
Follow-up of recurrent suicide attempts of patients admitted to the emergency department
Follow-up of suicide attempts
Authors
Abstract
AimThis study aimed to evaluate outpatient psychiatric follow-up among patients presenting to the emergency department (ED) with a suicide attempt (SA) and to identify factors associated with follow-up adherence and recurrence.
MethodsThis retrospective study included patients aged ≥18 years who presented to the ED of a tertiary hospital with SA between May 2023 and May 2024. Data were obtained from hospital records and telephone follow-up. Sociodemographic and clinical characteristics, psychiatric consultations, and follow-up adherence were analyzed.
ResultsA total of 329 patients were included. Psychiatric consultation was not performed in 49.2% of cases. Outpatient follow-up was recommended for 36.8% of patients, of whom 49.6% did not attend any follow-up visits. Previous psychiatric diagnosis, prior SA, and receiving a psychiatric diagnosis during ED evaluation were significantly associated with follow-up adherence (p<0.05). Fourteen patients (4.3%) had a recurrent SA within one year. Previous SA was the only significant predictor of recurrence (OR = 1.643, p = 0.017). Medication overdose was the most common method, while high-lethality methods were more frequent in recurrent cases.
ConclusionsA substantial proportion of patients presenting with SA do not receive psychiatric consultation or adhere to follow-up recommendations. Previous SA is the strongest predictor of recurrence. Improving psychiatric assessment in the ED and strengthening continuity of care may enhance follow-up adherence and contribute to suicide prevention.
Keywords
Introduction
According to the World Health Organization, approximately 800,000 people die each year due to suicide, corresponding to one death every 40 seconds. Suicide attempts are estimated to occur 10–30 times more frequently; however, inadequate records may lead to underestimation.1 Suicide risk and prevention remain major research areas.2 The etiology of suicide attempts involves complex interactions of social, psychological, and biological factors, and up to 98% of individuals who die by suicide have a diagnosable mental disorder, most commonly depression and substance use disorders.3
Risk factors include young age, unemployment, social isolation, prior attempts, untreated psychiatric illness, and lack of support, while internal drivers such as hopelessness and psychological pain are also important.4 Several tools have been developed to assess suicidal behavior.5
Many individuals who attempt suicide present to emergency departments (EDs), where rapid assessment is required.6 However, time constraints and limited conditions may hinder comprehensive psychiatric evaluation and continuity of care.7,8 Adherence to outpatient follow-up after ED discharge remains insufficiently studied.
This study aimed to evaluate adherence to outpatient follow-up among patients presenting to the ED with suicide attempts and its association with recurrent suicide attempts.
This study sought to address the following research questions:
1. What proportion of patients presenting to the ED with a suicide attempt (SA) attended the recommended outpatient psychiatric follow-up, and to what extent was follow-up completed within one year?
2. Which sociodemographic and clinical characteristics were identified during the ED evaluation, and were associated with engagement in outpatient psychiatric follow-up?
3. What were the psychiatric diagnoses and consultation characteristics of patients presenting to the ED following a SA?
4. Which emergency department–level and follow-up-related factors were associated with recurrent suicide attempts during the follow-up period?
Materials and Methods
Study Population and Data SourcesThis retrospective descriptive study included patients aged ≥18 years who presented to the emergency department of Alanya Alaaddin Keykubat University Alanya Education and Research Hospital following a suicide attempt between 1 May 2023 and 1 May 2024.
Patients recorded as forensic cases due to suicide attempts were identified using the International Classification of Diseases 10 (ICD-10) codes (X60–X84) and the institutional suicide attempt code (009). Suicide attempts were defined as intentional self-harm with suicidal intent, including methods such as medication overdose, self-inflicted injury, chemical ingestion, excessive alcohol intake, jumping from height, hanging, or firearm injury.
Adherence to outpatient psychiatric follow-up was evaluated using hospital electronic records and telephone interviews. The study was conducted in the only public hospital in XXX, XXX, that provides inpatient psychiatric services and receives suicide cases from the district. Patients under 18 years of age and those with incomplete records were excluded. Due to the retrospective design, some sociodemographic variables (e.g., marital status, number of children, and education) were unavailable.
Ethical ApprovalThe study was approved by the Ethics Committee of Alanya Alaaddin Keykubat University Alanya Education and Research Hospital (Date: 21.08.2024, Decision No: 19-08).
Statistical AnalysisData were analyzed using IBM SPSS Statistics for Windows version 29.0 (IBM Corp., Armonk, NY). Categorical variables were presented as frequencies and percentages, and continuous variables as means ± standard deviations. The Mann–Whitney U test and Pearson’s chi-square test were used for group comparisons, including analyses of recurrent suicide attempts. Multivariate logistic regression analysis was performed to examine factors associated with outpatient psychiatric follow-up and recurrent suicide attempts. A p-value < 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Sociodemographic and Clinical CharacteristicsA total of 329 patients were included (mean age: 33.76 ± 12.62 years; 57.8% female). Approximately half had a prior psychiatric diagnosis (50.2%), and 21.6% had a history of suicide attempts. Nearly half of the patients were not evaluated by a psychiatrist in the emergency department, and a substantial proportion left before completing the assessment. Details are presented in Supplementary Table 1.
Suicide Attempt MethodsMedication overdose was the most common method (79.6%), followed by chemical ingestion, firearm-related attempts, and other methods. Among overdose cases, psychiatric medications—particularly antidepressants—were most frequently used. Detailed distributions are shown in Figure 1 and Figure 2.
Outpatient Follow-upOutpatient psychiatric follow-up was recommended to 36.8% of patients; however, nearly half of them did not attend follow-up visits. Patients with a prior suicide attempt, previous psychiatric treatment, or a psychiatric diagnosis during ED evaluation were significantly more likely to attend follow-up (p<0.001 for all). Other variables were not significantly associated. Detailed comparisons are presented in Supplementary Table 1.
In multivariate analysis, prior suicide attempt (OR = 2.571, p=0.019), previous psychiatric treatment (OR = 7.585, p<0.001), and psychiatric diagnosis during ED evaluation (OR = 11.738, p<0.001) independently predicted follow-up adherence (Table 1).
Recurrent Suicide AttemptsFourteen patients re-presented with a suicide attempt within one year. Recurrent attempts were significantly associated with prior suicide attempts and psychiatric history, and were more likely to involve non-medication methods such as firearms or hanging (p=0.043). No association was found with age, gender, current diagnosis, or follow-up adherence. Detailed findings are shown in Supplementary Table 2.
Multivariate analysis identified prior suicide attempt as the only significant predictor of recurrence (OR = 1.643, p=0.017) (Table 2).
Psychiatric DiagnosesHalf of the patients had a prior psychiatric diagnosis, most commonly major depressive disorder. Post-evaluation diagnoses showed an increase in adjustment disorder, while no overall significant difference was observed between pre- and post-attempt diagnoses (p=0.586). Details are provided in Figure 3.
Discussion
This study examined the clinical and disease-related characteristics, follow-up processes, and recurrent suicide attempts of patients who presented to the ED after a suicide attempt within a one-year period using retrospective patient data. A review examining 90 studies showed that most people who made a serious but non-fatal suicide attempt did not make another attempt and had a survival rate of 93%.9 Therefore, initial intervention in patients is critical. Our study observed that 49.2% of the patients (n = 162) did not consult a psychiatrist in the ED. Similar to the results of this study, the survey conducted by Reulbach and Bleich reported that up to 45% of SA cases,10 and the study conducted by J. Suokas and J. Lonnqvist reported that 46% of the patients did not receive psychiatric consultation from the emergency department. It was observed that psychiatry was consulted less in patients who did not have a psychiatric disease diagnosis in the past, who did not have recurrent suicide attempts, and who were intoxicated when they presented to the ED after a suicide attempt.11 Our study observed that most patients referred from the emergency department to orthopedics and intensive care units were not consulted by a psychiatrist before discharge. This may be because physicians from departments other than emergency and psychiatry departments have less education and sensitivity in approaching patients who attempt suicide. The decision to refer to psychiatric consultation may sometimes depend on the hospital's practices rather than the patient's characteristics. In another study evaluating psychiatric consultations, it was found that those who attempted suicide using alcohol and substance use or violent methods (such as cutting and piercing) were less frequently referred to psychiatric consultation. This was explained by the negative attitudes of healthcare professionals towards alcohol and substance use and violent behavior.12 In addition, emergency department physicians may tend not to refer patients who are at low risk of death and who are not referred to psychiatric consultation. This situation may lead to incorrect and potentially dangerous results.11 For example, the correct diagnosis rates of psychiatric illnesses by physicians other than psychiatrists may be low.13 In one study, it was stated that non-psychiatric physicians could correctly diagnose 26.5% of anxiety disorders and only 57% of depressive disorders.14
After the initial evaluation in the ED, most patients are referred to an outpatient clinic for follow-up by a psychiatrist.15 In this study, although 121 (36.77%) patients were recommended for outpatient follow-up by a psychiatrist, 60 (49.58%) of those patients did not have any psychiatric outpatient follow-up. Fourteen patients attempted suicide again within one year and presented to the emergency department. Five of these patients had never been consulted by a psychiatrist in their previous attempts. Three were admitted to the inpatient ward, five were sent home with an outpatient follow-up recommendation, and they had attended at least one follow-up visit within the last year. One had not been consulted in his first attempt, but later sought treatment at an outpatient psychiatric clinic. These results raise the following question: Could the follow-up of patients recommended for outpatient clinic follow-up by mental health professionals prevent suicide attempts?
In one study, it was observed that the rate of individuals who attempted suicide receiving outpatient psychiatric care after being discharged from the emergency department decreased from 35% in the first month to 26% in the third month. It has been reported that increasing the level of education and having more mental health interviews in the emergency department positively affected the rate of accessing outpatient psychiatric services.16 A study examining the medical records of 525 patients who presented to the ED with SA found that only 20.4% attended the psychiatry outpatient clinic after discharge. In addition to having a high level of education, having religious beliefs and having received previous psychiatric treatment were seen as factors that increased compliance with treatment, while being drunk at the time of the suicide attempt was found to be a factor that decreased compliance with treatment.6 In a similar study conducted in Spain, 69% of patients who had suicidal behavior were referred to the psychiatry outpatient clinic, 50.5% of the participants attended the follow-up process within 6 months, and 23.3% of the participants attempted suicide again within 6 months. While previous suicide attempts are seen as a risk factor for recurrent suicide attempts, participation in the follow-up of mental health services and advanced age have been stated as protective factors against recurrent suicide attempts.17 In a study in which mental health services were provided by home visits to patients who applied with suicide attempts for 3 years, it was shown that home visits were an effective method in increasing the compliance rates of patients who attempted suicide for post-outpatient care, but it was reported that they did not have a significant effect in preventing recurrent suicidal behaviors. However, home visits may have served as social control and reminders in increasing patients' compliance.18 Telephone communication may also help identify individuals at high risk of further suicide attempts and promptly refer them for emergency care.19 Other factors, such as the lack of insurance and lack of ongoing communication with the counselor during the initial patient assessment, may negatively affect follow-up processes.20 Individuals who survive a suicide attempt are at risk of re-attempting, especially immediately after the attempt. Including these individuals in treatment should be one of the main focuses of mental health professionals. In this study, a strong statistical significance was found between recurrent suicide attempts and previous suicide attempts. Predicting recurrences in a patient who has made a first suicide attempt is an important task for psychiatrists. In a study conducted by Beghi et al.,21 similar to the data in our study, the strongest predictors of repeated suicide attempts were found to be a previous attempt. In addition, it was reported that unemployment, not being married, depression, childhood sexual abuse, and personality disorders predicted recurrent SA, while older age and male gender, together with a previous SA, were more strongly associated with completed SA. In this study, Bengi emphasized the purpose of suicide assessment as positioning a person in a hypothetical risk plane to assess suicide risk and to enable a more conscious intervention, especially in the period following the attempt.21 It has been reported that scheduling regular follow-up appointments by mental health workers for patients presenting with SA, continuity with the same therapist, and regular telephone communication with those who do not want to go to treatment reduces suicide attempts.22
Studies have shown that 60-98% of suicides are associated with a psychiatric disease.23 The remaining ones are often found to be related to reasons such as financial, relational crises, discrimination, violence, and war.1 In our study, 52% (n = 171) of those who attempted suicide received a psychiatric diagnosis. 65.49% (n = 112) of these 171 patients received a diagnosis of major depressive disorder and adjustment disorder. The data in our study confirm that more than half of the suicide attempts are diagnosed with a mental illness. However, in our study, it was a striking finding that the diagnosis of AjD, which was only in 15 patients before the suicide attempt, increased to 44 as a result of the evaluation of patients who presented to the ED after a suicide attempt. These individuals diagnosed with adjustment disorder often prefer methods with a high probability of survival, such as medication and sharp objects.24 Likewise, in this study, it was found that 93.2% of the patients diagnosed with adjustment disorder attempted suicide with medication or a tool. It should not be forgotten that if the diagnosis and treatment of psychiatric diseases could be improved by 100% globally, it is predicted that suicide rates worldwide could decrease by 20.5%.23 In our study, we found that the most commonly used method of suicide attempt is taking high doses of medication. Attempting suicide by taking high doses of medication is the most common method used by patients presenting with suicide attempts in emergency services in Türkiye.4
RecommendationsThis study examined adaptation to outpatient psychiatry follow-up among patients presenting to the emergency department after a suicide attempt and factors influencing recurrence. Prior suicide attempts, past psychiatric diagnoses, and diagnoses during emergency evaluation increased compliance with follow-up. Previous suicide attempts were also a significant risk factor for recurrence. Suicide attempts are a preventable public health problem, and timely interventions in the emergency department are crucial. Educating healthcare professionals, developing personalized interventions, ensuring follow-up continuity, and using community-based suicide prevention strategies are essential steps to reduce suicidal behavior.
Limitations
This study is limited by its retrospective and single-center design, which restricts generalizability and prevents causal inferences. Some sociodemographic and clinical variables were unavailable, and outpatient follow-up was assessed only as attendance. The small number of recurrent attempts and the one-year follow-up period may have limited the findings.
Conclusion
Previous suicide attempt was the strongest predictor of recurrence, while prior and ED-diagnosed psychiatric disorders were associated with better follow-up adherence. Early psychiatric evaluation and structured follow-up in the ED may reduce recurrence, though broader preventive strategies are also needed.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Due to the retrospective design of the study, the requirement for informed consent was waived by the ethics committee.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.K.S.
Methodology: G.K.S.
Software: G.K.S.
Validation: G.K.S.
Formal Analysis: V.D.
Investigation: V.D.
Resources: V.D.
Data Curation: V.D.
Writing – Original Draft Preparation: G.K.S.
Writing – Review & Editing: G.K.S.
Visualization: G.K.S.
Supervision: G.K.S.
Project Administration: G.K.S.
Funding Acquisition: G.K.S.
AI Usage Disclosure
The authors declare that no AI-assisted technologies were used.
Abbreviations
ED: Emergency department
ICD-10: International classification of diseases 10
OR: Odds ratio
SA: Suicide attempt
SPSS: Statistical package for the social sciences
STROBE: Strengthening the reporting of observational studies in epidemiology
References
-
World Health Organization. Suicide worldwide in 2021: global health estimates. World Health Organization; 2025.
-
Bachmann S. Epidemiology of suicide and the psychiatric perspective. Int J Environ Res Public Health. 2018;15(7):1425. doi:10.3390/ijerph15071425
-
Pirkis J, Dandona R, Silverman M, et al. Preventing suicide: a public health approach to a global problem. Lancet Public Health. 2024;9(10):e787-e795. doi:10.1016/s2468-2667(24)00149-x
-
Carrigan CG, Lynch DJ. Managing suicide attempts: guidelines for the primary care physician. Prim Care Companion J Clin Psychiatry. 2003;5(4):169-174. doi:10.4088/pcc.v05n0405
-
Tidemalm D, Långström N, Lichtenstein P, Runeson B. Risk of suicide after suicide attempt according to coexisting psychiatric disorder: Swedish cohort study with long-term follow-up. BMJ. 2008;337:a2205. doi:10.1136/bmj.a2205
-
Roy A. Risk factors for suicide in psychiatric patients. Arch Gen Psychiatry. 1982;39(9):1089-1095. doi:10.1001/archpsyc.1982.04290090071014
-
Shin J, Yang S, Park DH, et al. Predictors of psychiatric outpatient adherence after an emergency room visit for a suicide attempt. Psychiatry Investig. 2020;17(9):896-901. doi:10.30773/pi.2020.0130
-
Owens D, Horrocks J, House A. Fatal and non-fatal repetition of self-harm: systematic review. Br J Psychiatry. 2002;181:193-199. doi:10.1192/bjp.181.3.193
-
Reulbach U, Bleich S. Suicide risk after a suicide attempt. BMJ. 2008;337:a2512. doi:10.1136/bmj.a2512
-
Suokas J, Lönnqvist J. Selection of patients who attempted suicide for psychiatric consultation. Acta Psychiatr Scand. 1991;83(3):179-182. doi:10.1111/j.1600-0447.1991.tb05520.x
-
Suominen KH, Isometsä ET, Lönnqvist JK. Attempted suicide and psychiatric consultation. Eur Psychiatry. 2004;19(3):140-145. doi:10.1016/j.eurpsy.2003.12.004
-
Goldberg D. The recognition of psychiatric illness by non-psychiatrists. Aust N Z J Psychiatry. 1984;18(2):128-133. doi:10.3109/00048678409158781
-
Bahçeci B, Güveli H, Kandemir G, et al. The evaluation of psychiatric pre-diagnoses diagnosed by non-psychiatric doctors in an adult emergency service. J Kartal Train Res Hosp. 2011;22(2):65-69.
-
Kammer J, Rahman M, Finnerty M, et al. Most individuals are seen in outpatient medical settings prior to intentional self-harm and suicide attempts treated in a hospital setting. J Behav Health Serv Res. 2021;48(2):306-319. doi:10.1007/s11414-020-09717-1
-
Costemale-Lacoste JF, Balaguer E, Boniface B, et al. Outpatient treatment engagement after suicidal attempt: a multisite prospective study. Psychiatry Res. 2017;258:21-23. doi:10.1016/j.psychres.2017.09.062
-
Ramos-Martín J, Gómez Sánchez-Lafuente C, Martínez-García AI, et al. Suicidal behavior in persons attended in out-of-hospital emergency services in Spain. Front Psychiatry. 2023;14:1235583. doi:10.3389/fpsyt.2023.1235583
-
Van Heeringen C, Jannes S, Buylaert W, et al. The management of non-compliance with referral to out-patient after-care among attempted suicide patients: a controlled intervention study. Psychol Med. 1995;25(5):963-970. doi:10.1017/s0033291700037454
-
Vaiva G, Ducrocq F, Meyer P, et al. Effect of telephone contact on further suicide attempts in patients discharged from an emergency department: randomized controlled study. BMJ. 2006;332(7552):1241-1245. doi:10.1136/bmj.332.7552.1241
-
Magnusson A, Hedges JR, Vanko M, et al. Follow-up compliance after emergency department evaluation. Ann Emerg Med. 1993;22(3):560-565.
-
Beghi M, Rosenbaum JF, Cerri C, Cornaggia CM. Risk factors for fatal and nonfatal repetition of suicide attempts: a literature review. Neuropsychiatr Dis Treat. 2013;9:1725-1736. doi:10.2147/ndt.s40213
-
Appleby L, Shaw J, Amos T, et al. Suicide within 12 months of contact with mental health services: national clinical survey. BMJ. 1999;318(7193):1235-1239. doi:10.1136/bmj.318.7193.1235
-
Bertolote JM, Fleischmann A, De Leo D, Wasserman D. Psychiatric diagnoses and suicide: revisiting the evidence. Crisis. 2004;25(4):147-155. doi:10.1027/0227-5910.25.4.147
-
Bolu A, Doruk A, Ak M, et al. Suicidal behavior in adjustment disorder patients. Dusunen Adam J Psychiatry Neurol Sci. 2012;25(1):58-62. doi:10.5350/dajpn2012250107
-
Ata EE, Bayrak NG, Yılmaz EB. Evaluation of cases presenting to the emergency department due to suicide attempt: a one-year retrospective study. Cukurova Med J. 2021;46(4):1675-1686.
Figures
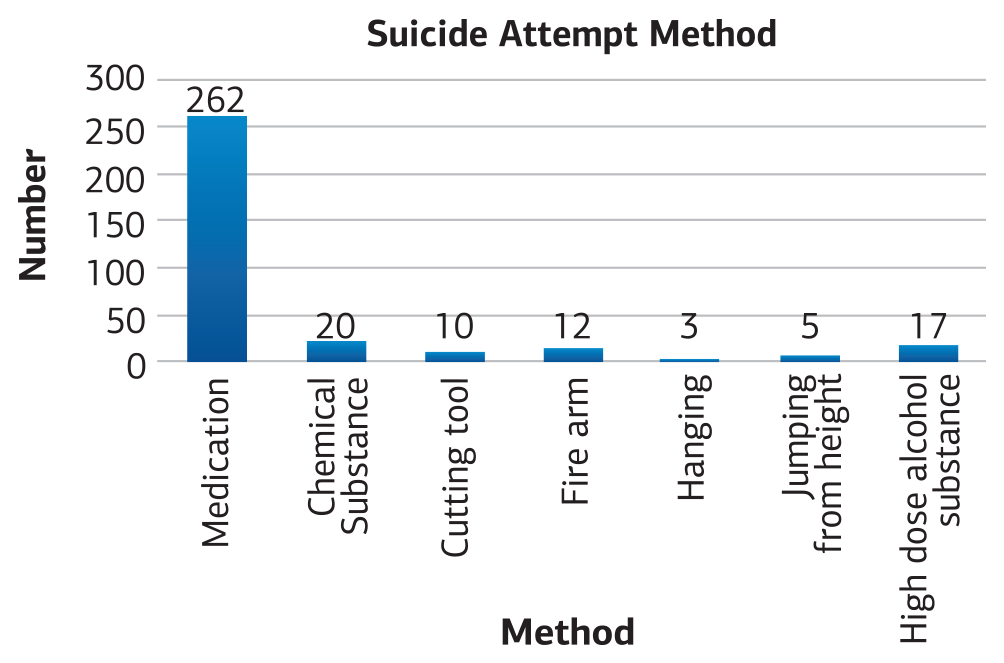
Figure 1. Suicide attempt method evaluated in the emergency department
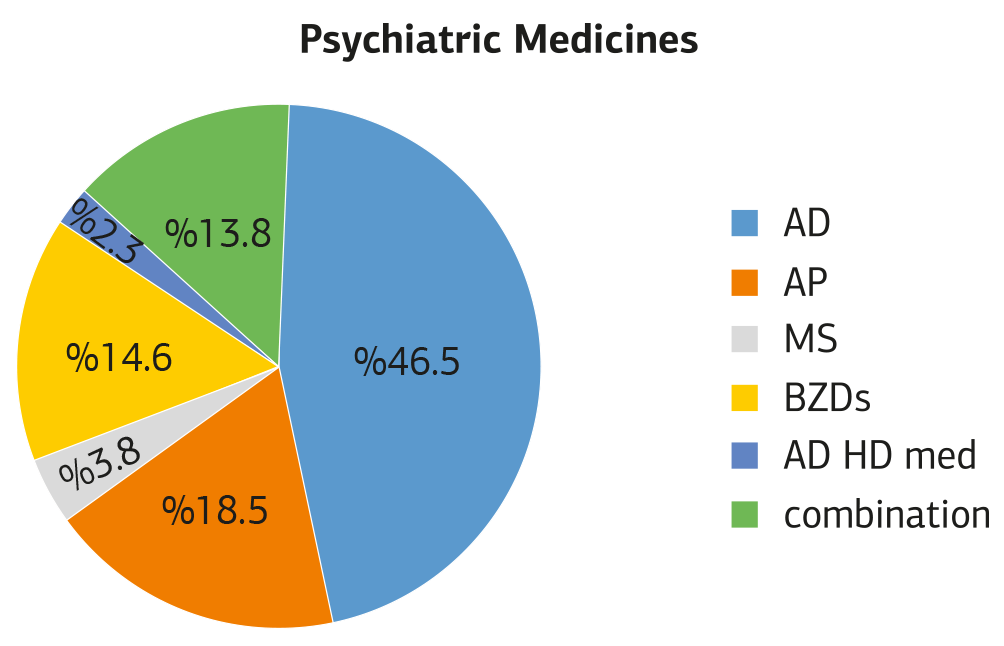
Figure 2. Group distribution of psychiatric drugs
Abbreviations: AD: Antidepressant, AP: Antipsychotic, BZDs: Benzodiazepine, MS: mood stabilizer, ADHD med: Attention deficit hyperactivity disorder medications combination: Combinations of these medications
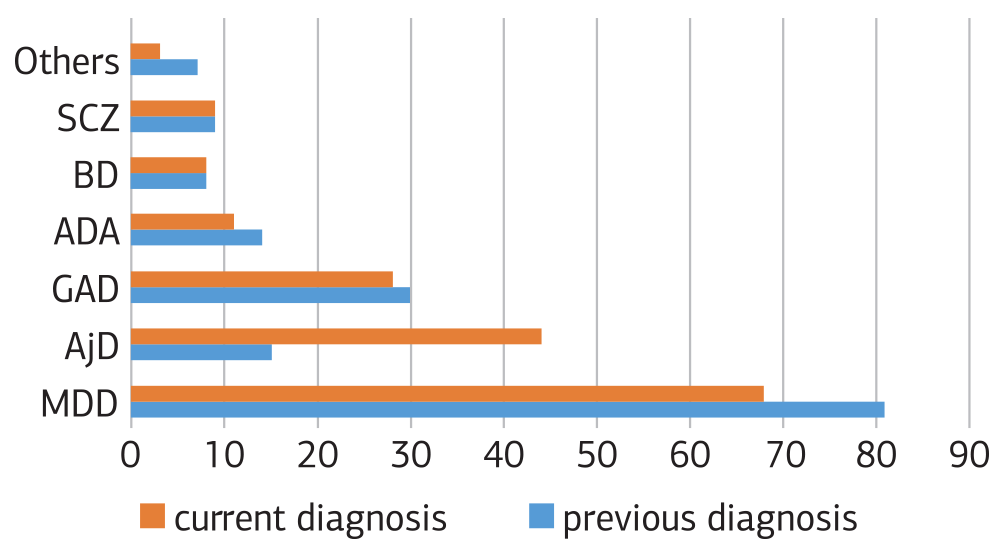
Figure 3. Comparison of pre-suicide and current diagnoses
Abbreviations: MDD: Major depressive disorder, AjD: Adjustment Disorder, GAD: Generalized Anxiety Disorder, ADA: Alcohol and Drug Addiction, BD: Bipolar Disorder, SCZ: Schizophrenia
Tables
Table 1. Multivariate logistic regression analysis for prediction of psychiatric outpatient follow up
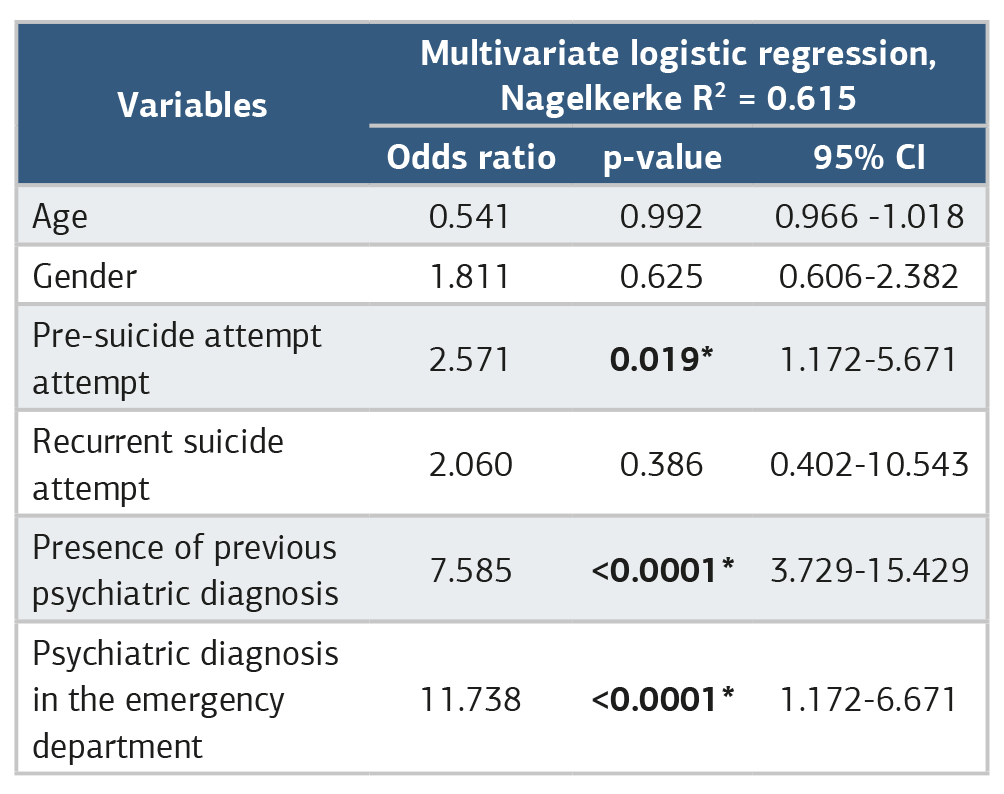
*statistically significant (p<0.05)
Table 2. Multivariate logistic regression analysis for repeated suicide attempts
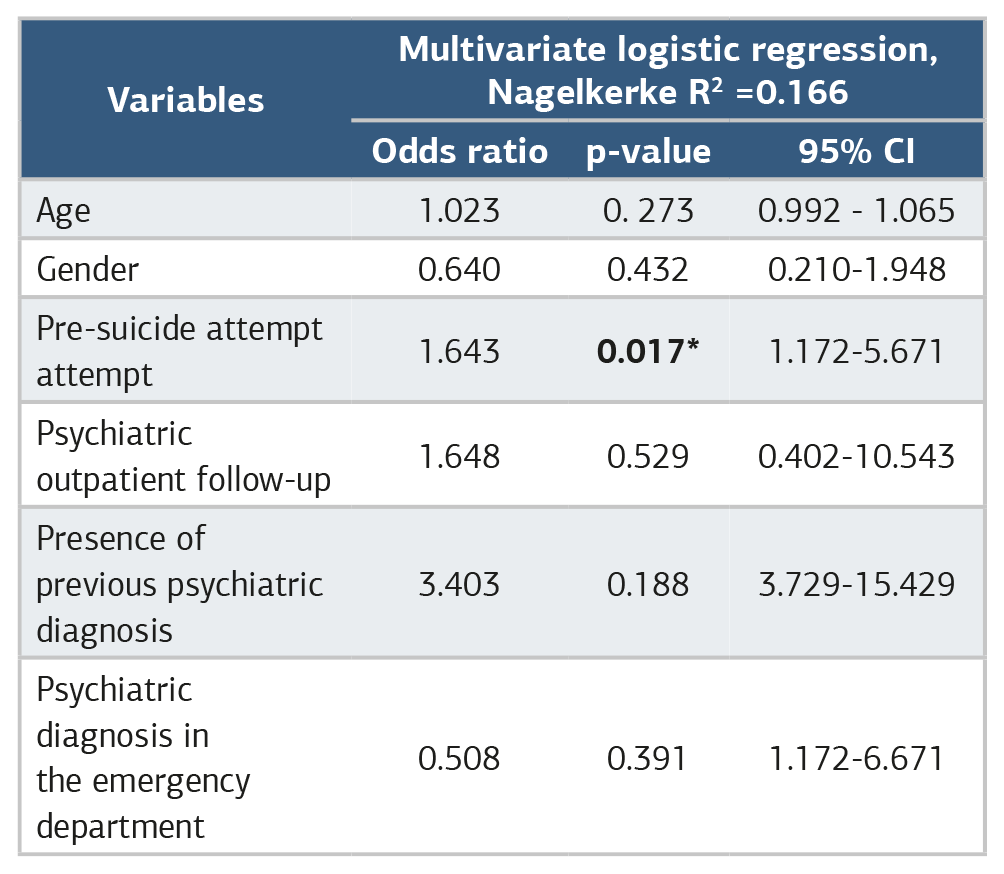
*statistically significant (p<0.05)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gökçe Kavak Sinanoğlu, Veysel Doğan. Follow-up of recurrent suicide attempts of patients admitted to the emergency department. Ann Clin Anal Med 2026;17(7):704-708. doi:10.4328/ACAM.50155
- Received:
- April 8, 2026
- Accepted:
- May 17, 2026
- Published Online:
- May 3, 2026
- Printed:
- July 1, 2026