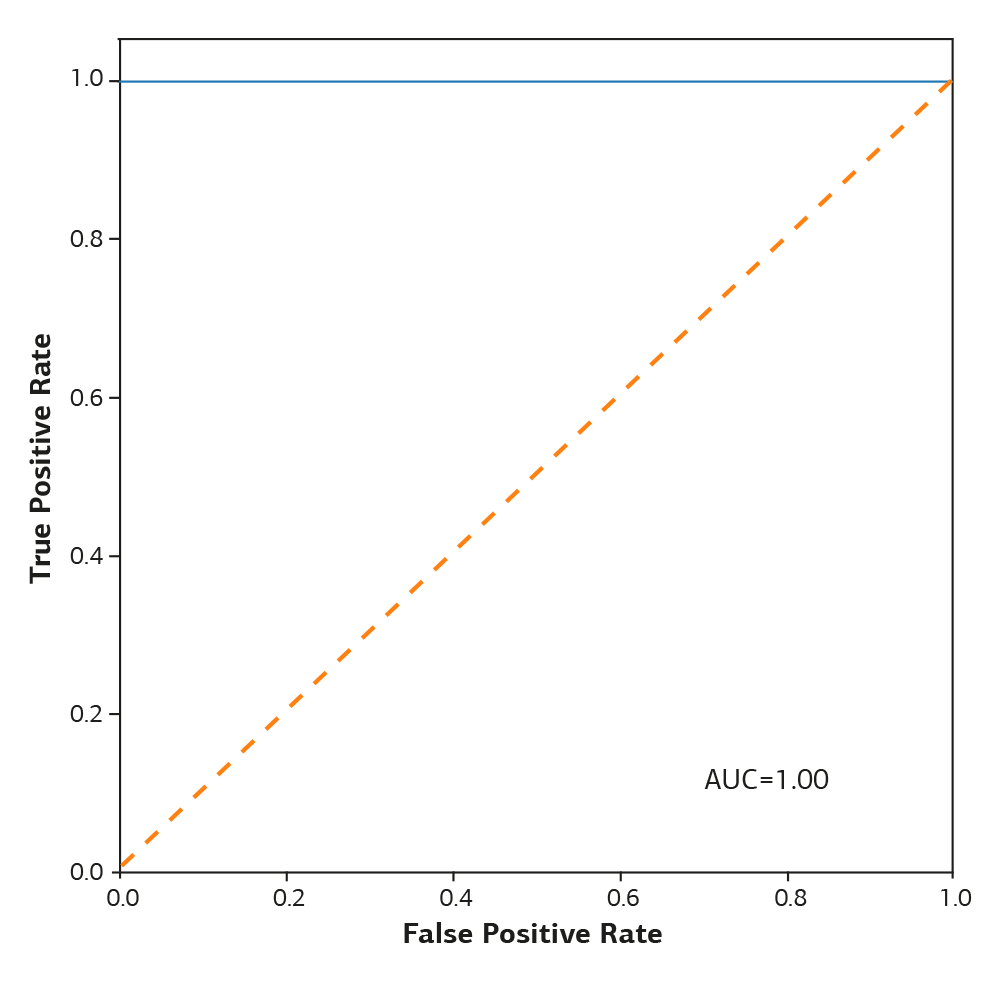
Figure 1. Receiver operating characteristic (ROC) curve showing the discriminative performance of admission serum creatitine for predicting renal replacement therapy requirement
Tables
Table 1. Admission creatinine levels according to RRT status
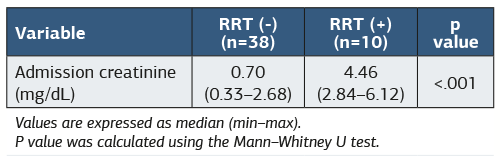
Values are expressed as median (min-max). P-value was calculated using the Mann-Whitney U test. Abbreviations: RRT = Renal replacement therapy; mg/dL = Milligrams per deciliter.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gamze Ergun, Ahmet Burak Dirim, Murvet Yilmaz. Admission serum creatinine as a predictor of renal replacement therapy in crush syndrome after the 2023 Kahramanmaraş earthquake. Ann Clin Anal Med 2026;17(5):403-406. doi:10.4328/ACAM.50107
- Received:
- March 2, 2026
- Accepted:
- April 8, 2026
- Published Online:
- April 8, 2026
- Printed:
- May 1, 2026