
Could corneal densitometry be a diagnostic criterion for keratoconus?
Corneal densitometry and diagnosis in keratoconus
Authors
Abstract
AimTo examine corneal densitometry measurements with the Pentacam Scheimpflug imaging system in keratoconus patients and compare them with a healthy control group.
MethodsThe study included 112 eyes of 112 keratoconus patients followed up in the cornea clinic and 246 eyes of age-matched 246 healthy individuals. In all cases, K1, K2, K Max, central corneal thickness, thinnest corneal thickness, anterior elevation, posterior elevation, and corneal densitometry values were measured using the Scheimpflug imaging system. Corneal densitometry was evaluated based on four concentric radial zones (0-2 mm, 2-6 mm, 6-10 mm, and 10-12 mm) and by depth (anterior, central, posterior, and total). Keratoconus patients were divided into four stages. Corneal densitometry values were compared between each stage and the healthy control group. The results were statistically analyzed.
ResultsThe average age between the groups did not show any statistically significant difference (p>0.05). Corneal densitometry values were found to be statistically significantly higher in keratoconus patients compared to the healthy control group in all zones and layers, except for the 10-12 mm zone (p<0.01). Nevertheless, no statistically significant differences were observed in corneal densitometry values across the various stages of keratoconus (p>0.05).
ConclusionScheimpflug topography combined with corneal densitometry measurement is a non-invasive examination method that provides information about corneal transparency. Changes in corneal histology in keratoconus patients may influence densitometry values. According to our study, the higher corneal densitometry values observed in keratoconus patients compared to the healthy group may provide supportive evidence for the diagnosis of keratoconus, in addition to other criteria used for diagnosis.
Keywords
Introduction
Keratoconus is an advancing ectatic condition of the cornea, marked by gradual thinning and out-ward bulging, resulting in irregular astigmatism and diminished visual acuity.1,2 Despite nu-merous pathological changes observed in the histopathology of keratoconus, the exact pathogene-sis of the disease remains incompletely understood.3 Several studies have reported ultrastruc-tural alterations in keratoconus, including the loss of stromal collagen lamellae, changes in colla-gen fibril orientation, and a notable decrease in keratocyte density, especially in the anterior cen-tral region.4,5,6,7
Pentacam® HR Scheimpflug tomography (Oculus, Inc., Wetzlar, Germany) is an objective and non-invasive method that assists in detecting changes in curvature and elevation of both the ante-rior and posterior corneal surfaces. Additionally, it measures corneal transparency by quantifying the intensity of light scattered back from the cornea.8 This study aims to evaluate corneal densitometry in previously untreated keratoconus patients, compare these results with those of healthy individuals, and assess whether there are differences in densitometry among different stages of keratoconus.
Materials and Methods
This retrospective observational study was conducted by the cornea unit of the Ankara Bilkent City Hospital Ophthalmology Clinic. Patients diagnosed with keratoconus who had not received treatment and who presented to our clinic between March 2021 and March 2023 were retrospec-tively screened. The study included 112 eyes of 112 keratoconus patients and 246 eyes of 246 age-matched healthy individuals. The healthy control group was made up of individuals who came to our clinic for soft contact lens fitting and were confirmed to be free of ectasia. Keratoconus pa-tients were categorized into four stages. Corneal densitometry values were compared between each stage and the healthy control group. Patients with a history of ocular trauma and surgery, contact lens use, significant corneal opacity, glaucoma, uveitis, lack of compliance/cooperation, diabetes mellitus, hypertension, or systemic rheumatologic diseases were excluded from the study. Both groups underwent a comprehensive ophthalmological examination, including an assessment of best-corrected visual acuity using Snellen charts, anterior and posterior segment biomicroscop-ic examination, and measurement of various parameters using the Scheimpflug imaging system (Pentacam HR, Oculus, Germany). The measured parameters included K1, K2, K Max, central corneal thickness, thinnest corneal thickness, anterior elevation, posterior elevation, and corneal densitometry values. Intraocular pressure (IOP) measurements were also taken using a Goldmann application tonometer. Scheimpflug imaging was performed in the morning hours, in the same dark room, and by the same individual (CC).
For corneal densitometry analysis, the Pentacam® Scheimpflug imaging system, equipped with software add-ons, was used to measure the amount of scattered light.
The measurements were conducted three times, and only those with a “quality specification = OK” reading were considered for inclusion in this study. This system is capable of measuring corneal densitometry in a 12 mm diameter area, with the central corneal apex being the reference point in four radial regions and three different depths. The first region consisted of a circular area with a 2 mm diameter at the center of the cornea. The second region was a ring-shaped area around the first region, ranging from 2 to 6 mm in diameter. The third region encompassed an area from 6 to 10 mm in diameter, and the fourth region covered a ring-shaped area from 10 to 12 mm in diame-ter. Based on depth, three different layers were defined: the most anterior 120 µm as the anterior layer, the most posterior 60 µm as the posterior layer, and the region between these two layers as the central layer. Densitometry results were expressed in units of grayscale, with maximum light scattering assigned a value of 100 (indicating minimum transparency, a fully opaque cornea) and minimum light scattering assigned a value of 0 (indicating maximum transparency). The values could vary between 0 and 100.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Bilkent City Hospital (Date: 07.06.2023, Decision No: E1-23-3673).
Statistical AnalysisAll data were analyzed using the IBM SPSS Statistics 21.0 software. Continuous variables were summarized as mean ± SD or median (min-max), and categorical variables were reported as frequencies and percentages. Pearson’s correlation test was employed for correlation analysis, and for comparing groups, the Mann-Whitney U test and Wilcoxon W test were used. A p-value of less than 0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
The study included a total of 358 eyes from 358 individuals, comprising 112 eyes of 112 kerato-conus patients who had not received prior treatment and 246 eyes of 246 healthy individuals. The mean age of the keratoconus patients was 27.49 ± 8.21 years, while that of the healthy controls was 26.3 ± 7.22 years. There was no statistically significant difference in mean age between the two groups (p=0.192). According to the Amsler–Krumeich classification, 35 (31.25%) keratoconus patients were classified as stage 1, 36 (32.14%) as stage 2, 32 (28.57%) as stage 3, and 9 (8.03%) as stage 4. Detailed anterior segment parameters for both keratoconus patients and healthy con-trols are presented in Table 1.
Significant differences in corneal densitometry were observed between keratoconus patients and healthy controls in the 0-2 mm, 2-6 mm, and 6-10 mm annular regions (p<0.01). However, there was no significant difference in corneal densitometry values in the peripheral 10-12 mm zone be-tween the two groups (p>0.05). The corneal densitometry measurements for keratoconus patients and healthy controls are presented in Table 2.
There were no statistically significant differences in corneal densitometry values among different stages of keratoconus (p>0.05). The detailed comparison of corneal densitometry measurements between keratoconus stages and healthy controls is shown in Table 3.
Discussion
Corneal densitometry is an objective measurement that evaluates the amount of light reflected from various areas of the cornea.9 Even though the cornea may appear transparent during slit-lamp examination, light can still scatter back from the cornea. Therefore, corneal densitometry can serve as an indicator and an objective tool for measuring mild corneal edema. The total corne-al densitometry measured with Scheimpflug corneal topography represents the sum of epithelial, stromal, and endothelial light scattering.10 For corneal transparency, collagen fibrils should have a small diameter, be arranged perpendicularly, and exhibit regular spacing, while keratocyte distribution should align with this arrangement.11 The corneal epithelial cell layer and corneal endothelium are the main sources of light scattering. In contrast, the corneal stroma causes less light scattering due to the regular arrangement of collagen fibrils and the precise organization of the extracellular matrix.10
Studies, both in vivo and in vitro, have demonstrated that structural disruption in the corneal stroma is most pronounced in the anterior and central corneal stroma in keratoconus and that all corneal layers except the endothelium are affected.4,12,13,14
We believe that structural changes in the cornea may lead to an increase in corneal densitometry, and therefore, densitometric analysis can be utilized in the diagnosis of keratoconus. In our study, we observed that corneal densitometry values were higher in keratoconus patients compared to a healthy control group, except for the 10-12 mm zone, across all zones and layers. In a study evalu-ating the histopathology of the cornea, it has been reported that the anterior cornea is affected in the early stages of keratoconus and that the first changes leading to thinning and disappearance of the epithelial layer, along with breaks in the basal epithelial cell layer, Bowman’s layer, and thick-ening of the sub-basal nerve plexus, are observed.4 In a study by Koç et al., corneal densitome-try measurements were found to increase in adult subclinical keratoconus patients, suggesting that these measurements could be a useful tool for early diagnosis of corneal densitometry.15
In two separate studies, it was demonstrated that corneal densitometry values in the central 0-2 mm and 2-6 mm zones increased in keratoconus patients compared to healthy controls, suggesting that corneal densitometry can serve as a prognostic determinant of the disease.16,17 In our study, unlike these previous studies, we did not observe any differences in corneal densitometry among different stages of keratoconus. Therefore, we do not believe that corneal densitometry indicates the prognosis of the disease. We suggest that additional research with a larger patient population is required to provide further clarity on this issue.
Statistically significant differences in peripheral cornea were not found between the two groups. This may be attributed to the possibility that the pathology of the peripheral cornea is not affected in keratoconus.18 Additionally, it should be noted that peripheral corneal densitometry meas-urements are known to have the weakest repeatability and reproducibility, which could explain the lack of differences observed between the two groups.9
Limitations
Our study has a limitation. Because it was conducted with a relatively small number of patients, the number of patients in each stage is limited, which can potentially affect the densitometric measurements between stages.
Conclusion
Our study demonstrates that corneal densitometry values are significantly higher in all areas of the cornea, except for the anterior 10-12 mm zone, in previously untreated keratoconus patients when compared to healthy controls. We believe that corneal densitometric measurements can be used as an independent method for the diagnosis of keratoconus, irrespective of topographic measurements. The lack of differences in densitometry values among different stages of kerato-conus suggests that corneal densitometry measurements may not serve as a prognostic indicator in keratoconus. Additional research with larger sample sizes is necessary to validate these findings.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
IOP: Intraocular pressure
K1: Flat keratometry
K2: Steep keratometry
Kmax: Maximum keratometry
SD: Standard deviation
References
-
Davidson AE, Hayes S, Hardcastle AJ, Tuft SJ. The pathogenesis of keratoconus. Eye (Lond). 2014;28:189-195. doi:10.1038/eye.2013.278
-
Vazirani J, Basu S. Keratoconus: current perspectives. Clin Ophthalmol. 2013;7:2019-2030. doi:10.2147/opth.s50119
-
Meek KM, Tuft SJ, Huang Y, et al. Changes in collagen orientation and distribution in keratoconus corneas. Invest Ophthalmol Vis Sci. 2005;46:1948-1956. doi:10.1167/iovs.04-1253
-
Mathew JH, Goosey JD, Bergmanson JPG. Quantified histopathology of the keratoconic cornea. Optom Vis Sci. 2011;88:988-997. doi:10.1097/opx.0b013e31821ffbd4
-
Kaldawy RM, Wagner J, Ching S, Seigel GM. Evidence of apoptotic cell death in keratoconus. Cornea. 2002;21(2):206-209. doi:10.1097/00003226-200203000-00017
-
Sherwin T, Brookes NH. Morphological changes in keratoconus: pathology or pathogenesis. Clin Exp Ophthalmol. 2004;32:211-217. doi:10.1111/j.1442-9071.2004.00805.x
-
Sykakis E, Carley F, Irion L, Denton J, Hillarby MC. An in-depth analysis of histopathological characteristics found in keratoconus. Pathology. 2012;44:234-239. doi:10.1097/pat.0b013e3283511b42
-
Bühren J. Hornhauttopografie und Keratokonusdiagnostik mittels Scheimpflug-Fotografie [Corneal topography and keratoconus diagnostics with Scheimpflug photography]. Ophthalmologe. 2014;111(4):920-926. doi:10.1007/s00347-013-2962-3
-
Ní Dhubhghaill S, Rozema JJ, Jongenelen S, Hidalgo IR, Zakaria N, Tassignon MJ. Normative values for corneal densitometry analysis by Scheimpflug optical assessment. Invest Ophthalmol Vis Sci. 2014;55:162-168. doi:10.1167/iovs.13-13236
-
Otri AM, Fares U, Al-Aqaba MA, Dua HS. Corneal densitometry as an indicator of corneal health. Ophthalmology. 2012;119(3):501-508. doi:10.1016/j.ophtha.2011.08.024
-
Meek KM, Knupp C. Corneal structure and transparency. Prog Retin Eye Res. 2015;49:1-16. doi:10.1016/j.preteyeres.2015.07.001
-
Mathew JH, Goosey JD, Söderberg PG, Bergmanson JPG. Lamellar changes in the keratoconic cornea. Acta Ophthalmol. 2015;93:767-773. doi:10.1111/aos.12811
-
Mercatelli R, Ratto F, Rossi F, Tatini F, Menabuoni L, Malandrini A. Three-dimensional mapping of the orientation of collagen corneal lamellae in healthy and keratoconic human corneas using SHG microscopy. J Biophotonics. 2016;10:75-81.
-
Khaled ML, Helwa I, Drewry M, Seremwe M, Estes A, Liu Y. Molecular and histopathological changes associated with keratoconus. Biomed Res Int. 2017;2017:7803029. doi:10.1155/2017/7803029
-
Koc M, Tekin K, Tekin MI, et al. An early finding of keratoconus: increase in corneal densitometry. Cornea. 2018;37(5):580-586. doi:10.1097/ico.0000000000001537
-
Anayol MA, Sekeroglu MA, Ceran BB, Dogan M, Gunaydin S, Yilmazbas P. Quantitative assessment of corneal clarity in keratoconus: a case-control study of corneal densitometry. Eur J Ophthalmol. 2016;26(1):18-23. doi:10.5301/ejo.5000644
-
Lopes B, Ramos I, Ambrósio R Jr. Corneal densitometry in keratoconus. Cornea. 2014;33(12):1282-1286. doi:10.1097/ico.0000000000000266
-
Ucakhan OO, Kanpolat A, Yılmaz N, Ozkan M. In vivo confocal microscopy findings in keratoconus. Eye Contact Lens. 2006;32(4):183-191.
Tables
Table 1. Anterior segment parameters for both keratoconus patients and healthy controls (Mean ± SD)
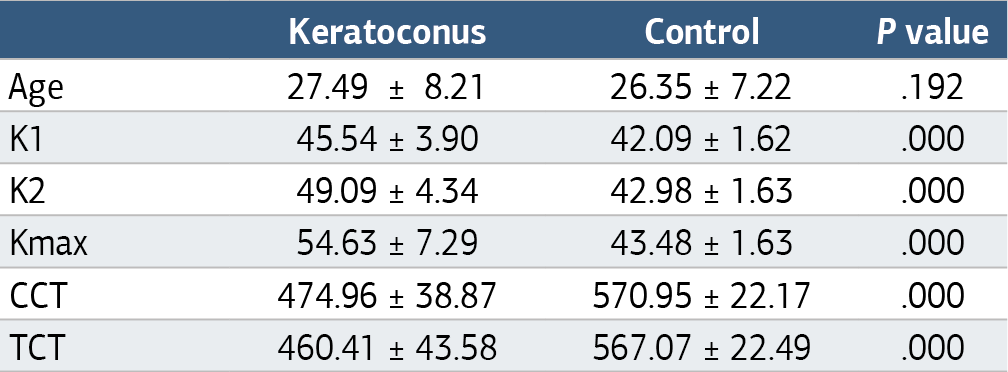
K1: flat keratometry K2: steep keratometry Kmax: maximum keratometry CCT: central corneal thickness TCT: thinnest corneal thickness.
Table 2. The corneal densitometry measurements for keratoconus patients and healthy controls (Mean ± SD)
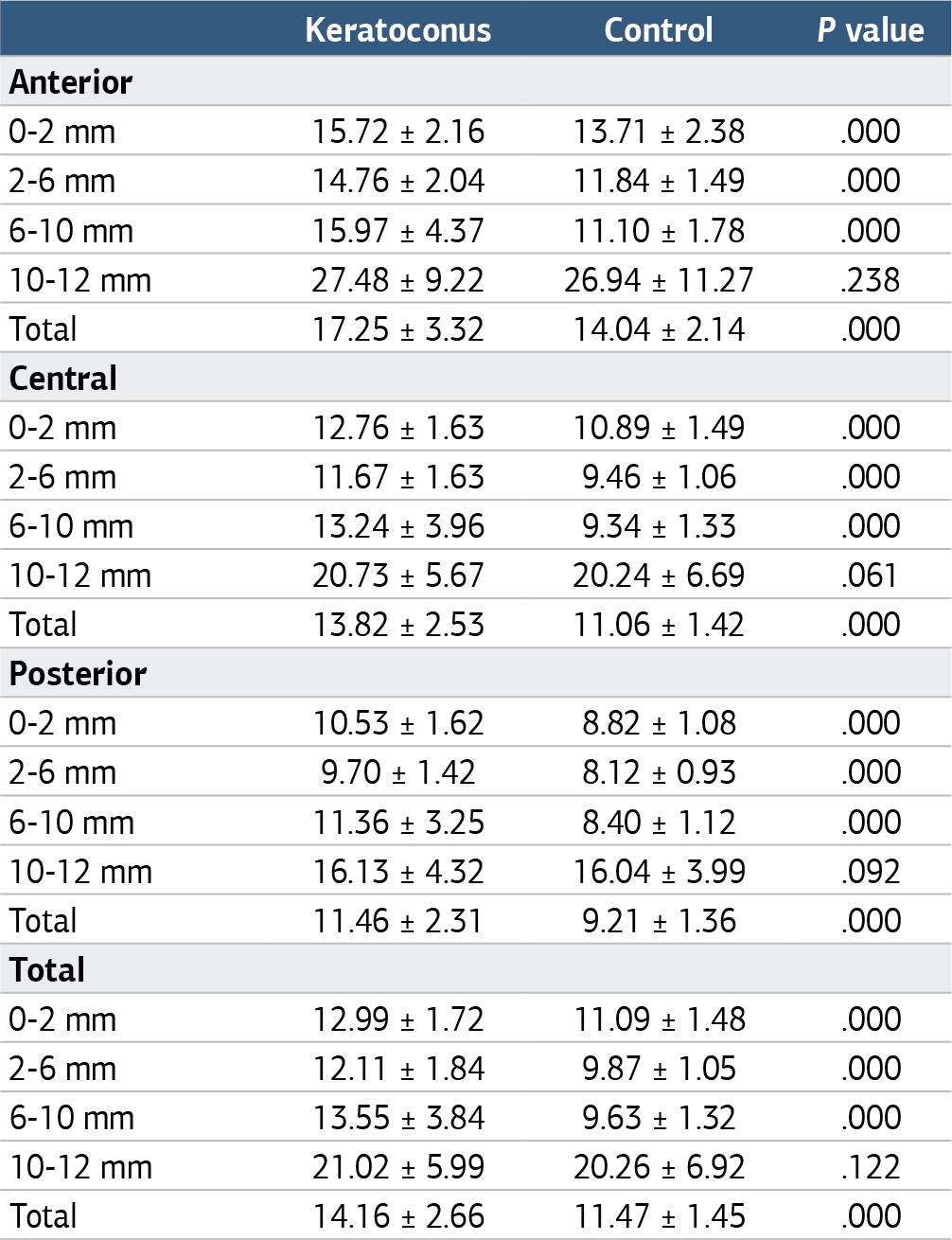
Table 3. Corneal densitometry measurements between keratoconus stages and healthy controls (Mean ± SD)

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Cigdem Coskun, Sebile Çomçalı. Could corneal densitometry be a diagnostic criterion for keratoconus? Ann Clin Anal Med 2025;16(2):118-121. doi:10.4328/ACAM.22400
- Received:
- September 13, 2024
- Accepted:
- October 21, 2024
- Published Online:
- November 7, 2024
- Printed:
- February 1, 2025