
Evaluation of the change of vitamin D deficiency by age, gender, season, and years: a report from west of Turkey
Change of vitamin D deficiency by age, gender, season, and years
Authors
Abstract
Aim In our study, we aimed to determine the frequency of vitamin D deficiency by examining vitamin D levels in children, adults, and geriatric groups and to examine vitamin D levels according to gender, months, seasons, and years.
Methods The study included 150,068 patients who applied to Muğla Sıtkı Koçman University University Training and Research Hospital polyclinics between April 2016 and December 2020. Only the initial results of patients whose 25-Hydroxy Vitamin D levels were measured more than once were evaluated. Four groups were formed as 0-4 years, 5-17 years old, adults (18-65 years old) and over 65 years old and were evaluated separately.
Results Considering all age groups, vitamin D deficiency decreased to a minimum level of 3.5% in September and increased to 22.2% in February. When the summer months are compared with winter months for all age groups, an average of 23% decrease in vitamin D deficiency is observed. In the 0-4 age group, vitamin D deficiency was found to be 1.5% in men, 3% in women, and vitamin D insufficiency was 18% in men and 17.8% in women. In the children (5-17 years old) group, vitamin D deficiency was found to be 38.8% in men and 58.5% in women. In the age group over 65, vitamin D deficiency was found to be 15.3% in men, 20.8% in women, and vitamin D deficiency was 34.9% in men and 29.4% in women.
Conclusion Vitamin D deficiency is an important problem that needs to be addressed. This situation is not only a public health problem, but also a pandemic situation. In order to improve the increasing prevalence of vitamin D deficiency, it is important to adopt this situation as an important public problem through health policies to be implemented by national-international institutions, to increase UVB exposure, vitamin D use and public interest.
Keywords
Introduction
Despite advances in medicine, vitamin D deficiency is still a global health problem. According to the World Health Organization, more than one billion people worldwide suffer from vitamin D deficiency 1,2. In North America, approximately one-third of the population is considered vitamin D deficient, while in Europe approximately 80% of the population is deficient in vitamin D. The groups most affected by this condition are infants and children, persons over the age of 65, pregnant women, and people with dark skin 3,4. Studies conducted in Turkey also show that the prevalence of vitamin D deficiency is high 13,14.
Vitamin D is a hormone-like substance produced in the body. The classical role of vitamin D is to regulate calcium homeostasis and blood pressure regulation 5. However, vitamin D is a vital component of our immune system 6,7. It also plays an important role in regulating diseases of the endocrine system. It is estimated that about 3% of the human genome is regulated by the vitamin D endocrine system. It is known that hundreds of genes function by regulating their activities 7. According to current research, vitamin D deficiency plays a role in the pathogenesis of many cancer types such as breast, colon, and prostate cancer. It has also been associated with some neurodegenerative diseases such as stroke, arthritis, diabetes, depression, heart disease, auto-immune, and Alzheimer’s disease 6,7,8,9.
Although vitamin D can be obtained from dietary products such as fish, eggs, and dairy products, most people produce vitamin D by synthesis of UVB rays through the skin. This process is very effective in the production of vitamin D 10. Between May and November, regular exposure to the sun is important to obtain vitamin D synthesis. When the whole body is exposed to sunlight for at least 10 minutes, the minimum dose of vitamin D (MED) is produced in the skin 1. While sun exposure provides about 3000 IU of vitamin D, it’s important to remember that the concentration needed is different for different skin types. This process and amount are affected by factors such as time of day, latitude, air pollution, skin color, obesity, clothing is worn, and genetic and physiological differences. The increase in the use of high-tech cosmetic products that protect against ultraviolet radiation is one of the important factors that prevent vitamin D synthesis 3,11,12.
The amount of vitamin D in serum is usually determined by measuring 25-hydroxy vitamin D, which indicates the body’s storage status. However, the reference values for vitamin D deficiency and insufficiency are still controversial, and there is no international consensus on this issue 13,14. US Institute of Medicine, US Endocrine Society Guidelines, Mayo Clinic, and Turkish Society of Endocrinology and Metabolism (TEMD) guides offer different recommendations on this subject 13,14,15. In our study, we aimed to determine the frequency of vitamin D deficiency by examining vitamin D levels in children, adults, and geriatric groups according to the recommendations in TEMD’s Practice Guide, and to examine vitamin D levels according to gender, months, seasons and years.
Statistical AnalysisData were analyzed using the open-source statistical software Jamovi (version 2.2.5.0, Sydney, Australia). Descriptive statistics were given as frequency and percentage for categorical variables, and median and interquartile range (IQR) for numerical variables. Conformity of continuous variables to normal distribution was checked with the Shapiro-Wilk test. Since the numerical variables did not meet the normal distribution condition, comparison of the two independent groups was made using the Mann-Whitney U test. The relationship between numerical variables were examined using Spearman’s correlation analysis as they did not meet the parametric test conditions. Statistical significance level p < 0.05 was considered significant.
Materials and Methods
The study included 150,068 patients who applied to Muğla Sıtkı Koçman University Training and Research Hospital polyclinics between April 1, 2016 and December 31, 2020 whose 25-Hydroxy Vitamin D levels were checked for any reason. Only the initial results of patients whose 25-Hydroxy Vitamin D levels were measured more than once were evaluated. Therefore, 397 patients were excluded from the study and 149,671 patient results were evaluated.
The pediatric, adult and geriatric groups were evaluated separately, considering that the pediatric group aged 0-4 years and the intensively recommended and used vitamin D supplements after the age of 65 may affect the results. As recommended in TEMD’s Application Guide, values below 10 ng/ml (25 nmol/L) indicate vitamin D deficiency and values between 10 ng/ml-19.9 ng/ml (25-50 nmol/L) indicate vitamin D insufficiency and 20 ng/ml (values above 50 nmol/L) were considered normal vitamin D levels. Values above 100 ng/ml were not included in the study.
25-OH Vitamin D levels were measured with the “Microparticle Enzyme Immunoassay Method” in a Cobas 601 device (Roche Diagnostic, Germany).
Ethical ApprovalAll procedures were carried out in accordance with the ethical standards of the Declaration of Helsinki. This study was approved by the Ethics Committee of the Muğla Sıtkı Koçman University Science (Date: 2021-09-14, No: 203).
Results
Demographic characteristics of the patients are presented in Supplementary Table S1, Figure 1, and Figure 2. Measured 25-Hydroxy Vitamin D levels were between a minimum of 3 ng/ml and a maximum of 100 ng/ml. Values above 100 ng/ml were not included in the study. The ages of the patients ranged from 0 to 104 years (Supplementary Table S2). A statistically significant difference was found in Vitamin D levels between all years, except for the years 2016-2020 (p < 0.001).
There was no statistical difference between the ages according to gender (p > 0.05). A significant difference was found between Vitamin D levels according to gender (p < 0.05).
A positive correlation was found between age and vitamin D deficiency (rho: 0.013, p < 0.001).
Discussion
In this study, the prevalence of vitamin D deficiency and insufficiency in Muğla was evaluated according to age, gender, season, and years.
In our study, a large population of 149,671 people were selected and divided into four groups so that the 0-4 age group and the age group over 65 who are recommended vitamin D replacement do not lead to biased results. Vitamin D cutoff points were determined according to TEMD criteria and four groups were formed: 0-4 years old, children (5-17 years old), adults, and over 65 years old 15. In this way, it was aimed to contribute to studies on vitamin D deficiency.
According to the results we obtained, considering all age groups, vitamin D deficiency decreased to a minimum level of 3.5% in September and increased to 22.2% in February. It was determined that vitamin D insufficiency decreased to minimum levels of 25.4% in September and increased to 44% in April. Studies have reported that vitamin D deficiency ranges from 46 to 80% in Turkey 16. In a study conducted by Hekimsoy et al. in the Aegean region in 2010, it was reported that there was 74.9% vitamin D deficiency and 13.8% insufficiency 17. Doğan et al. investigated vitamin D deficiency in the pediatric group in Izmir in 2015 and reported that vitamin D deficiency and insufficiency were 61% in the related study. While these rates increase up to 80% in American and European countries, it is stated that prevalence has increased in the last 20 years, especially in northern European countries 13,14.
According to our results, when the 0-4 age group is taken into account, vitamin D deficiency and insufficiency are around 20%, and vitamin D deficiency is the least common group in the whole population. However, current studies have repeatedly shown that vitamin D is of vital importance for the development and immune system of children. Vitamin D deficiency and insufficiency are around 50% (Male: 51.1%, Female: 51.2%) in the age group over 65, which is one of the most important risk groups in which vitamin D replacement is common 3,4.
And it was found to be the group with the highest values in the population. These values include a great risk for the 0-4 age group and the age group over 65. In the Middle East, despite the abundance of vitamin D, the region has the highest rate of hypovitaminosis D worldwide and cases of rickets are very common 2,3. Vitamin D deficiency, which can lead to different effects in different life stages, is caused by UVB exposure and D exposure in terms of osteoporosis and osteomalacia, especially in the geriatric group. Removal of vitamin D with replacement is of vital importance 18,19.
Vitamin D deficiency and insufficiency in our child group (5-17 years old) have great differences according to gender. While it was 38.8% in men, it was determined as 58.5% in women. There is a difference of approximately 50% by gender. When vitamin D deficiency and vitamin D insufficiency are evaluated seperately, it is seen that the majority of this difference is vitamin D deficiency.
Vitamin D deficiency in the adult group between the ages of 18-65, which we examined in more detail, includes serious differences according to gender. When the prevalence of vitamin D deficiency was examined according to TEMD criteria, it was determined to be 7% in men and 14.5% in women, while vitamin D deficiency was found to be 36% in men and 38.7% in women 15. However, based on the practice guidelines of institutions such as the US Endocrine Society, the US Geriatrics Osteoporosis Society, and the Mayo Clinic, the rate of vitamin D deficiency is found to be 43.1% in men and 53.2% in women 13,14,15. Likewise, vitamin D deficiency in the over 65 age group is 50.1% in men and 50.2% in women.
Considering all age groups, an increasing vitamin D deficiency with age has been detected. It is observed that there is an average of 23% decrease in vitamin D deficiency in summer months for all age groups when compared to winter months (Supplementary Table S3, Figure 3).
Considering all years, although the median values seem to be very close to each other, a statistically significant difference for risky groups, when the tests performed over the years are examined retrospectively, we obtained results similar to those obtained in studies conducted in the world and in Turkey 14,15.
As a result, although different rates of vitamin D deficiency are obtained in different geographies, different populations, or similar populations with similar geographical conditions, there are common causes in all geographies. These are the reasons such as the increase in spending time indoors in the modern world, the increase in cosmetic products used, the clothing habits that can change according to cultural norms, economic conditions that may prevent regular nutrition, reasons such as obesity, insufficient information about vitamin D deficiency, the indifference of the public or the insufficient work of national institutions. We believe that this epidemic may have important common factors 4. Although the Mugla region is one of the regions that receive the most sunlight in all seasons in Turkey, we believe that the same reasons are at the root of vitamin D deficiency.
Limitations
Genetic, physiological differences, body composition, and metabolic differences of patients in the population were not taken into account.
Conclusion
In conclusion, Vitamin D deficiency is an important problem that needs to be addressed. This situation is not only a public health problem-, but also a global disease situation [20]. In order to improve the increasing prevalence of vitamin D deficiency, it is important to adopt this situation as an important public problem by the health policies to be implemented by national- international institutions, to increase UVB exposure, vitamin D use, and public interest.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of the the Muğla Sıtkı Koçman
University Science (Date: 2021-09-14, No: 203)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing,
and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Clark A, Mach N. Role of vitamin D in the hygiene hypothesis: the interplay between vitamin D, vitamin D receptors, gut microbiota, and immune response. Front Immunol. 2016;7:627. doi:10.3389/fimmu.2016.00627.
-
Cashman KD. Global differences in vitamin D status and dietary intake: a review of the data. Endocr Connect. 2022;11(1):1-18. doi:10.1530/EC-21-0282.
-
Hossein-nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo Clin Proc. 2013;88(7):720-55. doi:10.1016/j.mayocp.2013.05.011.
-
Prentice A. Vitamin D deficiency: a global perspective. Nutr Rev. 2008;66(10 Suppl 2): S153-64. doi:10.1111/j.1753-4887.2008.00100.x.
-
DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr. 2004;80(6 Suppl):1689S-96S. doi:10.1093/ajcn/80.6.1689S.
-
Litonjua AA, Weiss ST. Is vitamin D deficiency to blame for the asthma epidemic? J Allergy Clin Immunol. 2007;120(5):1031-5. doi:10.1016/j.jaci.2007.08.028.
-
Kamen DL, Tangpricha V. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. J Mol Med (Berl). 2010;88(5):441-50. doi:10.1007/s00109-010-0590-9.
-
Disanto G, Chaplin G, Morahan JM, et al. Month of birth, vitamin D and risk of immune-mediated disease: a case control study. BMC Med. 2012;10:69. doi:10.1186/1741-7015-10-69.
-
Banerjee A, Khemka VK, Ganguly A, Roy D, Ganguly U, Chakrabarti S. Vitamin D and alzheimer’s disease: neurocognition to therapeutics. Int J Alzheimers Dis. 2015;2015:192747. doi:10.1155/2015/192747.
-
Reichrath J, Zouboulis CC, Vogt T, Holick MF. Targeting the vitamin D endocrine system (VDES) for the management of inflammatory and malignant skin diseases: an historical view and outlook. Rev Endocr Metab Disord. 2016;17(3):405-17. doi:10.1007/s11154-016-9353-4.
-
Yan L, Zhou B, Wang X, et al. Older people in China and the United Kingdom differ in the relationships among parathyroid hormone, vitamin D, and bone mineral status. Bone. 2003;33(4):620-7. doi:10.1016/s8756-3282(03)00216-3.
-
Gatta E, Cappelli C. Sunscreen and 25-hydroxy vitamin D levels: Friends or foes? A systematic review and meta-analysis. Endocr Pract. 2025;31(6):839-48. doi:10.1016/j.eprac.2025.03.014.
-
Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clin Proc. 2010;85(8):752-8. doi:10.4065/mcp.2010.0138.
-
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911-30. doi:10.1210/jc.2011-0385.
-
Demay MB, Pittas AG, Bikle DD, et al. Vitamin D for the preventation of disease: an endocrine society clinical ractice guideline. J Clin Endocrinol Metab. 2024;109(8):1907-47. doi:10.1210/clinem/dgae290.
-
Açıkgöz A, Günay T, Uçku R. Gebelikte D Vitamini Gereksinimi ve Desteklenmesi [Vitamin D requirements and supplementation during pregnancy]. TAF Preventive Medicine Bulletin. 2013;12(5):597-608. doi: 10.5455/pmb.1-1346410426.
-
Hekimsoy Z, Dinç G, Kafesçiler S, et al. Vitamin D status among adults in the Aegean region of Turkey. BMC Public Health. 2010;10:782. doi:10.1186/1471-2458-10-782.
-
Pazianas M, Miller PD. Osteoporosis and chronic kidney disease-mineral and bone disorder (CKD-MBD): back to basics. Am J Kidney Dis. 2021;78(4):582-9. doi:10.1053/j.ajkd.2020.12.024.
-
Barnsley J, Buckland G, Chan PE, et al. Pathophysiology and treatment of osteoporosis: challenges for clinical practice in older people. Aging Clin Exp Res. 2021;33(4):759-73. doi:10.1007/s40520-021-01817-y.
-
Mf H. Chen TC. Vitamin D deficiency: a worldwide problem with health consequnces. Am J Clin Nutr. 2008;87(4):1080-6. doi:10.1093/ajcn/87.4.1080S.
Figures
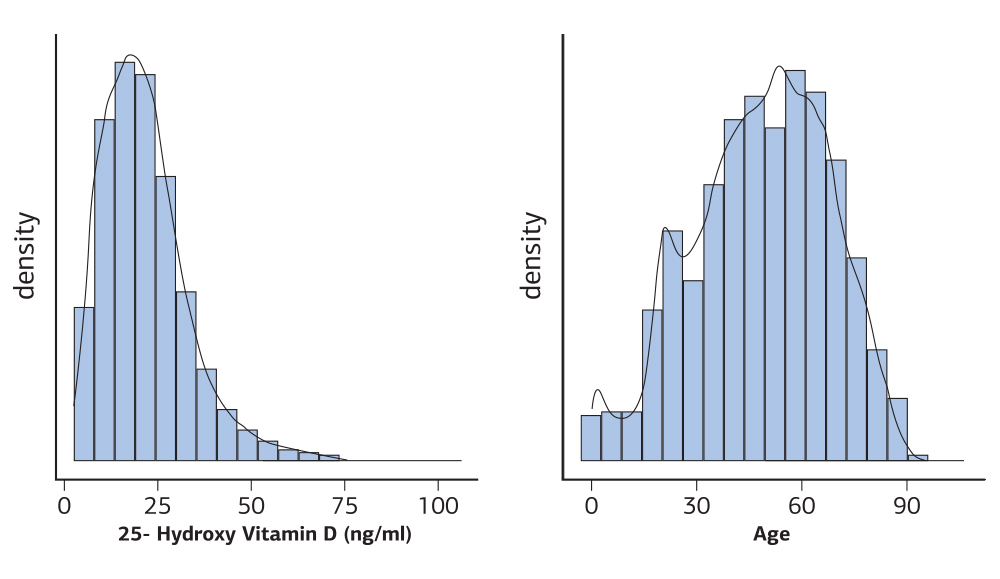
Figure 1. Average 25-Hydroxy Vitamin D levels and age distribution of all participants
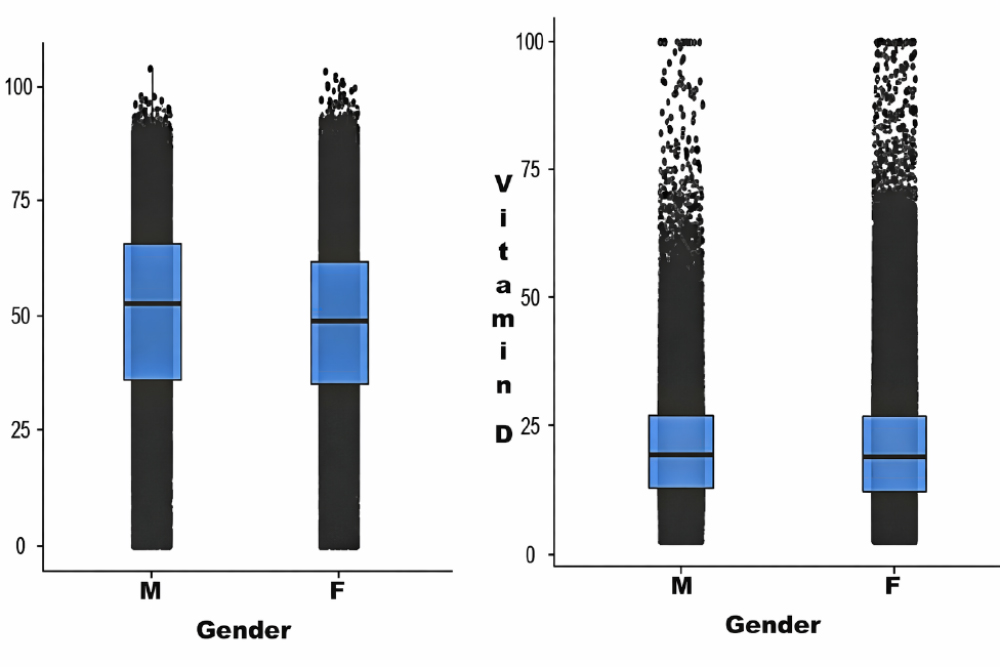
Figure 2. Demographic characteristics and vit d distribution by gender box-plot and age-gender box-plot
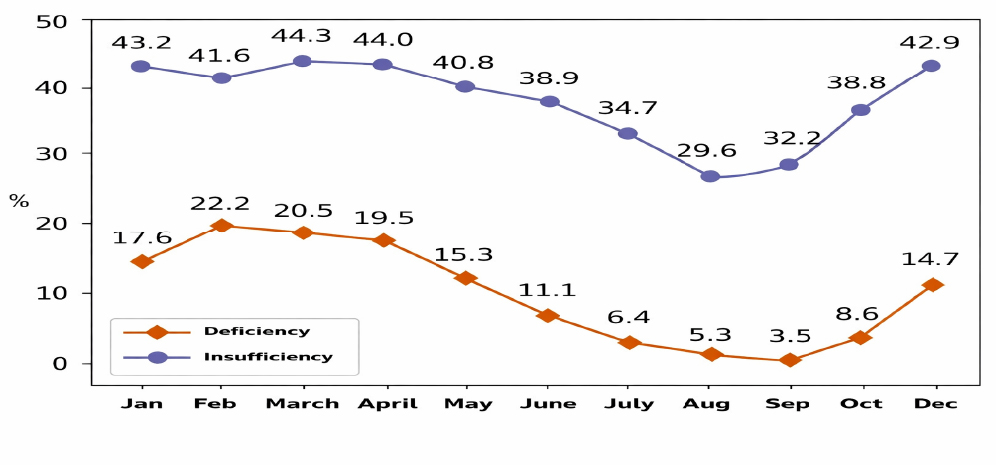
Figure 3. Comparison of 25-Hydroxy Vitamin D deficiency and insufficiency rates by month for all years
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Süheyl Uçucu, Talha Karabıyık, Tarkan Yazıcı. Evaluation of the change of vitamin D deficiency by age, gender, season, and years: a report from west of Turkey. Ann Clin Anal Med 2026;17(2):102-105
- Received:
- September 29, 2025
- Accepted:
- November 18, 2025
- Published Online:
- November 6, 2025
- Printed:
- February 1, 2026