
Resection arthroplasty in diabetic foot patients: a paradigm shift in finger amputations and its clinical implications
Resection arthroplasty in diabetic foot patients
Authors
Abstract
AimThis study aims to investigate the clinical implications of resection arthroplasty in diabetic foot patients and assess its potential advantages over conventional methods.
MethodsA thorough literature review was conducted, encompassing clinical studies, case reports, and expert opinions on resection arthroplasty in diabetic finger amputations. Data were extracted and analyzed to determine key clinical implications and outcomes associated with this innovative surgical approach.
ResultsResection arthroplasty offers several benefits in managing diabetic finger amputations. It preserves functional digit length, enhances aesthetic outcomes, and reduces wound healing complications compared to traditional methods. Additionally, precise bone resection and joint preservation may maintain joint function and overall foot functionality, leading to improved psychological well-being and postoperative quality of life.
ConclusionThe clinical implications of resection arthroplasty extend beyond immediate surgical outcomes. Preserving finger length and function can enhance overall foot functionality, aiding patients in daily activities and preserving independence. Moreover, the psychological impact of improved foot aesthetics and function is significant. Furthermore, by reducing wound complications and hospital stays, resection arthroplasty may generate healthcare cost savings. It represents a promising shift in managing diabetic finger amputations, offering clinical advantages over traditional approaches.
Keywords
Introduction
Diabetes mellitus, a chronic metabolic disorder characterized by hyperglycemia, has become a global epidemic. Its long-term complications span from cardiovascular diseases to neuropathy and nephropathy, with diabetic foot syndrome posing a significant challenge. Among its consequences are digital ischemia and necrosis, often leading to necessary surgical interventions like finger amputations.
Historically, traditional surgical approaches focused on infection control but often resulted in significant tissue loss and functional limitations for patients.1,2 However, a paradigm shift has occurred with the emergence of resection arthroplasty, a technique aiming to preserve both digit length and function by meticulously removing affected bone and joint structures and reconstructing the finger.
This innovative approach offers potential advantages over conventional methods, including improved functional and aesthetic outcomes.3 Through a systematic literature review, this study aims to explore the multifaceted implications of resection arthroplasty, addressing questions about its effectiveness, impact on quality of life, and economic implications.4
By delving into the clinical, functional, psychological, and economic dimensions of resection arthroplasty, this research seeks to contribute to a deeper understanding of its benefits and empower healthcare providers and patients in decision-making regarding diabetic finger amputations.
Materials and Methods
This study employed a retrospective analysis of clinical cases and a comprehensive literature review to investigate the clinical implications of resection arthroplasty in the context of diabetic finger amputations. Patient data from the Diabetic Foot Surgery Clinic at Hitit University Research Hospital underwent retrospective scrutiny, focusing on demographic characteristics, diabetic status, preoperative evaluations, surgical particulars, and postoperative follow-up details. Inclusion criteria encompassed diabetic patients who underwent finger amputation with resection arthroplasty as the primary intervention, provided their medical records were complete and follow-up information was sufficient. Conversely, exclusion criteria entailed cases with incomplete data, alternative surgical methods, or contraindications for resection arthroplasty.
A systematic review of literature from 2020 to 2023 was conducted to identify pertinent articles from electronic databases and academic journals. The surgical procedure was characterized by meticulous bone resection, joint preservation, and tendon realignment, aimed at optimizing postoperative outcomes. Short-term metrics, including wound healing and pain management, as well as long-term indicators such as preservation of finger length and functional recovery, were scrutinized. Furthermore, specific complications relevant to diabetic patients were examined, along with strategies for their mitigation. Through this integrative approach, the study sought to furnish comprehensive insights into the efficacy and challenges associated with resection arthroplasty in managing diabetic finger amputations.
Ethical ApprovalThis study was approved by the Ethics Committee of Hitit University (Date: 03.04.2024, Decision No: 2024-0116).
Statistical AnalysisNo formal statistical analysis was performed; data were evaluated descriptively.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Resection arthroplasty, heralded as a transformative surgical intervention, marks a departure from conventional techniques in the realm of finger amputations, particularly pertinent in the context of diabetic foot patients,5 This innovative procedure intricately involves the precise excision of diseased bone and joint structures while concurrently safeguarding finger length and functionality to an exceptional extent.2 Its emergence has captured considerable attention for its potential to redefine the treatment landscape for finger amputations, presenting a paradigmatic shift in addressing the complexities inherent in managing diabetic foot complications. This exposition undertakes a comprehensive exploration of resection arthroplasty, elucidating its procedural intricacies and the profound transformative impact it imparts upon the lives of patients.6
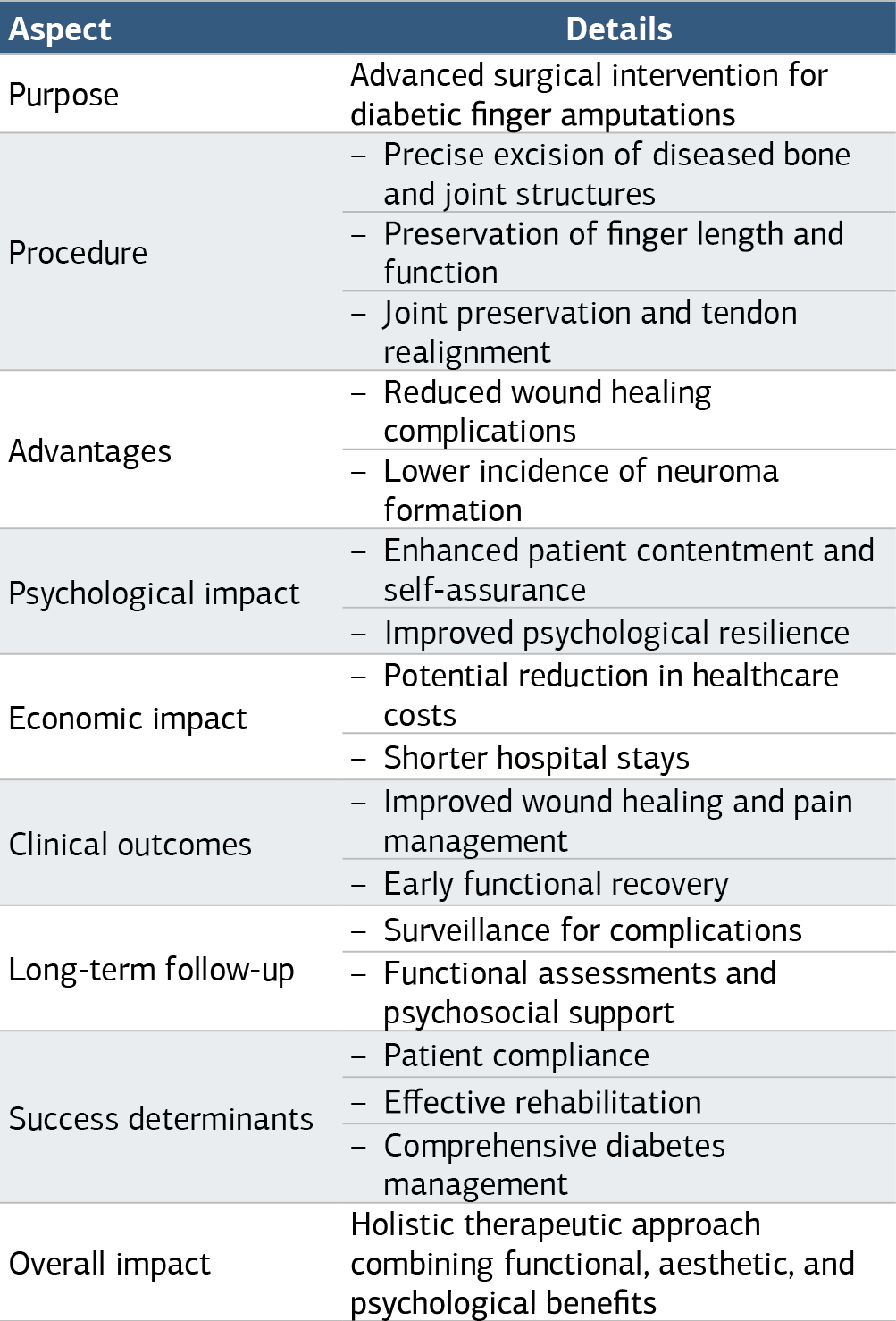
Resection arthroplasty, positioned as a cornerstone in the surgical armamentarium for diabetic finger amputations, is distinguished by its methodical approach encompassing precise bone resection, joint preservation, and tendon realignment. These meticulous maneuvers are aimed at excising pathological tissue while preserving essential anatomical structures and optimizing functional outcomes.7 The preservation of finger length constitutes a pivotal aspect. Notably, resection arthroplasty confers advantages over conventional techniques, notably in mitigating wound healing complications and neuroma formation, thereby facilitating a smoother postoperative course.
Psychologically, the preservation of finger length and aesthetics engenders a sense of contentment and self-assurance among patients, augmenting their overall well-being and psychological resilience (Table 1). Furthermore, the economic ramifications of resection arthroplasty cannot be understated, with its potential to curtail healthcare costs stemming from complications and protracted hospital stays. Thus, resection arthroplasty emerges as a holistic therapeutic modality, addressing multifaceted dimensions encompassing functional rehabilitation, aesthetic restoration, psychological well-being, and healthcare resource optimization.
Assessment of clinical outcomes and long-term follow-up serves as a linchpin in evaluating the efficacy and durability of resection arthroplasty in the context of diabetic finger amputations.8 Short-term outcomes, including wound healing, pain management, and early functional recovery, underscore the immediate benefits conferred by this technique, underscored by minimized tissue trauma and optimized wound healing.9 Furthermore, the perpetuation of finger length and aesthetics bears tangible psychological dividends, fostering a positive outlook and reinforcing patient satisfaction.
In the continuum of care, sustained success hinges upon meticulous long-term follow-up, encompassing vigilant surveillance for complications, ongoing functional assessments, and psychosocial support. Key determinants of enduring success encompass patient compliance, rehabilitation initiatives, and judicious diabetes management strategies, epitomizing the imperative for comprehensive care extending beyond the immediate perioperative period. Thus, amidst the evolving landscape of diabetic finger amputations, resection arthroplasty emerges as a beacon of hope, embodying a paradigmatic shift towards patient-centered, evidence-based therapeutic approaches.
Discussion
The discussion section critically evaluates the study’s findings on resection arthroplasty for diabetic finger amputations. It underscores the significance of this novel surgical approach in addressing the complex needs of diabetic patients with finger complications. Comparative analyses with existing literature illuminate how resection arthroplasty aligns with or diverges from established practices, contributing to the broader understanding of surgical interventions for diabetic foot care. Lastly, avenues for future research are outlined, including prospective studies with larger cohorts and investigations into economic impact and cost-effectiveness. Overall, the discussion section serves to interpret the study’s findings, contextualize them within the existing body of knowledge, and delineate directions for further research, thus advancing the field of diabetic foot care and surgical management.
Limitations
Methodological limitations, such as sample size and follow-up duration, are acknowledged, providing transparency and context to the study’s scope.
Conclusion
The clinical implications of the study’s findings are emphasized, particularly in terms of patient satisfaction, quality of life improvements, and healthcare resource utilization.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
DM: Diabetes mellitus
RA: Resection arthroplasty
References
-
Boileau P, Raynier J, Chelli M, Gonzalez J. Reverse shoulder-allograft prosthesis composite, with or without tendon transfer, for the treatment of severe proximal humeral bone loss. J Shoulder Elbow Surg. 2020;29(11):e401-e415. doi:10.1016/j.jse.2020.03.016
-
Malhotra V, Singh V, Rao J, et al. Lateral arthroplasty along with buccal fat pad interpositioning in the management of Sawhney type III temporomandibular joint ankylosis. J Korean Assoc Oral Maxillofac Surg. 2019;45(3):129-135. doi:10.5125/jkaoms.2019.45.3.129
-
Scimeca C, Bharara M, Fisher T, Kimbriel H. Novel use of platelet-rich plasma to augment curative diabetic foot surgery. J Diabetes Sci Technol. 2010;4(5):1121-1126. doi:10.1177/193229681000400510
-
Pontes J, Ferreira-Pinto P, Martha B, Silva W, Senior M. Resection arthroplasty for isolated costotransverse joint osteoarthritis: a case report and literature review. Surg Neurol Int. 2022;13:62. doi:10.25259/sni_88_2022
-
Cooney W, Manuel J, Froelich J, Rizzo M. Total wrist replacement: a retrospective comparative study. J Wrist Surg. 2012;1(2):165-172. doi:10.1055/s-0032-1326728
-
Chaudhary M, Walker P. Analysis of an early intervention tibial component for medial osteoarthritis. J Biomech Eng. 2014;136(6):061008. doi:10.1115/1.4027467
-
Brooks F, Hariharan K. The rheumatoid forefoot. Curr Rev Musculoskelet Med. 2013;6(4):320-327. doi:10.1007/s12178-013-9178-7
-
Kang H, Chung S. Resection arthroplasty in radiation-induced osteonecrosis of the hip. J Clin Orthop Trauma. 2019;10(2):364-367. doi:10.1016/j.jcot.2018.02.016
-
Periasamy M, Muthukumar V, Reddy R, Asokan K. Outcomes of Keller gap arthroplasty for plantar hallux interphalangeal joint ulcers in patients with diabetes mellitus. Foot Ankle Int. 2023;44(3):192-199. doi:10.1177/10711007231152883
Tables
Table 1. Key points of resection arthroplasty in diabetic finger amputations
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İsmail Sezikli, Kaan Canal, Taner Alic, Murat Kendirci. Resection arthroplasty in diabetic foot patients: a paradigm shift in finger amputations and its clinical implications. Ann Clin Anal Med 2025;16(2):82-85. doi:10.4328/ACAM.22260
- Received:
- May 13, 2024
- Accepted:
- October 21, 2024
- Published Online:
- November 6, 2024
- Printed:
- February 1, 2025