
Clinical characteristics of patients with adrenocortical carcinoma: a single center experience
Adrenocortical carcinoma
Authors
Abstract
AimAdrenocortical carcinomas (ACC) are rare tumors with an aggressive course. A better understanding of the molecular pathogenesis may lead to the development of more effective therapies in the future. However, there are limited effective treatment options currently.
This study aimed to retrospectively investigate the clinical characteristics of patients diagnosed with adrenocortical carcinoma who were followed at Ankara Numune Training and Research Hospital and Ankara City Hospital between November 2002 and January 2022.
MethodsThe medical records of patients diagnosed with ACC and followed at Ankara Numune Education and Research Hospital and Ankara City Hospital between November 2002 and January 2022 were retrospectively reviewed. Metastatic and non-metastatic patients were compared regarding demographic data, clinical parameters, and survival.
ResultsTwenty-five patients with a median age of 45 (17-75) were included. Abdominal pain (36%) was the most common presenting symptom. The median tumor diameter was 12 (2-27) cm. In the 18 patients who were initially non-metastatic, the median disease-free survival (DFS) was 57.3 months (95% CI: 15.7- 98.9). The median progression-free survival (PFS) for metastatic patients was 8.3 months (95% CI 0-24.6). The overall survival (OS) in patients with metastasis at diagnosis was 16.1 months, while in those without metastasis, it was 98.1 months (p<0.0001).
ConclusionAdjuvant mitotane therapy is an option for high risk cases. Mitotane plus chemotherapy combinations are the current treatment options for metastatic patients. However, further research is needed to develop treatment guidelines due to the disease’s rarity
Keywords
Introduction
Adrenocortical carcinomas (ACC) are rare tumors with an aggressive course and limited effective treatment options for advanced stages. According to the Surveillance, Epidemiology, and End Results (SEER) database, the annual incidence in the United States is 0.72 cases per million, accounting for 0.2% of all cancer deaths.1 The frequency of ACC follows a bimodal distribution, with peaks in childhood and the 5th-6th decades, and the mean age of occurrence is 46.2 The incidence is slightly higher in females, with a ratio of 1.5-2.5/1 compared to males.3
Clinically, patients commonly (40-60%) present with symptoms related to hormone excess, while non-functional ACCs typically manifest with symptoms related to large masses, such as abdominal pain and early satiety.2,4
In terms of diagnosis, most cases of adrenocortical carcinoma present with large tumor sizes, with a mean tumor size ranging from 10 to 13 cm.2,5 A tumor size of less than 6 cm is detected in 9-14% of cases, while tumors smaller than 4 cm are found in 3%.5,6 Staging can be performed using the World Health Organization (WHO) 2004 classification or its Sullivan modification, the American Joint Committee on Cancer (AJCC) Tumor-Node-Metastasis (TNM) staging, or the European Network for the Study of Adrenal Tumors (ENSAT) system.7 While older studies reported higher rates, currently, 25-30% of patients are diagnosed at a metastatic stage, the most common sites of metastasis being the lungs (40-80%), liver (40-90%), and bones (5-20%).8
Complete surgical resection is the only curative treatment.9 For stage 1-3 disease, surgery at an experienced center is the preferred approach 10However, despite complete resection, local recurrence rates of 19-34% were reported. In a series including 3982 patients, the authors noted that 9% underwent R1 while 10% underwent R2 resection.11 Mitotane is the only FDA-approved agent for ACC treatment, and adjuvant mitotane treatment showed benefits regarding relapse-free survival (RFS) and overall survival (OS) in patients with stage 1-3 ACC.12 Therefore, in high-risk cases with a Ki67 value of >20%, a history of incomplete resection, and suspicion of tumor spread due to intraoperative capsular rupture, adjuvant mitotane is recommended.13
In a retrospective study including 31 patients, it was reported that adding platinum-based chemotherapy to adjuvant mitotane led to a significant increase in RFS and OS in the patients with a Ki67 value >20%, extensive vascular invasion, or tumor thrombus in the vena cava.14 Also, combinations of mitotane and platinum-based chemotherapy are commonly used for unresectable, recurrent, and metastatic ACC patients. The First International Randomized Trial in Locally Advanced and Metastatic Adrenocortical Carcinoma Treatment (FIRMACT) study, which compared etoposide, doxorubicin, cisplatin, mitotane [EDPM] combination with streptozotocin-mitotane combination in metastatic ACC patients concluded that the EDPM combination demonstrated a superior objective response rate.15 In this trial, the EDPM arm showed better progressionfree survival (PFS), but only by 5 months.
Despite these findings, due to the paucity of data in the literature, further research is needed regarding the treatment of ACC.
This study investigated the clinical characteristics of patients diagnosed with ACC and followed at two tertiary care centers.
Materials and Methods
The medical records of patients diagnosed with ACC and followed at Ankara Numune Training and Research Hospital and Ankara City Hospital between November 2002 and January 2022 were retrospectively reviewed. The survival status of patients no longer under follow-up was checked through the death notification system (DNS) using their national identification numbers. Eastern Cooperative Oncology Group (ECOG) score was used to assess performance status. The demographic and clinical characteristics, including age, gender, initial tumor stage, baseline performance status, tumor size, side (left vs. right), initial symptoms, and data regarding hormonal activity, were collected and comparatively analyzed. In addition, patients who received adjuvant therapy were determined, and DFS was calculated in these cases. Likewise, PFS and OS were calculated in metastatic patients. We analyzed whether age, gender, side of the tumor, tumor size, and the presence of metastasis at the time of initial diagnosis impacted survival.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Bilkent City Hospital (Date: 18.01.2023, Decision No: E2-23-3261).
Statistical AnalysisDescriptive data were given as means and standard deviations, medians, and ranges [minimum-maximum]. Groups were formed based on gender, symptomatology, disease stage, and other clinical features, and differences between these groups were analyzed. The chi-square test, Student’s t-test, Mann-Whitney U test, and ANOVA were used for primary and comparative statistical analyses. Overall survival and diseasefree survival (DFS/PFS) analyses were performed. Kaplan-Meier method was used for survival analyses, including OS, DFS, and PFS. Differences between the groups concerning survival were analyzed using the log-rank test. Cox regression analysis was used to determine factors affecting OS. Hazard ratios and 95% confidence intervals (CI) were calculated. All statistical analyses were performed using the SPSS (Statistical Package for Social Sciences, SPSS v22, IBM, Armonk, NY, US). The level of statistical significance was set at 5%.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
The general characteristics of the patients are displayed in Table 1. A total of 25 patients with a median age of 45 (17- 75) were included. While 60% (n = 15) were female, 40% (n = 10) were male. Abdominal pain was the most common presenting symptom, observed in 36% (n = 9) of the cohort. The median tumor diameter was 12 (2-27) cm, and the tumor was on the left side in 64% (n = 16) of the cases. Hormonal changes were detected in 36% (n = 9) of the patients.
The review regarding initial disease stages revealed that 8% (n = 2) of the patients had stage 1, 48% (n = 12) stage 2, 12% (n = 3) stage 3, and 32% (n = 8) stage 4 disease. Among the 25 patients, 7 (28%) were metastatic at the initial diagnosis, and 6 of these patients received systemic treatment. Among the 18 non-metastatic patients, 7 received adjuvant chemotherapy.
Adjuvant treatment consisted of cisplatin-etoposide in 3 patients and mitotane in 4 patients.
Comparative analyses based on gender showed that hirsutism was more commonly observed in females (27% vs. 0%, p=0.044), while left-sided tumors were significantly more prevalent in males compared to females (90% vs. 47%, p=0.04). There were no other significant differences between female and male patients regarding other parameters (Table 2).
Our retrospective review also revealed that among 18 nonmetastatic patients, 10 (56%) experienced recurrence or metastasis during follow-up, and 9 of these patients received systemic treatment. Among the patients with metastatic disease at diagnosis or those who developed recurrence or metastasis during follow-up and received systemic treatment (15 patients), mitotane was the most commonly preferred agent (33%), followed by the cisplatin-etoposide-mitotane combination (26.7%), and cisplatin-etoposide without mitotane (20%). The CAP (cisplatin-doxorubicin-vincristine) and CAP+mitotane were the other treatment regimens preferred in this cohort.
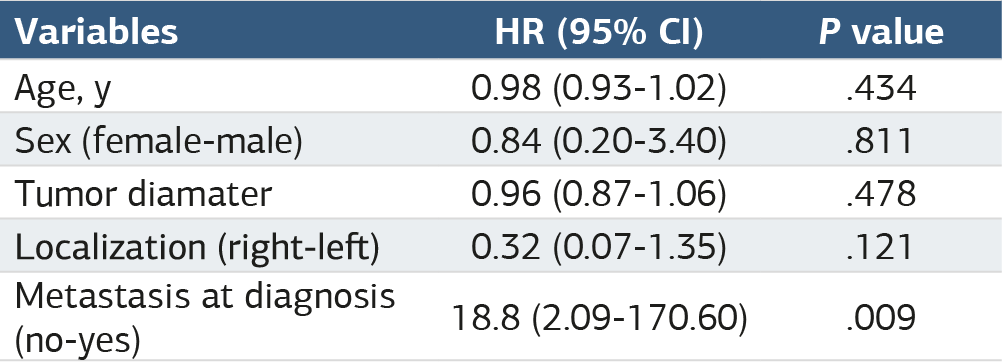
The survival analyses showed that the median OS was 63.7 (95% CI 6.0-121.4) months in the entire group (Figure 1). In the female group, the median OS was 63.7 months, while it was 30.4 months in the male group. However, the difference was not statistically significant. For the 18 patients who were initially non-metastatic, the median DFS was 57.3 (95% CI 15.7- 98.9) months (Figure 2). On the other hand, in the metastatic patients, the median PFS was 8.3 (95% CI 0-24.6) months. The most common sites of metastasis were the liver (n = 4) and lungs (n = 4). In our cohort, the median follow-up duration was 28.4 months, and 9 (36%) died during follow-up. Our analysis also included a search for potential factors affecting OS (Table 3). This analysis included potential factors such as age, gender, tumor diameter, tumor side (right vs left), and metastasis at the initial diagnosis. This analysis revealed that, among these potential factors, only metastasis at diagnosis was significantly associated with shorter OS: While OS was 16.1 months in initially metastatic patients, it was 98.1 months in those who were non-metastatic at the time of initial diagnosis (p<0.0001).
Discussion
In our study, we examined the general characteristics of the patients diagnosed with ACC, a rare and aggressive disease with a poor prognosis.
In the relevant literature, it was reported that the mean patient age was 46.2 We calculated the mean patient age as 45 in our cohort. It was previously reported that ACC was 1.5-2.5 times more frequently diagnosed in women than in men.3,16 In line with this finding, in our study, 60% of the patients were female. Fassnacht et al. noted that the rate of left-sided ACC was 1.2-fold higher than the right-sided disease in their cohort.17 It was denoted that hormonal hypersecretion symptoms are common in ACC.10,12 In our patient group, hormonal hypersecretion was detected in 36% of cases. These findings suggest that all patients should undergo endocrinological assessment before initiation of treatment.
In our cohort, analysis regarding sites of distant metastasis revealed that the most common sites of metastases were the liver and lungs. This finding is also consistent with the literature since the most commonly reported metastatic sites were the liver and lungs, followed by intra-abdominal lymph nodes, adrenal glands, and bones in the existing literature.
Although surgical resection is the primary curative treatment modality in ACC, it is associated with a relatively higher recurrence rate than other common malignancies.18 Due to insufficient evidence-based data regarding adjuvant therapy, clinical decisions on adjuvant mitotane treatment in patients at high risk of recurrence should be made by an individualized approach. In a meta-analysis including 1249 patients, Tang Y. et al. reported that adjuvant mitotane treatment led to an increase in recurrence-free survival and overall survival in patients with ACC.19 On the other hand, the ADIUVO study, which investigated the impact of adjuvant mitotane treatment on DFS in 91 low-risk (stage 1-3, R0 resected, Ki-67<10%) ACC patients, concluded that adjuvant mitotane treatment did not lead to an increase in RFS and OS.20
As per ENSAT guidelines, adjuvant mitotane therapy should be considered in patients with a high risk of recurrence based on disease stage, R0 resection status, Ki-67 value, or mitotic index.14,21 Currently, adjuvant mitotane treatment is recommended for those with Ki-67 values between 10% and 20% or mitotic indices higher than 20 under a 50x magnification and those with an intraoperative capsular rupture. On the other hand, according to the guidelines, in cases with a Ki-67 value of higher than 20%, there is a significant risk of extensive vascular invasion or tumor thrombus in the vena cava, and cytotoxic treatments should be preferred over adjuvant mitotane therapy in these patients. However, the decision should be given by an individualized approach. In our cohort, most of our patients were diagnosed before 2015. Therefore, Ki-67 and mitotic index values were not available for all participants, and these parameters were not used while making decisions regarding patient management.
Some studies on the management of metastatic ACC focused on mitotane monotherapy.22 Although these studies included patients with low tumor burden, they reported a median survival of 6.5 months, similar to untreated patients. Currently, the preferred treatment approach involves combining mitotane with cytotoxic chemotherapy.23 In an in vitro setting, it was demonstrated that mitotane sensitized the human ACC cells to other chemotherapeutic drugs, possibly by acting as an antagonist to multidrug resistance (MDR) proteins. This finding constitutes the rationale for combination therapy.24,25 The First International Randomized Trial in Locally Advanced and Metastatic Adrenocortical Carcinoma Treatment (FIRM-ACT) study compared the combination of etoposide, doxorubicin, cisplatin, and mitotane [EDPM] with streptozotocin and mitotane in metastatic ACC patients.16,17 The EDPM combination showed a superior objective response rate than streptozotocin (23% vs 9%). In this study, the PFS was better in the EDPM arm, albeit by only 5 months.16
In our patient group, only one patient received this combination therapy since most patients were diagnosed before the publication of these reports.16,17 Three patients received cisplatin-etoposide-mitotane, and 2 patients received cisplatinetoposide. The low number of patients makes it difficult to compare these regimens regarding survival. Our analysis revealed that the median OS was 63.7 months for the entire patient group. The relatively longer OS in our cohort compared to the published reports can be because approximately half of our patients were at stage 2.
Limitations
The retrospective single-center design and the small sample size are the main limitations of this study.
Conclusion
In conclusion, ACC is a rare and aggressive disease with limited treatment options, especially in the metastatic stage. For patients who undergo R0 resection, the recurrence risk should be determined. Adjuvant mitotane treatment should be given in high-risk patients. On the other hand, for metastatic ACC patients, EDPM combination therapy should be considered in patients who can tolerate it. Since there is still insufficient data for composing guidelines, further clinical research is needed to arrive at more concrete conclusions.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Waived due to the retrospective study design.Our analysis also included a search for poten
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ACC: Adrenocortical carcinoma
CI: Confidence interval
DFS: Disease-free survival
ECOG: Eastern Cooperative Oncology Group
EDPM: Etoposide, doxorubicin, cisplatin, mitotane
ENSAT: European Network for the Study of Adrenal Tumors
OS: Overall survival
PFS: Progression-free survival
SPSS: Statistical Package for the Social Sciences
References
-
Kebebew E, Reiff E, Duh QY, Clark OH, McMillan A. Extent of disease at presentation and outcome for adrenocortical carcinoma: have we made progress? World J Surg. 2006;30(5):872-878. doi:10.1007/s00268-005-0329-x
-
Fassnacht M, Allolio B. Clinical management of adrenocortical carcinoma. Best Pract Res Clin Endocrinol Metab. 2009;23(2):273-289. doi:10.1016/j.beem.2008.10.008
-
Luton JP, Cerdas S, Billaud L, et al. Clinical features of adrenocortical carcinoma, prognostic factors, and the effect of mitotane therapy. N Engl J Med. 1990;322(17):1195-1201. doi:10.1056/nejm199004263221705
-
Allolio B, Fassnacht M. Clinical review: adrenocortical carcinoma: clinical update. J Clin Endocrinol Metab. 2006;91(6):2027-2037. doi:10.1210/jc.2005-2639
-
Else T, Kim AC, Sabolch A, et al. Adrenocortical carcinoma. Endocr Rev. 2014;35(2):282-326. doi:10.1210/er.2013-1029
-
Egoshi K, Masai M, Nagao K, Ito H. 11-Deoxycorticosterone-producing adrenocortical carcinoma. Urol Int. 1998;61(4):251-253. doi:10.1159/000030341
-
Sturgeon C, Shen WT, Clark OH, Duh QY, Kebebew E. Risk assessment in 457 adrenal cortical carcinomas: how much does tumor size predict the likelihood of malignancy? J Am Coll Surg. 2006;202(3):423-430. doi:10.1016/j.jamcollsurg.2005.11.005
-
Paton BL, Novitsky YW, Zerey M, et al. Outcomes of adrenal cortical carcinoma in the United States. Surgery. 2006;140(6):914-920. doi:10.1016/j.surg.2006.07.035
-
Fassnacht M, Johanssen S, Quinkler M, et al; Adrenocortical Carcinoma Registry Group; European Network for the Study of Adrenal Tumors. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a revised TNM classification. Cancer. 2009;115(2):243-250. doi:10.1002/cncr.24030
-
Allolio B, Hahner S, Weismann D, Fassnacht M. Management of adrenocortical carcinoma. Clin Endocrinol (Oxf). 2004;60(3):273-287. doi:10.1046/j.1365-2265.2003.01881.x
-
Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology clinical practice guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2018;179(4). doi:10.1530/eje-18-0608
-
Zeiger MA, Thompson GB, Duh QY, et al; American Association of Clinical Endocrinologists; American Association of Endocrine Surgeons. American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons medical guidelines for the management of adrenal incidentalomas: executive summary of recommendations. Endocr Pract. 2009;15(5):450-453. doi:10.4158/ep.15.5.450
-
Bilimoria KY, Shen WT, Elaraj D, et al. Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer. 2008;113(11):3130-3136. doi:10.1002/cncr.23886
-
Berruti A, Fassnacht M, Baudin E, et al. Adjuvant therapy in patients with adrenocortical carcinoma: a position of an international panel. J Clin Oncol. 2010;28(23). doi:10.1200/jco.2009.27.5958
-
Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma. N Engl J Med. 2007;356(23):2372-2380. doi:10.1056/nejmoa063360
-
Kimpel O, Bedrose S, Megerle F, et al. Adjuvant platinum-based chemotherapy in radically resected adrenocortical carcinoma: a cohort study. Br J Cancer. 2021;125(9):1233-1238. doi:10.1038/s41416-021-01513-8
-
Fassnacht M, Terzolo M, Allolio B, et al; FIRM-ACT Study Group. Combination chemotherapy in advanced adrenocortical carcinoma. N Engl J Med. 2012;366(23):2189-2197. doi:10.1056/nejmoa1200966
-
Fassnacht M, Libé R, Kroiss M, Allolio B. Adrenocortical carcinoma: a clinician’s update. Nat Rev Endocrinol. 2011;7(6):323-335. doi:10.1038/nrendo.2010.235
-
Glenn JA, Else T, Hughes DT, et al. Longitudinal patterns of recurrence in patients with adrenocortical carcinoma. Surgery. 2019;165(1):186-195. doi:10.1016/j.surg.2018.04.068
-
Tang Y, Liu Z, Zou Z, Liang J, Lu Y, Zhu Y. Benefits of adjuvant mitotane after resection of adrenocortical carcinoma: a systematic review and meta-analysis. Biomed Res Int. 2018;2018:9362108. doi:10.1155/2018/9362108
-
Berruti A, Fassnacht M, Libe R, Lacroix A, Kastelan D, Haak H. First randomized trial on adjuvant mitotane in adrenocortical carcinoma patients: the ADIUVO study. J Clin Oncol. 2022;40(6_suppl):1.
-
Beuschlein F, Weigel J, Saeger W, et al. Major prognostic role of Ki67 in localized adrenocortical carcinoma after complete resection. J Clin Endocrinol Metab. 2015;100(3):841-849. doi:10.1210/jc.2014-3182
-
Hutter AM Jr, Kayhoe DE. Adrenal cortical carcinoma: clinical features of 138 patients. Am J Med. 1966;41(4):572-580. doi:10.1016/0002-9343(66)90219-1
-
Flynn SD, Murren JR, Kirby WM, Honig J, Kan L, Kinder BK. P-glycoprotein expression and multidrug resistance in adrenocortical carcinoma. Surgery. 1992;112(6):981-986.
-
Haak HR, van Seters AP, Moolenaar AJ, Fleuren GJ. Expression of P-glycoprotein in relation to clinical manifestation, treatment and prognosis of adrenocortical cancer. Eur J Cancer. 1993;29A(7):1036-1038. doi:10.1016/s0959-8049(05)80219-9
Figures
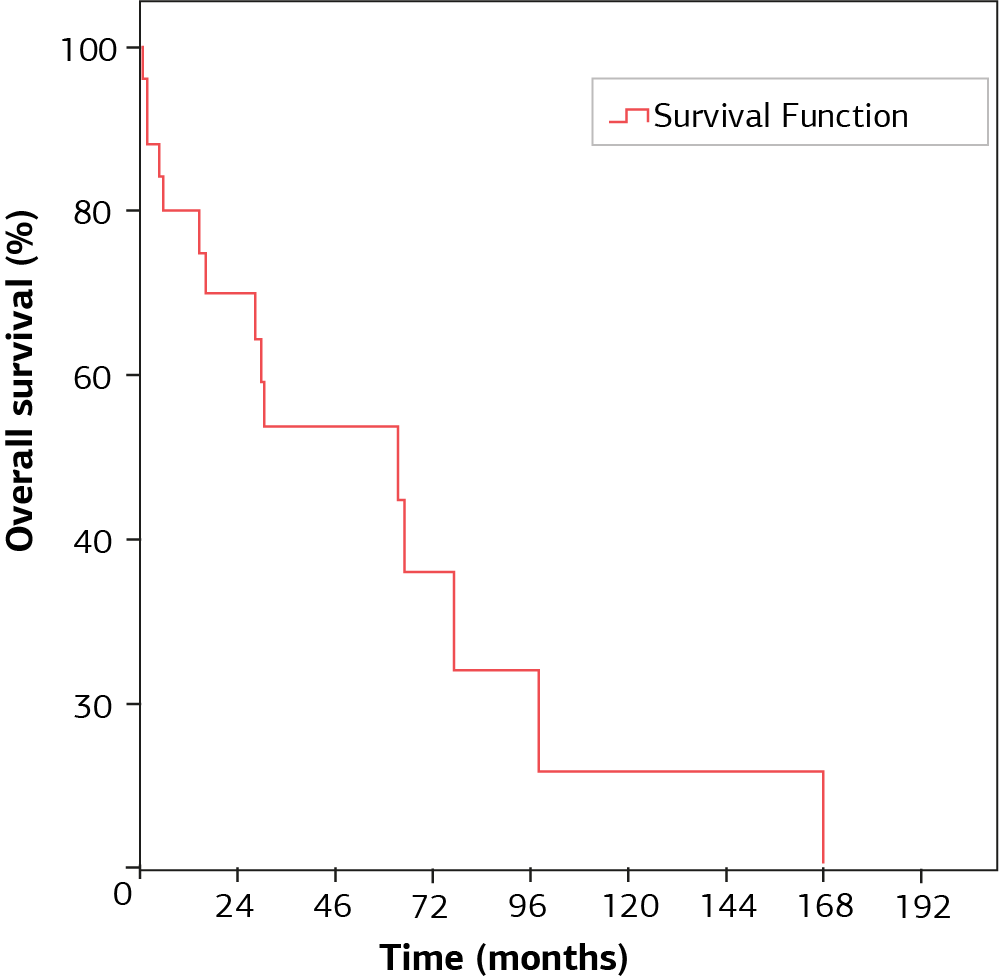
Figure 1. Overall survival of patients

Figure 2. Disease-free survival data of the patients

Figure 3
Tables
Table 1. Demographic and clinical characteristics of the patients
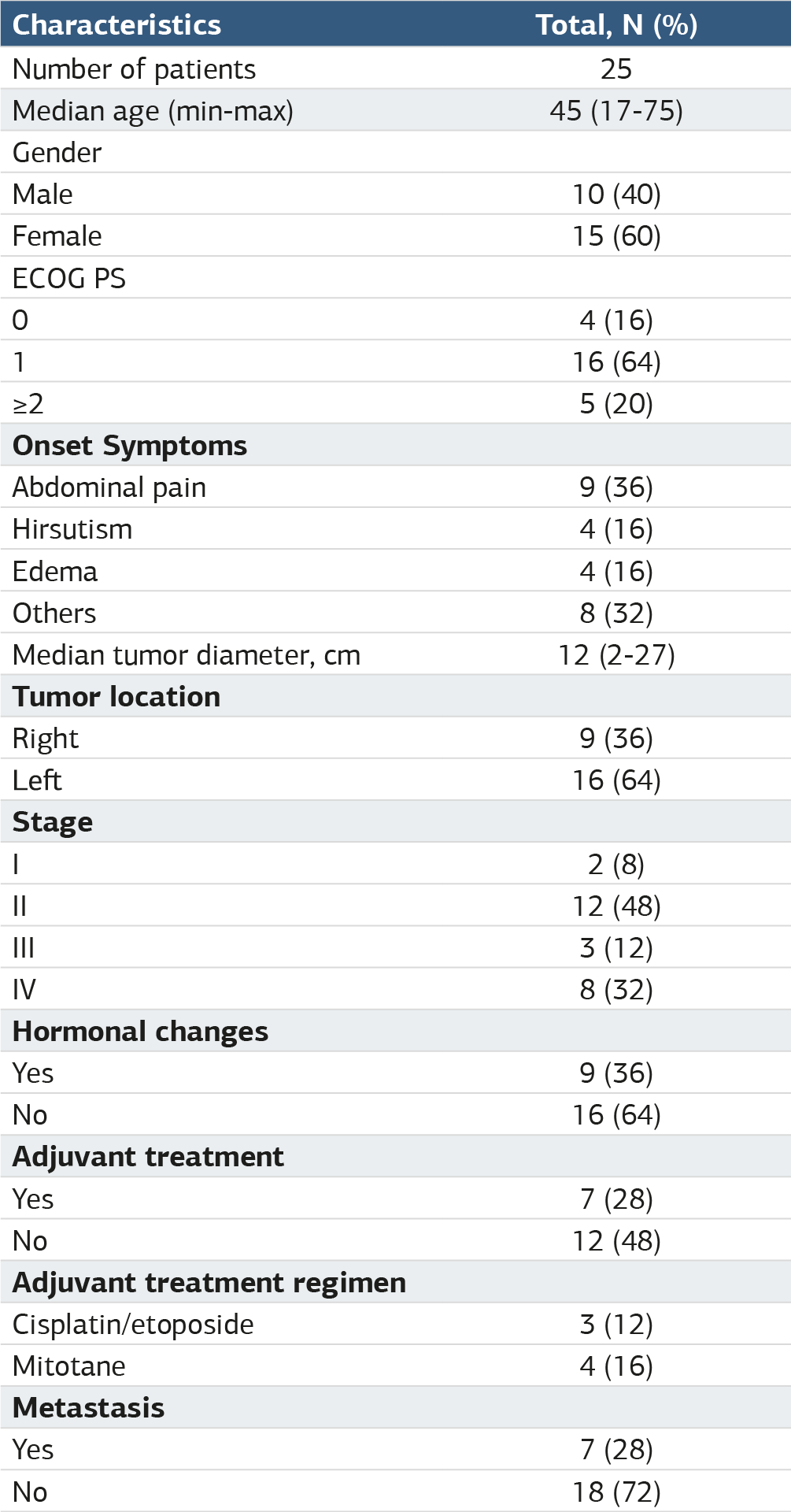
Table 2. Comparison of the demographic and clinical data based on gender

Table 3. Results of the regression analysis regarding overall survival
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Perihan Perkin, Yusuf Acikgoz, Tugba Kos. Clinical characteristics of patients with adrenocortical carcinoma: a single center experience. Ann Clin Anal Med 2025;16(4):232-236. doi:10.4328/ACAM.22055
- Received:
- December 23, 2023
- Accepted:
- February 22, 2024
- Published Online:
- November 30, 2024
- Printed:
- April 1, 2025