
Evaluation of exacerbation factors and CRP in stable bronchiectasis by BSI and E-FACED indices
Bronchiectasis exacerbation and inflammation
Authors
Abstract
AimThis study aims to evaluate the factors affecting systemic inflammation (C-reactive protein [CRP]) and exacerbation frequency in patients with stable bronchiectasis, specifically focusing on subgroup analyses of parameters within the E-FACED and bronchiectasis severity index (BSI) severity scores.
MethodsA total of 107 stable bronchiectasis patients diagnosed via high-resolution computed tomography (HRCT) were enrolled. Pulmonary function tests and quantitative serum CRP measurements were performed. Disease severity was assessed using the E-FACED (0-9 points) and BSI (0-26 points) scoring systems.
ResultsThe mean BSI and E-FACED scores were 7.23 ± 4.92 and 3.46 ± 2.63, respectively. CRP levels increased significantly with disease severity (p=0.005 for BSI; p=0.020 for E-FACED). CRP showed significant correlations with Pseudomonas aeruginosa colonization and forced expiratory volume in the first second (FEV₁)%. Exacerbation frequency correlated strongly with BSI, E-FACED, hospitalizations, modified Medical Research Council (mMRC) score, and FEV₁%. While exacerbation rates were significantly higher in patients with comorbid asthma or chronic obstructive pulmonary disease (COPD) than in those with bronchiectasis alone (p<0.001), no significant difference in CRP levels was observed between these groups (p=0.902).
ConclusionBoth BSI and E-FACED scores effectively reflect not only clinical prognosis but also the systemic inflammatory burden (CRP) in non-cystic fibrosis bronchiectasis. While CRP levels are primarily driven by FEV₁ impairment and Pseudomonas aeruginosa colonization, the lack of a direct correlation between CRP and exacerbation frequency suggests that stable-state systemic inflammation represents chronic structural damage rather than acute risk. Furthermore, the presence of comorbid asthma or COPD significantly increases exacerbation rates, necessitating more aggressive personalized management strategies beyond standard severity scoring.
Keywords
Introduction
Bronchiectasis is a chronic respiratory disease characterized by various etiologies and associated with symptoms such as cough, sputum production, and hemoptysis. Its progression and pathogenesis are driven by a "vicious cycle" dominated by airway infection, airway inflammation, and structural damage.1 To evaluate disease severity, clinical scoring systems such as the E-FACED score (E: at least one exacerbation requiring hospitalization in the previous year, F: FEV₁ (FEV₁: Forced Expiratory Volume in the first second), A: age, C: colonization, E: number of affected lobes, D: dyspnea) and the Bronchiectasis Severity Index (BSI) have been developed.2,3 The E-FACED score is a six-item grading system designed to predict mortality and exacerbations in patients followed over a five-year period.2 Conversely, the BSI is a seven-item scale that defines the risk for future mortality, hospitalization, and exacerbations.3 In stable bronchiectasis, a significant correlation has been demonstrated between C-reactive protein (CRP), an indicator of systemic inflammation, and both BSI and FACED scores.4 Furthermore, the correlation and suitability of these two scoring systems in assessing bronchiectasis severity have been used in Turkish patient populations.5
In clinical studies, an exacerbation of bronchiectasis is defined as a deterioration in three or more key symptoms for at least 48 hours, alongside a clinician's decision that a change in bronchiectasis treatment is required. Key symptoms include cough, increased sputum volume and/or consistency, sputum purulence, dyspnea and/or exercise intolerance, fatigue and/or malaise, and hemoptysis.6 A clinical decision typically entails prescribing antibiotics as a treatment modification.7
Frequent exacerbations in patients with bronchiectasis can predict future mortality and hospitalizations. Notably, while the E-FACED scoring system utilizes the definition of exacerbations requiring hospitalization, the BSI scoring system employs the broader definition of bronchiectasis exacerbation.2,3
Subgroup analyses of parameters within the E-FACED and BSI scoring systems, specifically regarding exacerbations and CRP, have not been adequately investigated in patients with stable bronchiectasis in previous studies. Therefore, this study aims to investigate the factors affecting CRP levels and exacerbation frequency in patients with stable bronchiectasis, utilizing the E-FACED and BSI scores developed to measure disease severity.
Materials and Methods
Patients followed at the Chest Diseases clinics of Balıkesir University Faculty of Medicine and Sakarya Training and Research Hospital, with a definitive diagnosis of bronchiectasis confirmed by high-resolution computed tomography (HRCT), were enrolled in the study. Exclusion criteria included patients with bronchiectasis secondary to immunodeficiency, allergic bronchopulmonary aspergillosis (ABPA), or primary ciliary dyskinesia, as well as those with heart failure, malignancy, pregnancy, or chronic renal failure. Additionally, patients who had used antibiotics or steroids within the last month or reported an acute exacerbation were excluded. A total of 107 patients meeting these criteria were included in the study.
All patients underwent spirometry. For serum CRP level measurement, 3 cc of venous blood was collected into biochemistry tubes. Quantitative determination of CRP levels was performed using the nephelometric method with a BN 200 device. The reference range for healthy individuals was 0.00–5.00 mg/L according to the method employed.
E-FACED and BSI ScoringThe E-FACED score comprises six variables: history of exacerbations in the past year, FEV₁%, age, Pseudomonas aeruginosa (P. aeruginosa) colonization, radiological extent, and dyspnea assessment using the modified Medical Research Council (mMRC) scale. The total score is obtained by summing the points for each variable, with a range of 0 to 9.
The BSI score includes nine variables: age, body mass index (BMI), FEV1%, hospitalizations in the past 2 years, number of exacerbations in the past year, dyspnea assessed using the mMRC scale, P. aeruginosa colonization, colonization with other microorganisms, and radiological extent. The total score ranges from 0 to 26.
Ethical ApprovalThe study was approved by the Ethics Committee of Balıkesir University Health Sciences Research Ethics Committee (Date: 06.05.2025, Decision No: 2025/179).
Statistical AnalysisContinuous variables are presented as mean ± standard deviation. Differences between the two groups were analyzed using the t-test for normally distributed variables and the Mann-Whitney U test for non-normally distributed variables. For analyzing more than two groups, ANOVA was used for normally distributed data, and the Kruskal-Wallis test was used for non-normally distributed data. Correlations were evaluated using Spearman's rank correlation test. A p-value of less than 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
The baseline clinical characteristics of the study participants are presented in Supplementary Table 1. The mean BSI score was 7.23 ± 4.92, and the mean E-FACED score was 3.46 ± 2.63. When evaluated by disease severity, CRP levels in stable bronchiectasis patients increased significantly as severity increased (p=0.005 for BSI and p=0.020 for E-FACED, respectively). A significant correlation was observed between CRP and both the BSI and FACED scores (r = 0.28 and 0.24, respectively).
In the subgroup analysis, CRP was significantly correlated with Pseudomonas aeruginosa colonization (r = 0.23, p=0.034) and FEV₁% (r = −0.35, p=0.002) (Table 1).
Exacerbations were significantly correlated with hospitalizations (r = 0.51, p<0.001), mMRC dyspnea score (r = 0.57, p<0.001), number of affected lobes (r = 0.27, p=0.008), FEV₁% (r = −0.44, p<0.001), and colonization with other microorganisms (r = 0.25, p=0.011) (Table 2).
When patients were categorized into three groups based on the coexistence of chronic respiratory diseases—bronchiectasis only (n = 47), asthma-bronchiectasis overlap (n = 37), and chronic obstructive pulmonary disease (COPD)-bronchiectasis overlap (n = 23)-a significant difference was found in the number of exacerbations between the groups (p<0.001) (Table 3). Sub-group analysis revealed a significant difference between the bronchiectasis-only group and the other two groups with comorbid chronic airway diseases. However, no significant difference in the number of exacerbations was observed between the asthma and COPD groups. Regarding CRP, which indicates systemic inflammation, no significant difference was observed between the three groups (p=0.902).
Finally, no significant correlation was found between the number of exacerbations and CRP levels in this study (r = 0.097, p=0.34).
Discussion
In this study, bronchiectasis severity was evaluated using the E-FACED and BSI scoring systems, which consist of various clinical and radiological variables. CRP levels and exacerbation frequencies in patients with stable bronchiectasis were analyzed alongside these scoring parameters. Significant correlations were identified among CRP levels, E-FACED/BSI scores, FEV₁%, and P. aeruginosa colonization. Furthermore, the number of exacerbations showed significant correlations with E-FACED/BSI scores, FEV₁%, hospitalization history, mMRC dyspnea score, colonization with other microorganisms, and radiological extent.
Bronchiectasis exacerbations are critical events in the clinical course of the disease and are integral components of severity scoring systems such as BSI and E-FACED.2,3 These scoring tools serve as valuable assets for clinicians in assessing prognosis and guiding the management of bronchiectasis patients.8 In the present study, significant correlations were found between the number of exacerbations and both E-FACED and BSI scores (r = 0.56 and r = 0.60, respectively). Both scoring systems utilize historical exacerbation data. A recent study demonstrated that frequent past exacerbations are the strongest predictor of future exacerbations. This emphasizes the need for clinicians to focus on the "frequent exacerbator" phenotype, as these patients experience higher hospitalization rates and increased five-year mortality.9
Data from 21 observational cohort studies comparing patients with and without P. aeruginosa colonization has been shown to be associated with increased exacerbations, hospitalizations, and mortality.10 In a multicenter European study investigating the relationship between bacterial infection and exacerbation risk during the stable phase, chronic P. aeruginosa infection was independently associated with exacerbation frequency.11 However, in our study, no significant relationship was found between P. aeruginosa colonization and exacerbations. This discrepancy may be attributed to the relatively small number of patients with P. aeruginosa colonization in our study population. Conversely, we identified a significant, albeit weak, positive correlation between colonization with other microorganisms and exacerbations (r = 0.25, p=0.025).
The frequent exacerbator phenotype in bronchiectasis is characterized by factors such as low FEV₁% and radiological severity, both of which independently predict future exacerbation frequency.9 Consistent with earlier findings, our study revealed a significant correlation among low FEV₁%, the number of affected lobes, and exacerbation rates.
Regarding systemic inflammation, a previous study reported no significant correlation between CRP levels and future exacerbations in patients with stable bronchiectasis.12 This finding was highlighted in a recent meta-analysis, which emphasized that while systemic inflammation may originate from airway inflammation, the host inflammatory response plays a more prominent role during an exacerbation.13 Similarly, our study found no significant correlation between CRP and the number of exacerbations. However, when evaluating CRP as an indicator of systemic inflammation, we observed significant positive correlations with BSI and E-FACED scores and the presence of P. aeruginosa colonization, whereas a negative correlation was found with FEV₁%.
Recent literature indicates a significant overlap between bronchiectasis and other chronic respiratory diseases, with approximately 31% of bronchiectasis patients diagnosed with asthma and 25% with COPD.14,15 Our study identified similar rates of comorbid COPD and asthma. Such comorbidities not only complicate the clinical picture during stable phases but also influence the frequency, severity, and clinical characteristics of exacerbations, thereby impacting overall patient health and therapeutic approaches.14,15 Due to the similarity in clinical symptoms—such as increased cough, wheezing, dyspnea, and sputum changes—distinguishing the specific role of each disease during an exacerbation remains a challenge in patients with multiple chronic lung conditions.16
Previous research has shown that the risk of exacerbation increases when bronchiectasis coexists with other airway diseases. A Chinese study comparing patients with bronchiectasis alone to those with comorbid asthma found that the presence of asthma was independently associated with bronchiectasis exacerbations.17 Similarly, patients with COPD-related bronchiectasis have been shown to have higher exacerbation frequencies compared to those without COPD.9,18 In a European cohort study, COPD was independently associated with the frequency of bronchiectasis exacerbations over a five-year follow-up period.9 Consistent with these reports, our study demonstrated that the frequency of exacerbations was significantly higher in bronchiectasis patients with comorbid asthma or COPD.
Limitations
Our study has several limitations that should be acknowledged. First, the relatively small sample size may have limited the statistical power required to fully elucidate the impact of critical parameters, such as P. aeruginosa colonization, on exacerbation rates. Second, the retrospective recording of exacerbation frequencies may have introduced recall bias. Third, systemic inflammation was assessed through a single-point CRP measurement, which may not fully reflect the dynamic nature of the inflammatory process over time. Finally, the inability to fully determine the microbiological profile in patients who could not produce sputum may have influenced the strength of the observed relationship between severity scores and exacerbations.
Conclusion
This study demonstrates that the BSI and E-FACED scoring systems, utilized to determine disease severity in patients with non-cystic fibrosis bronchiectasis, reflect not only the clinical prognosis but also CRP levels, an indicator of systemic inflammation. It was observed that systemic inflammation increases in correlation with the severity of bronchiectasis. In particular, low FEV₁% values and P. aeruginosa colonization were found to be the factors most strongly associated with the systemic inflammatory load. The absence of a direct correlation between the frequency of exacerbations and CRP levels suggests that systemic inflammation during the stable period represents existing structural damage and chronic bacterial load rather than the immediate risk of exacerbation. The presence of comorbid asthma and COPD significantly increases the frequency of exacerbations. This situation may indicate that bronchiectasis patients with concomitant chronic airway diseases require more aggressive exacerbation management compared to those with bronchiectasis alone. In the management of stable bronchiectasis patients, BSI and E-FACED scores are reliable tools for understanding both the functional status and the inflammatory load of the patient. However, especially in individuals with comorbid chronic airway disease, there is a need to develop personalized treatment strategies beyond scoring systems to reduce exacerbations.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: H.C.
Methodology: H.C.
Formal Analysis: H.C.
Investigation: H.C.
Data Curation: H.C.
Writing – Original Draft Preparation: H.C.
Writing – Review & Editing: H.C.
Supervision: H.C
AI Usage Disclosure
The authors did not use artificial intelligence (AI) tools in the preparation of this manuscript.
Abbreviations
ABPA: Allergic bronchopulmonary aspergillosis
ANOVA: Analysis of variance
BMI: Body mass index
BSI: Bronchiectasis severity index
COPD: Chronic obstructive pulmonary disease
CRP: C-reactive protein
E-FACED: Exacerbation, forced expiratory volume in the first second, age, chronic colonization, extension, dyspnea
FEV₁: Forced expiratory volume in the first second
HRCT: High-resolution computed tomography
mMRC: Modified Medical Research Council
SPSS: Statistical Package for the Social Sciences
STROBE: Strengthening the reporting of observational studies in epidemiology
References
-
Barbosa M, Chalmers JD. Bronchiectasis. Presse Med. 2023;52(3):104174. doi:10.1016/j.lpm.2023.104174
-
Martinez-Garcia MA, Athanazio RA, Girón R, et al. Predicting high risk of exacerbations in bronchiectasis: the E-FACED score. Int J Chron Obstruct Pulmon Dis. 2017;12:275-284. doi:10.2147/copd.s121943
-
Chalmers JD, Goeminne P, Aliberti S, et al. The bronchiectasis severity index: an international derivation and validation study. Am J Respir Crit Care Med. 2014;189(5):576-585. doi:10.1164/rccm.201309-1575oc
-
Coban H, Gungen AC. Is there a correlation between new scoring systems and systemic inflammation in stable bronchiectasis? Can Respir J. 2017;2017:9874068. doi:10.1155/2017/9874068
-
Coban H. Relationship between FACED and bronchiectasis severity index in the evaluation of bronchiectasis severity: cross-sectional study. Eurasian J Pulmonol. 2020;22(1):55-58. doi:10.4103/ejop.ejop_34_19
-
Hill AT, Haworth CS, Aliberti S, et al. Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research. Eur Respir J. 2017;49(6):1700051. doi:10.1183/13993003.00051-2017
-
Choi H, Chalmers JD. Bronchiectasis exacerbation: a narrative review of causes, risk factors, management and prevention. Ann Transl Med. 2022;11(1):25.
-
De Angelis A, Johnson ED, Sutharsan S, Aliberti S. Exacerbations of bronchiectasis. Eur Respir Rev. 2024;33(173):240085. doi:10.1183/16000617.0085-2024
-
Chalmers JD, Aliberti S, Filonenko A, et al. Characterization of the “frequent exacerbator phenotype” in bronchiectasis. Am J Respir Crit Care Med. 2018;197(11):1410-1420. doi:10.1164/rccm.201711-2202oc
-
Finch S, McDonnell MJ, Abo-Leyah H, Aliberti S, Chalmers JD. A comprehensive analysis of the impact of Pseudomonas aeruginosa colonization on prognosis in adult bronchiectasis. Ann Am Thorac Soc. 2015;12(11):1602-1611. doi:10.1513/annalsats.201506-333oc
-
Araújo D, Shteinberg M, Aliberti S, et al. The independent contribution of Pseudomonas aeruginosa infection to long-term clinical outcomes in bronchiectasis. Eur Respir J. 2018;51(2):1701953. doi:10.1183/13993003.01953-2017
-
Posadas T, Oscullo G, Zaldivar E, et al. C-reactive protein concentration in steady-state bronchiectasis: prognostic value of future severe exacerbations. Data from the Spanish Registry of Bronchiectasis (RIBRON). Arch Bronconeumol. 2021;57(1):21-27. doi:10.1016/j.arbres.2019.12.017
-
Chalmers JD, Aliberti S, Polverino E, et al. The EMBARC European Bronchiectasis Registry: protocol for an international observational study. ERJ Open Res. 2016;2(1):00081-2015. doi:10.1183/23120541.00081-2015
-
Polverino E, Dimakou K, Traversi L, et al. Bronchiectasis and asthma: data from the European Bronchiectasis Registry (EMBARC). J Allergy Clin Immunol. 2024;154(4):1553-1562.
-
Polverino E, De Soyza A, Dimakou K, et al. The association between bronchiectasis and chronic obstructive pulmonary disease: data from the European Bronchiectasis Registry (EMBARC). Am J Respir Crit Care Med. 2024;210(1):119-127. doi:10.1164/rccm.202309-1614oc
-
Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of chronic obstructive pulmonary disease exacerbations: the Rome proposal. Am J Respir Crit Care Med. 2021;204(11):1251-1258. doi:10.1164/rccm.202108-1819pp
-
Mao B, Yang JW, Lu HW, Xu JF. Asthma and bronchiectasis exacerbation. Eur Respir J. 2016;47(6):1680-1686. doi:10.1183/13993003.01862-2015
-
Ni Y, Shi G, Yu Y, Hao J, Chen T, Song H. Clinical characteristics of patients with chronic obstructive pulmonary disease with comorbid bronchiectasis: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1465-1475. doi:10.2147/copd.s83910
Tables
Table 1. Correlations between CRP and scoring systems/variables
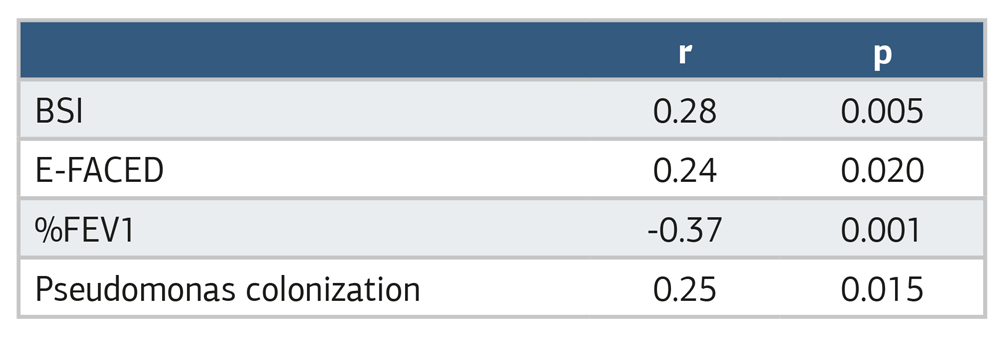
Table 2. Correlations between exacerbation frequency and scoring systems/variables
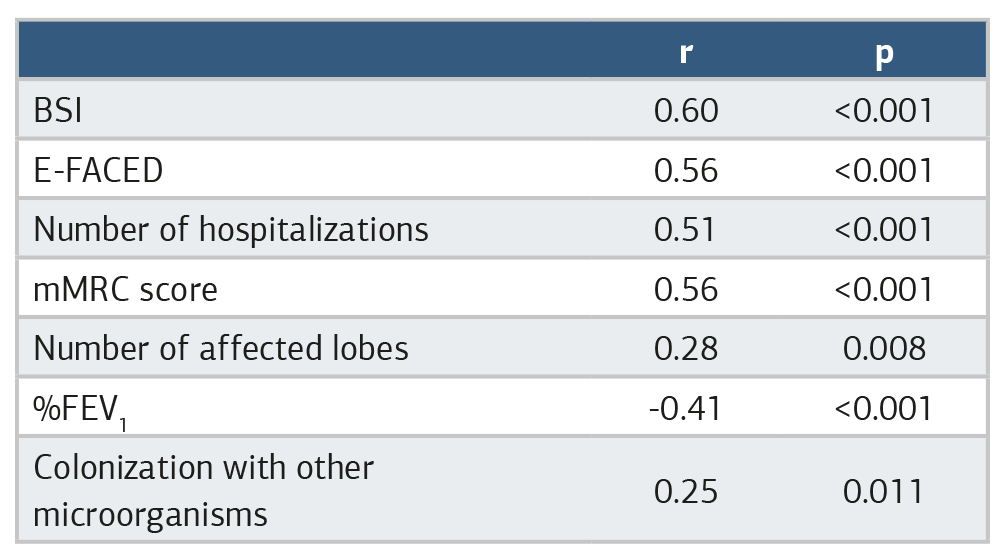
Table 3. Relationship between chronic respiratory comorbidities, exacerbations, and CRP

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hikmet Çoban. Evaluation of exacerbation factors and CRP in stable bronchiectasis by BSI and E-FACED indices. Ann Clin Anal Med 2026;17(7):690-694. doi:10.4328/ACAM.50165
- Received:
- April 20, 2026
- Accepted:
- May 17, 2026
- Published Online:
- May 3, 2026
- Printed:
- July 1, 2026