
Assessing kidney and collecting system in patients with ureter stone with statistical shape analysis
Shape analysis in patients with ureter stone
Authors
Abstract
**Aim*
Despite semi-rigid ureteroscopy being the standard treatment for ureteral stones, it is hard to understand whether the treatment has reached success mainly in an early period. It This study aimed to investigate the shape differences in the CT images of kidneys and collecting systems compared between preoperative and postoperative periods terms.
MethodsKidney and collecting system CT images for both terms were evaluated with statistical shape analysis to detect any morphological changes.
ResultsHigh levels of kidney deformations were observed at the medial point of the superior segment and the extremitas superior. For the collecting system, a high level of deformation was is seen in the area around the hilum renal inferior. The two periods have no significant shape difference between the kidney and the collecting system.
ConclusionThe most significant aspect of this study is the quantitative quantitatively demonstration, for the first time, of the shrinking observed in the kidney and collecting systems following treatment for ureteral stones. Our method gives objective and qualitative results by making appropriate landmarks landmarking on the CT image by a physician familiar with the renal anatomy. This new method can be used to follow up stone-induced obstruction due to its ease of application and objective results.
Keywords
Introduction
Semi-rigid ureteroscopy is the standard treatment for ureteral stones. Although it is known as the most effective treatment method for patients with ureteral stones, it is hard to understand whether the treatment has reached success, mainly in an early period. Ureteral stone patients account for about 70% of those treated for stone disease.1 In the management process of the patients with ureteral stone, the aim is to protect the kidney from possible morbidities and make the collecting system stone-free. Hydronephrosis is seen in 92-94% of the patients with ureteral stones.2 When the obstructing ureter stone occurs, it first causes the collecting system pressure to increase and causes dilatation of the renal pelvis and calyces and stretching of the renal capsule. Peristalsis is subsequently disrupted, and collecting system pressure increases further, resulting in renal failure. Dilatation in the collecting system and blunting of the papillary tips are present 42 hours after the onset of obstruction.3 The kidney size expands and shows a cystic appearance compared to the normal opposite side kidney after 6 weeks of obstruction.4 Drainage can be provided temporarily by percutaneous nephrostomy or ureteral stents that are similar in effect and complication.5 However, the primary treatment is to eliminate the cause of obstruction. Delay of drainage can lead to fever, infection, and renal failure. Studies have shown that one-third of patients with unilateral stone-induced obstruction lasting more than 4 weeks have irreversible renal injury.6
The severity of obstruction is a determines determinant of both kidney function loss and stone management.3,7 After hydronephrosis has been is eliminated, the damage progression is prevented, and the kidney starts to function again. Therefore, even if there are is no signs of pain or infection, hydronephrosis must be treated.7
It is generally accepted that hydronephrosis regresses and kidney size decreases after ureteral stone treatment. Hydronephrosis regression and kidney shrinkage may indicate be used as an indicator of the resolution of the obstruction after adequate treatment. With the decline in hydronephrosis, it is evident can be seen that the patient is steering clear of progressive kidney damage caused by obstruction. However, this decline has been demonstrated using the grading systems described in the imaging methods. Moreover, to the best of our knowledge the results have yet to be demonstrated quantitatively. to the best of our knowledge. We believe think the decrease in hydronephrosis and kidney sizes should be demonstrated objectively and quantitatively after ureteral stone treatment. Many studies in the field of medicine consider the geometrical properties of organs or organisms, by taking its geometrical properties into and morphometric methods are frequently preferred for examining the structures and geometrical properties of organ-related diseases.8,9,10,11 Morphometric studies have been performed on kidneys, but modeling is mainly aimed at applying segmentation to various imaging methods.12,13,14 Studies have been carried out on with the morphometric character of the kidney tumor or infundibulopelvic angle calculation to decide the treatment method for the tumors or lower pole stones.15,16 Studies using statistical shape analysis are new to the literature, and the only study with kidney shape probabilistic occupant models belongs to Yates and colleagues.17
Along with the advances in imaging technology and software that enables this technology to be integrated into medicine, geometric change in the shape of the organ or structure of interest can be analyzed using key points called landmark, which have anatomical significance. It is possible to work with geometric shapes by taking the coordinates of the landmarks as the variables in the figure from the measurements taken from the organisms. Statistical shape analysis is a modern geometric morphometric method that uses the shape of organs or organisms as input data.18 Statistical shape analysis also stands out as an auxiliary tool that allows the interpretation of structural differentiation in the relevant organ, by considering the changes in shape.
We hypothesized that the collecting system and kidney sizes shrank shrink after ureteral stone treatment and that this shrinkage could be shown quantitatively with landmark-based geometric analysis. In this study, we aimed to compare similar areas in at CT images taken from the pre- and post-operated patients with ureterolithiasis and thus to show whether there is a significant decline as expected.
Materials and Methods
This study used the coronal abdominal CT scans of 17 (12 male, 5 female) patients with ureteral stones with a mean age of 69.2 ± 6.9. Six of the 17 patients’ CT scans were of the right and 11 were of the left kidney. The non-contrast CT scans of patients admitted to the Zonguldak Ataturk State Hospital Urology Clinic were evaluated retrospectively between from December 2019 to and March 2020. Patients who underwent semirigid ureterorenoscopy due to proximal ureteral stones were selected. separated. Only completely stone-free patients without any ureteral catheter after semirigid URS were included in the study. Among patients whose images could be accessed, those patients with anatomic renal malformations, previous kidney surgery, and accompanying kidney stones were excluded. The same surgeon operated on all patients after they received receiving general anesthesia. Then, a 9.5Fr semi-rigid ureteroscope [Karl Storz, Tuttlingen, Germany] and a Holmium YAG laser [SphinX 30 litho, holmium-YAG laser, LISA Laser Products–GmbH, Germany] were was used in the lithotomy position. A gGrasping forceps were was used for extracting fragments. Non-contrast CT scans were obtained one month before surgery and on the 30th day postoperatively. All CT imaging examinations were performed on a 16-slice SOMATOM Sensation CT scanner.[Siemens AG, Forchheim, Germany]
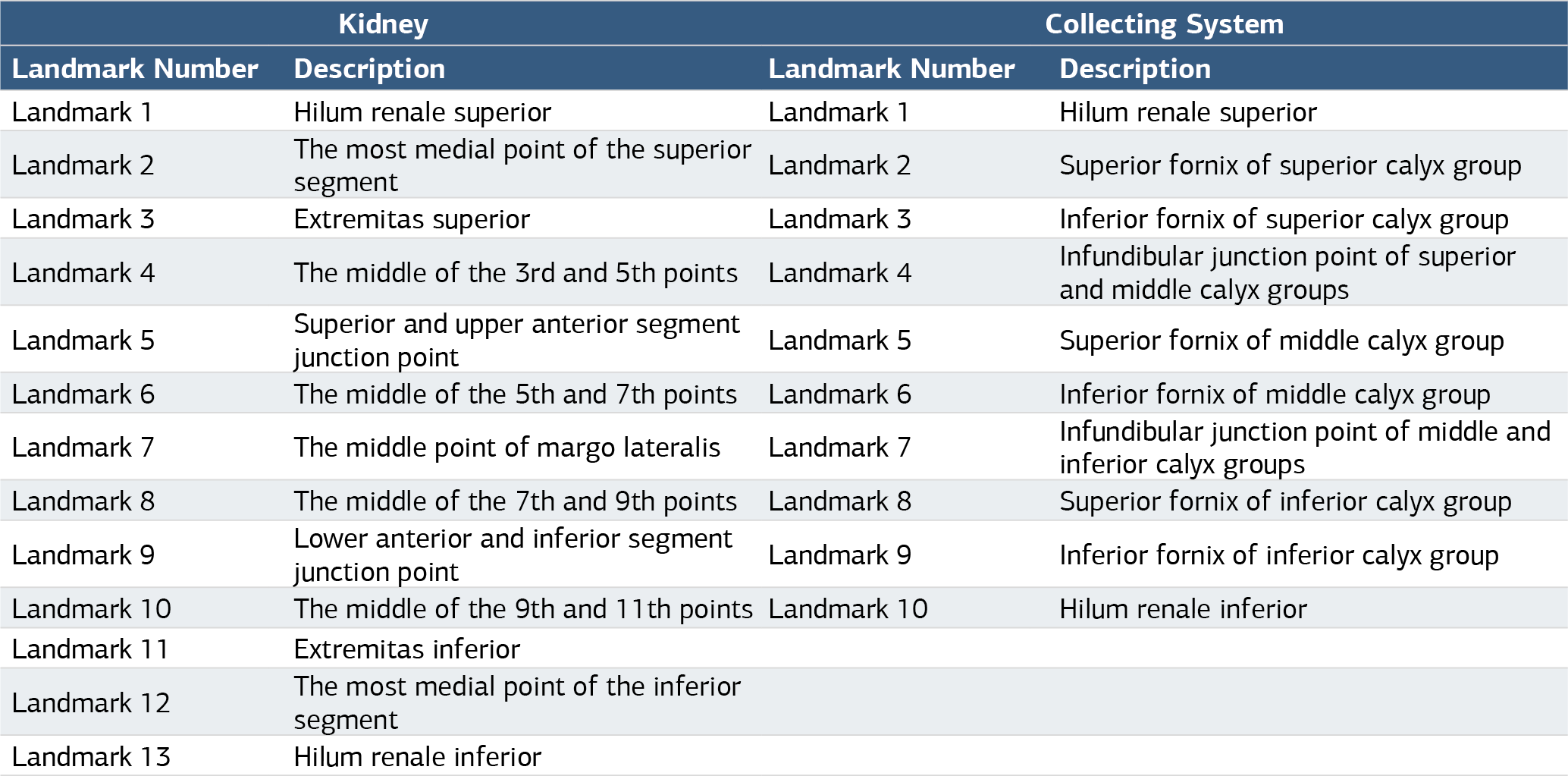
Collection of Two-Dimensional LandmarksData of the regions marked in the kidney and collecting system were collected from two-dimensional digital images. In each image, markings were made in the middle section of the kidney in the coronal plane. Thirteen landmarks for the kidney and ten landmarks for the collecting system.(Table 1) were considered from the image corresponding to the coronal plane and marked using TPSDIG version 2.04 software. The landmarks were chosen based on reliability and anatomical coverage to maximize the description of the kidney and collecting system. description. Mirror images of six right kidney images were taken and analyzed on the same plane.
Geometric Morphometric AnalysisStatistical Shape AnalysisStatistical shape analysis of the pre- and post-treatment kidney and collecting system images of 17 patients was performed. The Generalized Procrustes analysis was used to obtained the mean kidney and collecting system shapes in pre- and post-treatment phases and the related tangent coordinates. Procrustes analysis is the an approach that obtains the minimum sum of squared differences between the landmarks.19 Principal coordinate analysis (PCoA), a type kind of ordination method also known as metric multidimensional scaling, was applied to tangent coordinates derived from the Procrustes analysis. The PCoA routine finds the eigenvalues and eigenvectors of a matrix containing the distances or similarities between all landmark points. Euclidean distance is used in PCoA. The Eigenvalues were computed to measure the variance accounted for by the corresponding eigenvectors (coordinates). The percentages of variance accounted for by these components were are also reported. After that, the classification and changes of patients were examined for pretreatment and post-treatment time points using PCoA. The shape deformation of the kidney and collecting system from the pre- to post-treatment phases was evaluated using the thin plate spline (TPS) method, derived from a mathematical model used in computer graphics and applied to morphometrics by Bookstein.20 The points exhibiting the greatest enlargements or reductions, labeled as deformations were established through the TPS analysis.
Ethical ApprovalThis study was approved by the Ethics Committee of Zonguldak Bulent Ecevit University (Date: 08.07.2020, Decision No: 2020/14-11).
Statistical AnalysisData regarding sex are presented as frequency (%), and those data for age are presented as mean and standard deviation values. For statistical analysis, R 3.5.1, PAST 3.0 and SPSS 21 softwares were used.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Figure 1 shows the combined Procrustes mean shapes for the kidney and collecting system. Procrustes mean shapes (Figure 2a) were obtained as a result of landmark markings from pre- and post-treatment periods of the kidney. PCoA was applied to the tangent coordinates obtained after the Procrustes analysis. PCoA of the preop and postop terms showed a variance explanation rate for the first two coordinates (45.70% and 15.30%, respectively) considered in the study group of 61%.[Figure 2b] The convex hulls on the scatterplot indicate that the patients did not significantly differ in the pre- and post-treatment periods. TPS analysis was also performed using mean shapes obtained from the Procrustes analysis. The A high level of deformations for in the kidney from pre- to post-treatment term observed in the TPS graphic.[Figure 2c] When the figure is examined, it is seen that in the area including the most medial point of the superior segment (Landmark 2) and extremitas superior (Landmark 3), an expansion occurred in the post-treatment period compared to the pre-treatment period. In addition to this, while the general shape of the kidney is determined to be have shrunk compared to the preoperative period, except for the area of landmarks 2 and 3, it is seen that the region where the shrinkage is observed at the highest level occurs in the region including the middle of the 9th and 11th points (Landmark 10) and extremitas inferior (Landmark 11).
Procrustes mean shapes (Figure 3a) were obtained as a result of landmark markings from the pre-treatment and post-treatment periods of the collecting system. PCoA was applied to the tangent coordinates obtained after the Procrustes analysis. PCoA of the preop and postop terms showed a variance explanation rate for the first two coordinates (43.15% and 20.56%) considered in the study group of 63.71%.[Figure 3b] The convex hulls on the scatterplot indicate that the patients did not significantly differ in the pre-treatment and post-treatment periods. TPS analysis was also performed using mean shapes obtained from the Procrustes analysis. The A high level of deformation in for the collecting system from pre-treatment to post-treatment term was observed in the TPS graphic.[Figure 3c] When the figure is examined, it is seen that in the area around the hilum renale inferior (Landmark 10), an expansion occurred in the post-treatment period compared to the pre-treatment period. In addition to this, while the general shape of the collecting system is determined to have be shrunk compared to the preoperative period, except for the area around landmark 10, it is seen that the region where the shrinkage is observed at the highest level occurs in the regions mainly including inferolateral part of the collecting system as hilum renale superior (Landmark 1) and superior fornix of superior calyx group (Landmark 2), superior fornix of middle calyx group (Landmark 5) and inferior fornix of middle calyx group (Landmark 6), infundibular junction point of middle and inferior calyx groups (Landmark 7) and superior fornix of inferior calyx group (Landmark 8), superior fornix of inferior calyx group (Landmark 8) and inferior fornix of inferior calyx group (Landmark 9).
Discussion
In this study, we have shown for the first time, that the size of the kidney and collecting system shrank quantitatively after ureteral stone treatment. In addition to the general changes, the landmark-based shape analysis approach showed us the changes on a regional basis. Although there is no statistical difference between the mean shapes before and after the treatment, kidney and collecting system shrinkage were was demonstrated in the deformation graphs. As a result of both analyses, it was found that the kidney showed the most significant change in the inferomedial part after the obstruction resolved. In addition to the general shrinkage in the figures, a slight expansion was found in the superomedial part of the kidney and the hilum renal area of the collecting system. It is noteworthy that the area in where which the enlargement is detected in the kidney is closest to the section of the collecting system that shows the most shrinkage, and the area where the enlargement in the collecting system is located is the region where the kidney shows the most shrinkage. These expansion areas may have appeared secondary to the deformation caused by the intense shrinkage regions.
The kidney is surrounded by the Gerota’s fascia like a natural anatomic barrier, which keeps the kidney immobilized and prevents the spread of perirenal fluid, hematoma, or infection. This fascia envelops the kidney from all sides except the inferior part. The two fascia leaves do not conjunct at the lower part of the kidney, which where remains are uncovered.21 The most shrinking areas of the kidney and collecting system that shrink the most are located in the inferior part due to the anatomy of the Gerota’s fascia, which that does not cover the lower kidney.
Limitations
Our study has some limitations. Firstly, the retrospective structure of the study and the low number of cases evaluated were significant drawbacks. Furthermore, the anatomical shape differences between the kidneys on both sides were not considered when mirroring the images. In studies to be conducted with more cases, the difference in mean shapes can be reported more significantly. This study showed shrinkage in the kidney and collecting system after ureteral stone treatment. To the best of our knowledge, this is the first study to show that pre- and post-treatment kidney and collecting system shapes of patients with ureteral stones can be compared using the landmark-based geometric morphometric method by considering the topographic distribution. We hope that the results obtained from this study will serve as a guide for to future clinical studies by demonstrating localized variations in the components of the kidney and collecting system.
Conclusion
As far as we know, no studies in the literature focus on kidney size after ureteroscopy. The change in collecting system dimensions after ureteroscopy has been revealed before. However, it has yet to be demonstrated using a as landmark-based or quantitative approach. quantitatively. Sarıca et al. showed that hydronephrosis levels decreased in patients operated on for ureteral stones. However, they only compared this to the degree of hydronephrosis.22 After ureteroscopy, Chen et al. showed that hydronephrosis regressed in groups with and without DJ stent. They also classified made classification patients as having hydronephrosis and no hydronephrosis.23 The results of both studies are presented given subjectively. Furthermore, unlike our study, Tahanaj M. et. al. studied on association of kidney shapes with via disease and anthropometric factors and found that kidney shape has a statistically significant association with chronic kidney disease, type-2 diabetes and hypertension.24 Our method gives objective and qualitative results by making appropriate landmarks landmarking on the CT image by a physician familiar with the renal anatomy. This new method can be used to follow up on stone-induced obstruction due to its ease of application and objective results.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CT: Computed tomography
PCoA: Principal coordinate analysis
TPS: Thin-plate spline
URS: Ureterorenoscopy
References
-
Scales CD, Curtis LH, Norris RD, et al. Changing gender prevalence of stone disease. J Urol. 2007;177(3):979-982. doi:10.1016/j.juro.2006.10.069
-
Xafis K, Thalmann G, Benneker LM, et al. Forget the blood, not the stone! Microhaematuria in acute urolithiasis and the role of early CT scanning. Emerg Med J. 2008;25(10):640-644. doi:10.1136/emj.2006.043703
-
Meldrum KK. Pathophysiology of urinary tract obstruction. In: Wein AJ, Kavoussi LR, Partin AW, Peters CA, eds. Campbell-Walsh Urology. 11th ed. Elsevier; 2016:1097.
-
Ladefoged O, Djurhuus JC. Morphology of the upper urinary tract in experimental hydronephrosis in pigs. Acta Chir Scand Suppl. 1976;472:29-35.
-
Pearle MS, Pierce HL, Miller GL, et al. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998;160(4):1260-1264. doi:10.1097/00005392-199810000-00013
-
Holm-Nielsen A, Jørgensen T, Mogensen P, Fogh J. The prognostic value of probe renography in ureteric stone obstruction. Br J Urol. 1981;53(6):504-507.
-
Leavitt DA, de la Rosette JJMCH, Hoenig DM. Strategies for nonmedical management of upper urinary tract calculi. In: Wein AJ, Kavoussi LR, Partin AW, Peters CA, eds. Campbell-Walsh Urology. 11th ed. Elsevier; 2016:1250.
-
Taskapilioglu MO, Ocakoglu G, Kaya S, Baykal D. Statistical shape analysis of trigonocephaly patients. Childs Nerv Syst. 2020;36(2):379-384.
-
Ocakoglu G, Baykal D, Altunyuva O, Taskapilioglu MO, Yilmazlar S. Statistical shape analysis of cerebellum in patients with Chiari malformation. J Craniofac Surg. 2019;30(6):1683-1685. doi:10.1097/scs.0000000000005505
-
Ocakoglu G, Taskapilioglu MO, Ercan I, et al. Statistical shape analysis of temporal lobe in mesial temporal sclerosis patients. Acta Neurochir (Wien). 2015;157(11):1897-1903. doi:10.1007/s00701-015-2555-9
-
Ocakoglu G, Ozdemir ST, Ercan I, Etoz A. The shape of the external human ear: a geometric morphometric study. Turkiye Klinikleri J Med Sci. 2013;33(1):184-190.
-
Cerrolaza JJ, Safdar N, Peters CA, Myers E, Jago J, Linguraru MG. Segmentation of kidney in 3D-ultrasound images using Gabor-based appearance models. In: 2014 IEEE 11th International Symposium on Biomedical Imaging (ISBI). IEEE; 2014:633-636. doi:10.1109/isbi.2014.6867950
-
Tsagaan B, Shimizu A, Kobatake H, Miyakawa K. An automated segmentation method of kidney using statistical information. Lect Notes Comput Sci. 2002;2488:556-563. doi:10.1007/3-540-45786-0_69
-
Adams F, Qiu T, Mark A, et al. Soft 3D-printed phantom of the human kidney with collecting system. Ann Biomed Eng. 2017;45(4):963-972. doi:10.1007/s10439-016-1757-5
-
Simmons MN. Morphometric characterization of kidney tumors. Curr Opin Urol. 2011;21(2):99-103. doi:10.1097/mou.0b013e32834208d6
-
Dresner SL, Iremashvili V, Best SL, Hedican SP, Nakada SY. Influence of lower pole infundibulopelvic angle on success of retrograde flexible ureteroscopy and laser lithotripsy for the treatment of renal stones. J Endourol. 2020;34(6):655-660. doi:10.1089/end.2019.0720
-
Yates KM, Untaroiu CD. Finite element modeling of the human kidney for probabilistic occupant models: statistical shape analysis and mesh morphing. J Biomech. 2018;74:50-56. doi:10.1016/j.jbiomech.2018.04.016
-
Kaya MO, Ozturk S, Ercan I, Gonen M, Erol FS, Kocabicak E. Statistical shape analysis of subthalamic nucleus in patients with Parkinson disease. World Neurosurg. 2019;126. doi:10.1016/j.wneu.2019.02.180
-
Dryden IL, Mardia KV. Statistical Shape Analysis: With Applications in R. 2nd ed. John Wiley & Sons; 2016:125. doi:10.1002/9781119072492
-
Bookstein FL. Principal warps: thin-plate splines and the decomposition of deformations. IEEE Trans Pattern Anal Mach Intell. 1989;11(6):567-585. doi:10.1109/34.24792
-
Elkoushy MA, Andonian S. Surgical, radiologic, and endoscopic anatomy of the kidney and ureter. In: Wein AJ, Kavoussi LR, Partin AW, Peters CA, eds. Campbell-Walsh Urology. 11th ed. Elsevier; 2016:1250.
-
Sarica K, Tarhan F, Erdem K, Sevinc AH, Guzel R, Eryildirim B. Functional and morphological recovery of solitary kidneys after drainage: double-J stent placement vs emergency ureteroscopy; which one is reasonable? Urolithiasis. 2018;46(5):479-484. doi:10.1007/s00240-017-1005-y
-
Yung-Tai C, Jun C, Wai-Yan W, Stephen SY, Cheng-Hsing H, Chung-Cheng W. Is ureteral stenting necessary after uncomplicated ureteroscopic lithotripsy? A prospective, randomized controlled trial. J Urol. 2002;167(5):1977-1980.
-
Thanaj M, Basty N, Cule M, Sorokin EP, Whitcher B. Kidney shape statistical analysis: associations with disease and anthropometric factors. BMC Nephrol. 2023;24(1):362. doi:10.1186/s12882-023-03407-8
Figures

Figure 1. The combined pre and post-treatment mean shapes for the kidney and collecting system

Figure 2. (a: upper left) Procrustes mean shapes for the pretreatment and postop treatment phases kidneys of patients, (b: upper right) scatter graphs with 95% confidence ellipses and convex hulls obtained by principal coordinate analysis results of patients (•: pretreatment; x: post treatment), (c: bottom) a thin-plate spline demonstrating the kidney shape deformation for post treatment term compared to pre-treatment

Figure 3. (a: upper left) Procrustes mean shapes for the pretreatment and postop treatment phases of collecting systems of patients, (b: upper right) scatter graphs with 95% confidence ellipses and convex hulls obtained by principal coordinate analysis results of patients(•: pretreatment; x: posttreatment), (c: bottom) a thin-plate spline demonstrating collecting systems shape deformation for post treatment term compared to pretreatment
Tables
Table 1. Definitions of landmarks used in the present study
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mustafa Çağatay Büyükuysal, Engin Denizhan Demirkıran, Gökhan Ocakoğlu. Assessing kidney and collecting system in patients with ureter stone with statistical shape analysis. Ann Clin Anal Med 2025;16(5):315-319. doi:10.4328/ACAM.22002
- Received:
- October 17, 2023
- Accepted:
- September 2, 2024
- Published Online:
- December 12, 2024
- Printed:
- May 1, 2025