
Can pregnancy, delivery, and early neonatal complications be predicted using the ultrasonographically measured first trimester placental volume? aprospective study
Prediction of neonatal complications using ultrasonography
Authors
Abstract
AimWe aimed to determine the relationship between first trimester placental volume and pregnancy, birth, and perinatal complications.
MethodsThis prospective observational study was performed between August 2022 and March 2023 at the Department of Obstetrics and Gynecology at Tekirdağ Namık Kemal University Faculty of Medicine. A total of 82 singleton pregnant women at 11 + 0 to 13 + 6 weeks from the last menstrual date or first trimester ultrasonography (USG) were enrolled.
ResultsThe median age of the patients was 24 (19–35) years. The median placental volume was 22.78 (11.31–35.46) cm3. gestational diabetes mellitus (GDM) developed in nine (11.0%) pregnant women and gestational hypertension (GHT) developed in eight (9.8%). There was a significant positive correlation between the mean placental volume and the maternal weight (r=0.251, p=0.023), gestational age according to the last menstrual period (r=0.572, p<0.001), and gestational age according to USG (r=0.735, p<0.001). There was no significant relationship between the mean placental volume and the birth type (p=0.540), cesarean section indication (p=0.146), admission to the neonatal intensive care unit (ICU) (p=0.733), indication for ICU admission (p=0.520), GDM (p=0.563), and GHT (p=0.527).
ConclusionAlthough the first trimester placental volume was positively related to maternal weight and gestational age, it was not associated with other variables. However, there is insufficient evidence regarding the role of first trimester placental volume in predicting problems related to pregnancy, delivery, and the early neonatal period.
Keywords
Introduction
The human placenta is a vascular organ that is a combination of embryo/fetal and maternal tissue, to which the fetus is connected by the umbilical cord. The human placental villi begin to emerge 7 to 8 days after fertilization, and a complete placenta is formed by the 3rd month of pregnancy. The placenta grows gradually as the pregnancy progresses.1,2 Transportation and endocrine and metabolic functions of the placenta are the main determinants of fetal nutrition and homeostasis.2,3,4 It ensures that oxygen and nutrients are delivered to the fetus and waste products are removed to maintain fetal growtH.1 Adequate blood flow from the placenta is an important determinant of fetal development and maternal health.2 Considering these factors, placental problems are the primary cause of common pregnancy disorders, including recurrent miscarriages, fetal growth restriction, preeclampsia, and stillbirth.1,5 The health, functions, and capacity of the placenta are related to its weight. The placental weight at birth is positively related to the birth weight.6 Since the 1970s,7 two-dimensional (2D) ultrasonography (USG) has been used to evaluate the placental size during early pregnancy. Several studies have revealed that low placental volume in the first trimester is associated with small for gestational age (SGA) fetus, fetal growth restriction, preeclampsia, gestational diabetes mellitus (GDM), and gestational hypertension (GHT).8,9,10,11,12 Problems during pregnancy and the early neonatal period create a serious burden on the health system in addition to negatively affecting maternal and infant health. Detection and prevention of possible complications in early pregnancy are necessary to reduce maternal and fetal mortality and morbidity. Demonstrating that the placental thickness, width, and volume on USG in the first trimester can predict the possible obstetric, fetal, and perinatal risks will provide a proactive approach to managing complications. However, the number of studies on this subject is limited. Thus, we aimed to determine the relationship between first trimester placental volume and pregnancy, birth, and perinatal complications.
Materials and Methods
82 participants were included in the study. The sample size of this study was determined based on the study by Soongsatitanon et al.9 Accordingly, a 95% confidence interval (CI) and 95% power were obtained for a sample calculation of 82 participants. G-Power (version 3.1.9.7) was used to calculate the power of the sample size. This prospective observational study was performed between August 2022 and March 2023 at the Department of Obstetrics and Gynecology at Tekirdag Namık Kemal University.
Measuring the Placental VolumePlacental volume was measured using a 2D transabdominal USG device (DC-8 Exp; Mindray, Shenzhen, China) and transabdominal convex probe (C5-2s probe; Mindray, Shenzhen, China) in patients during their 11 + 0 to 13 + 6 weeks of gestation, by a single operator blinded to all the clinical data. Volumetric imaging of the placenta was performed with the pregnant woman lying in the semi-recumbent position. After confirming the viability and determining the position of the placenta, optimal probe placement was determined for performing a 2D scan of the entire placenta. This was generally chosen as a cross-sectional plane near the placental center. The width, height, and thickness of the placenta were measured. The mean placental volume was estimated using the following convex–concave shell formula: V = (πT/6) ×[4H(W − T) + W(W − 4T) − 4T2], where V = volume; W = maximal width; H = height at maximal height; and T = thickness at maximal height.13 To calculate the placental volume, it is very important to identify the two ends of the placenta, the width of which is used in the calculation process. Another thing to consider is that the interface of the placenta and decidua is set above the placenta, perpendicular to the width. The thickness was measured along the height line from the junction of the placenta and amniotic fluid to the placental edge.
Other Tools and DefinitionsPreeclampsia and GHT were diagnosed in line with the recommendations of the International Society for the Study of Hypertension in Pregnancy.14 GDM was diagnosed in accordance with the International Association of Diabetes and Pregnancy Study Groups15 and the World Health Organization criteria. SGA was defined as a birth weight below the 10th percentile for the gestational age and sex of a standard birth weight curve used in the Turkish population.16 The APGAR score was assessed using the standard tool17 at the 1st, 5th, and 10th min after birth. Only the 1st and 5th min APGAR scores were used. The umbilical cord venous blood pH was measured using the blood gas analyzer immediately after childbirth.
Ethical ApprovalThis study was approved by the Ethics Committee of Tekirdağ Namık Kemal University (Date: 26.07.2022, Decision No: 2022.146.07.13).
Statistical AnalysisAll statistical analyses were performed using SPSS Statistics for Windows (version 25.0; IBM Corp., Armonk, NY, USA). Conformity of the continuous variables to normal distribution was evaluated using the Kolmogorov–Smirnov test. Non-parametric tests were used to analyze the non-normally distributed data. The Mann– Whitney U test was used to compare two independent groups, and the Kruskal–Wallis test was used to compare more than two groups. The relationship between the continuous variables was examined using the Spearman correlation test. The role of continuous numerical variables in predicting GDM and GHT was evaluated using the receiver operating characteristic (ROC) analysis. Statistical significance was set at p<0.05.
Reporting GuidelinesThe study was reported in accordance with the STROBE guideline.
Results
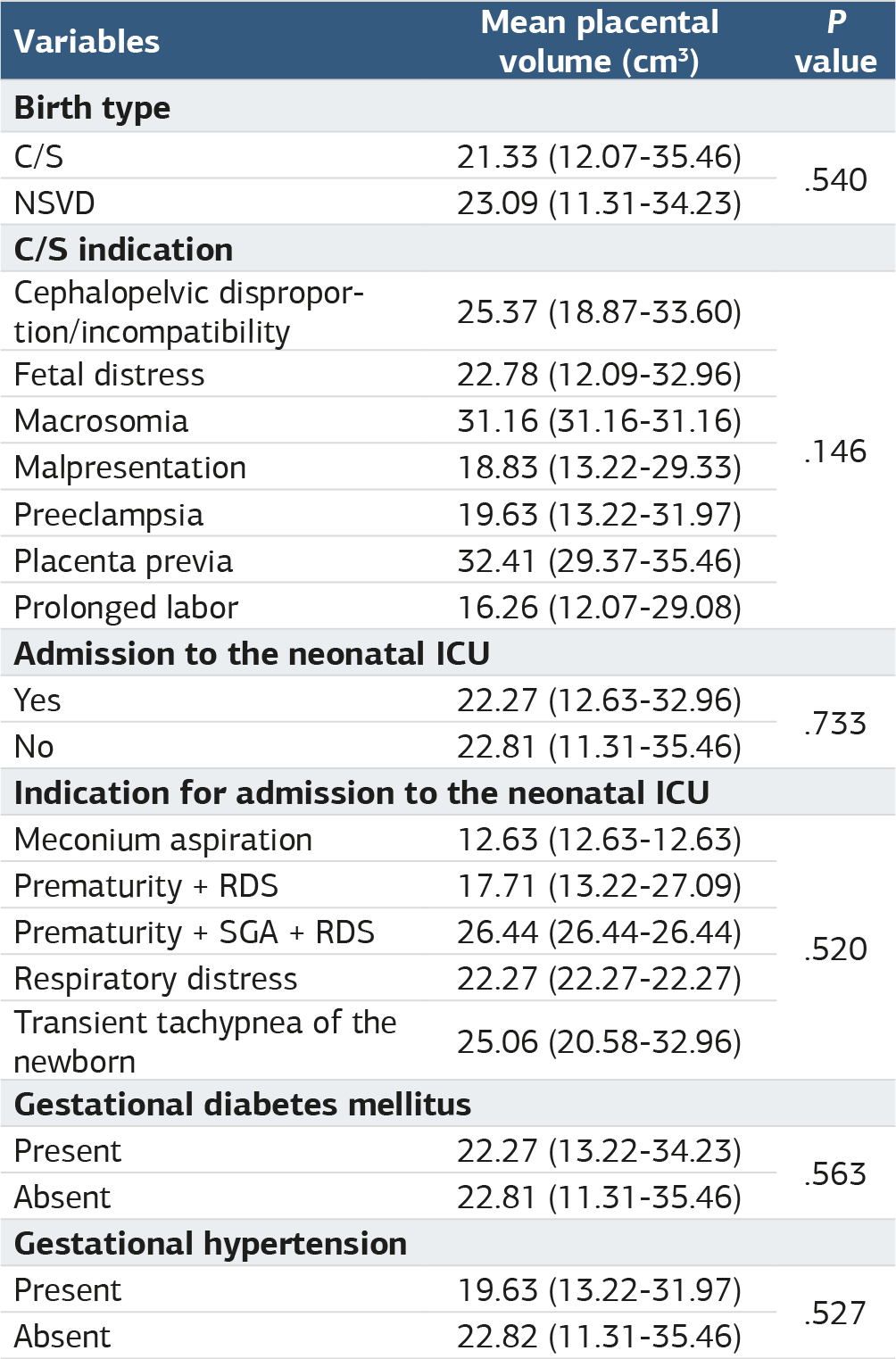
The median age of the patients was 24 (19–35) years. The median gestational age according to the last menstrual period was 26.19 (20.2–38.96) weeks while it was 12.49 ± 0.63 weeks according to USG. The median placental volume was 22.78 (11.31–35.46) cm3. GDM developed in nine (11.0%) pregnant women and GHT developed in eight (9.8%). Forty (48.8%) pregnant women delivered by C/S due to fetal distress (n = 10) or prolonged delivery (n = 10). Nine (11.0%) newborns were admitted to the ICU, and the most common indications were prematurity with respiratory distress syndrome (n = 3) and transient tachypnea (n = 3). All variables related to the pregnancies, births, and newborns and are summarized in Table 1. There was no significant relationship between the mean placental volume and the birth type (p=0.540), C/S indication (p=0.146), admission to the neonatal ICU (p=0.733), indication for ICU admission (p=0.520), GDM (p=0.563), and GHT (p=0.527). There was a significant positive correlation between the mean placental volume and the maternal weight (r = 0.251, p=0.023), gestational age according to the last menstrual period (r = 0.572, p<0.001), and gestational age according to USG (r = 0.735, p<0.001) (Table 2). ROC analysis evaluating the success of the first trimester mean placental volume in predicting the development of GDM and GHT is presented in Table 3, Figure 1 and Figure 2. The mean placental volume measured in the first trimester could not significantly predict the occurrence of GDM[AUC (95% CI) = 0.559 (0.351– 0.767), p=0.568)] and GHT[AUC (95% CI) = 0.432 (0.239– 0.626), p=0.532)].
Discussion
We found that the first trimester placental volume was significantly associated with the maternal body weight and gestational age at the time of volume measurement. There was no significant relationship between the first trimester placental volume and the other variables examined in the study. Obesity is becoming a common problem among pregnant women worldwide and is associated with a number of placentamediated obstetric complications such as preeclampsia, macrosomia, intrauterine growth restriction, and stillbirth. In addition to these direct effects, obesity can negatively and indirectly affect the placental health, pregnancy, and birth process by increasing the risk of GDM.18 The placenta has a key role in programming intrauterine development. Therefore, it is important to know the effects of maternal obesity on placental development. In the present study, a weak, significant, positive correlation was found between the first trimester placental volume and the maternal weight. We found a statistically significant positive correlation between the maternal BMI and body weight, and the fetal and placental weight. Howell and Powell showed that increased levels of maternal adipokine and metabolic hormones associated with body weight can cause an increase in the placental size and function and have long-term metabolic and behavioral consequences on the newborns.19 We found that placental volume and weight increase as the gestational age increases; this has been reported in previous studies as well.11,20 Our study results confirmed that the first trimester gestational age and placental volume were positively correlated. Pala et al. reported that placental volume was statistically significantly positively correlated with gestational age (r = 0.219) and parity (r = 0.228).11 Similarly, in another study, there was a similar and significant relationship between gestational age and placental volume.20 The placental volume increases as the pregnancy progresses because the fetus grows, which in turn increases the transfer of necessary oxygen, nutrients and other important components. Under hormonal influence, the placental volume increases in the later weeks of pregnancy. Thus, the placental volume is expected to increase as the gestational age increases. Furthermore, this volume increase is necessary for the healthy growth of the baby. However, if the increase in placental volume is more or less than it should be, it can cause problems in the growth or health of the fetus. Although the first trimester placental volume did not significantly affect the pregnancy process and outcomes in our study, ensuring the standardization of placental volume and volume increases according to the gestational age, following up women to assess this, and investigating the cause of possible adverse events can contribute to better pregnancy management and outcomes.
One of the main aims of this study was to evaluate the efficacy of first trimester placental volume in predicting the occurrence of GDB and GHT. However, there was no significant relationship between the first trimester placental volume and the development of GDB and GCT. The increased risk of greater fetal birth weight in pregnant women with GDM also carries the risk of increased placental weight.21 It is believed that this situation may be an indicator of increased delivery of nutrients to the placenta or a direct effect of GDM independently increasing both fetal and placental growth.21 Results obtained from previous studies using 2D and threedimensional (3D) USG show that there is no placental growth in the first trimester in pregnant women with GDM; placental growth occurs in the second trimester and later in pregnant women with GDM.10,11,12 Wong et al. suggested that placental overgrowth is not evident in pregnant women with GDM due to the limited-term effect of hyperglycemia in the first trimester; however, this effect emerges as pregnancy progresses when the continuous effect of hyperglycemia is seen.12 They also stated that the high glucose level in the placenta of patients with GDM may cause an increase in the glycogen, DNA, and lipid content in the placenta. While some studies have reported that the first trimester placental volumes in women with GHT are smaller than that in women without GHT,8,9,22 others have reported that they are larger,23 and some have stated that there is no significant difference.22 Our study results also showed that there was insufficient evidence to use first trimester placental volume measurements in predicting the occurrence of GHT and GDM in the later stages of pregnancy. Evaluation of the placenta via USG makes important contributions, because of its advantages such as ease of application, absence of side effects, and cost-effectiveness. In the present study, we evaluated the relationship between additional parameters, such as the newborn APGAR score, neonatal ICU requirement, gestational age, umbilical cord blood pH, and delivery type, and the first trimester placental volume, which has never been investigated before to the best of our knowledge. However, no significant relationship was found between any of these variables and the first trimester placental volume. The role of first trimester placental volume, measured via USG, in predicting pregnancy problems in the following trimesters, problems related to delivery, and problems in the early neonatal period seems to be limited or unclear.
Limitations
The current study has some limitations. Since our study was conducted at a single center with relatively few participants, the generalizability of its results is limited. Since the incidence of pregnancy complications such as GHT and GDM is relatively low, the relationship with the first trimester placental volume may not have been shown statistically. The main purpose of our study was to identify a parameter that can predict problems that may occur in the later stages of pregnancy and at birth. Therefore, placental volumes in the second and third trimesters, temporal changes in the placental volume, and the effects of these changes on the results were not investigated. Hence, there is a need for future studies that include case groups with and without relevant gestational complications and with a larger sample population, where placental volumes are evaluated not only in the first trimester, but also in the second and third trimesters.
Conclusion
In conclusion, although the first trimester placental volume was positively related to maternal weight and gestational age, it was not associated with maternal age, maternal height, maternal BMI, GDM, GHT, birth type, C/S indication, gestational age at birth baby’s birth weight, APGAR scores at 1 min and 5 min, cord blood pH, admission to the neonatal ICU, and indication for admission to the neonatal ICU. However, there is insufficient evidence regarding the role of first trimester placental volume in predicting problems related to pregnancy, delivery, and the early neonatal period. Thus, more comprehensive studies are required to investigate this.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
GDM: Gestational diabetes mellitus
GHT: Gestational hypertension
ICU: Intensive care unit
USG: Ultrasonography
References
-
Cindrova-Davies T, Sferruzzi-Perri AN. Human placental development and function. Semin Cell Dev Biol. 2022;131:66-77. doi:10.1016/j.semcdb.2022.03.039
-
Walker DW, McLean JR. Absence of adrenergic nerves in the human placenta. Nature. 1971;229:344-345. doi:10.1038/229344a0
-
Wynn RM. The Pathology of the Human Placenta. Mosby; 1968.
-
Gude NM, Roberts CT, Kalionis B, King RG. Growth and function of the normal human placenta. Thromb Res. 2004;114(5-6):397-407. doi:10.1016/j.thromres.2004.06.038
-
Burton GJ, Fowden AL, Thornburg KL. Placental origins of chronic disease. Physiol Rev. 2016;96:1509-1565. doi:10.1152/physrev.00029.2015
-
Janthanaphan M, Kor-Anantakul O, Geater A. Placental weight and its ratio to birth weight in normal pregnancy at Songkhlanagarind Hospital. J Med Assoc Thai. 2006;89:130-137.
-
Ashwal E, Ali-Gami J, Aviram A, et al. Contribution of second trimester sonographic placental morphology to uterine artery Doppler in the prediction of placenta-mediated pregnancy complications. J Clin Med. 2022;11(22):6759. doi:10.3390/jcm11226759
-
Plasencia W, González-Dávila E, González Lorenzo A, et al. First trimester placental volume and vascular indices in pregnancies complicated by preeclampsia. Prenat Diagn. 2015;35(12):1247-1254. doi:10.1002/pd.4692
-
Soongsatitanon A, Phupong V. First trimester 3D ultrasound placental volume for predicting preeclampsia and/or intrauterine growth restriction. J Obstet Gynaecol. 2019;39:474-479. doi:10.1080/01443615.2018.1529152
-
Ehlers E, Talton OO, Schust DJ, Schulz LC. Placental structural abnormalities in gestational diabetes and when they develop: a scoping review. Placenta. 2021;116:58-66. doi:10.1016/j.placenta.2021.04.005
-
Pala HG, Artunc-Ulkumen B, Koyuncu FM, Bulbul-Baytur Y. Three-dimensional ultrasonographic placental volume in gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2016;29(4):610-614. doi:10.3109/14767058.2015.1012066
-
Wong CH, Chen CP, Sun FJ, Chen CY. Comparison of placental three-dimensional power Doppler indices and volume in the first and the second trimesters of pregnancy complicated by gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2019;32(22):3784-3791. doi:10.1080/14767058.2018.1472226
-
Azpurua H, Funai EF, Coraluzzi LM, et al. Determination of placental weight using two-dimensional sonography and volumetric mathematic modeling. Am J Perinatol. 2010;27(2):151-155. doi:10.1055/s-0029-1234034
-
Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy. Hypertens Pregnancy. 2001;20(1). doi:10.3109/10641950109152635
-
Metzger BE, Gabbe SG, Persson B, et al. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676-682. doi:10.2337/dc09-1848
-
Tuzun F, Yucesoy E, Baysal B, et al. Comparison of INTERGROWTH-21 and Fenton growth standards to assess size at birth and extrauterine growth in very preterm infants. J Matern Fetal Neonatal Med. 2018;31(17):2252-2257. doi:10.1080/14767058.2017.1339270
-
Apgar V, Holaday DA, James LS, Weisbrot IM, Berrien C. Evaluation of the newborn infant: second report. J Am Med Assoc. 1958;168(15):1985-1988. doi:10.1001/jama.1958.03000150027007
-
Alwash SM, McIntyre HD, Mamun A. The association of general obesity, central obesity and visceral body fat with the risk of gestational diabetes mellitus: evidence from a systematic review and meta-analysis. Obes Res Clin Pract. 2021;15:425-430. doi:10.1016/j.orcp.2021.07.005
-
Howell KR, Powell TL. Effects of maternal obesity on placental function and fetal development. Reproduction. 2017;153:R97-R108. doi:10.1530/rep-16-0495
-
Thame M, Osmond C, Bennett F, Wilks R, Forrester T. Fetal growth is directly related to maternal anthropometry and placental volume. Eur J Clin Nutr. 2004;58(6):894-900. doi:10.1038/sj.ejcn.1601909
-
Figueroa R, Omar HA, Tejani N, Wolin MS. Gestational diabetes alters human placental vascular responses to changes in oxygen tension. Am J Obstet Gynecol. 1993;168(5):1616-1622. doi:10.1016/s0002-9378(11)90807-2
-
Odibo AO, Goetzinger KR, Huster KM, Christiansen JK, Odibo L, Tuuli MG. Placental volume and vascular flow assessed by 3D power Doppler and adverse pregnancy outcomes. Placenta. 2011;32(3):230-234. doi:10.1016/j.placenta.2011.01.010
-
González-González NL, González Dávila E, Padrón E, Armas Gonzalez M, Plasencia W. Value of placental volume and vascular flow indices as predictors of early and late preeclampsia at first trimester. Fetal Diagn Ther. 2018;44(4):256-263. doi:10.1159/000481433
Figures
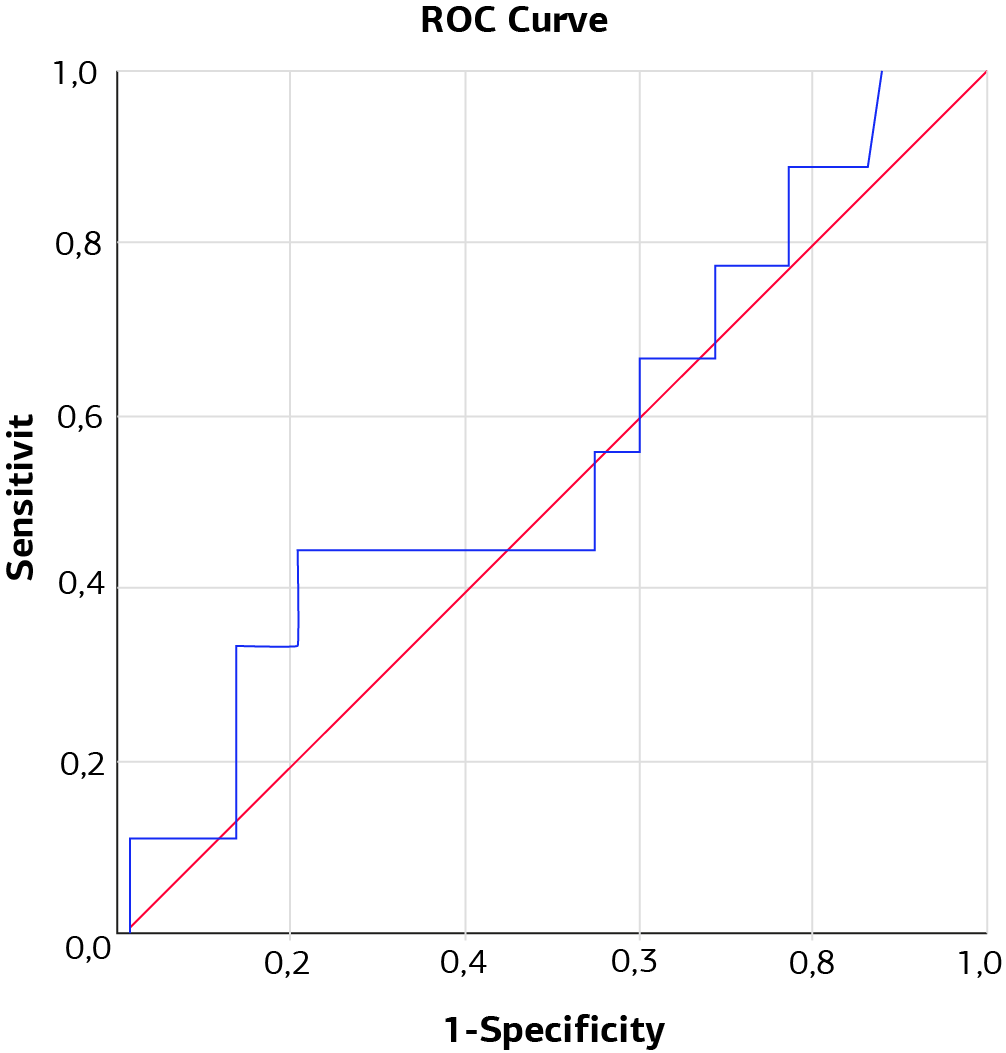
Figure 1. ROC curve graph showing the role of the mean placental volume in predicting the development of gestational diabetes mellitus

Figure 2. ROC curve graph showing the role of the placental volume in predicting the development of gestational hypertension
Tables
Table 1. Summary of the maternal, pregnancy, delivery, and newborn characteristics
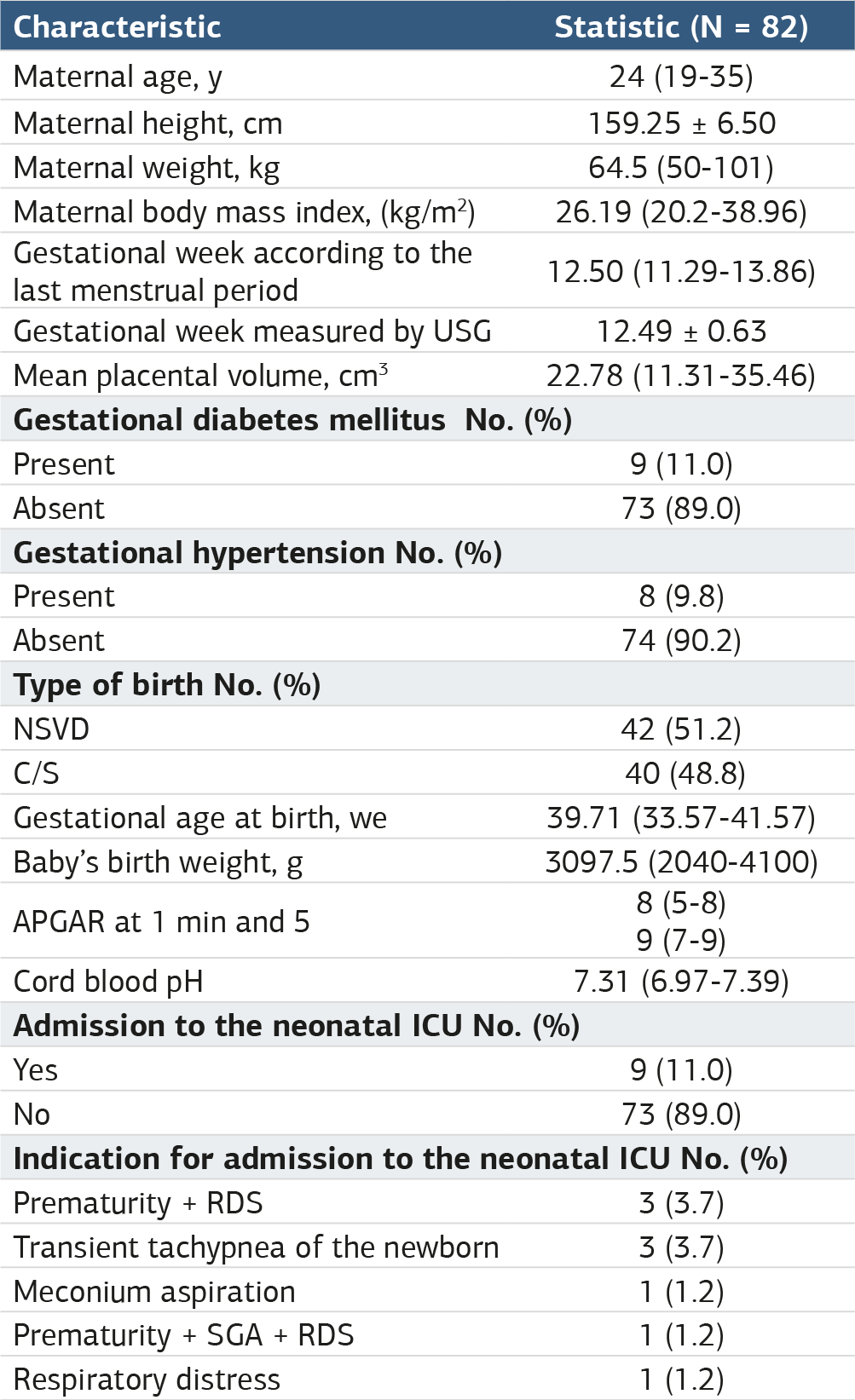
Data are presented as mean ± standard deviation or median (min–max) for continuous variables according to the normality of distribution and as frequency (percentage) for categorical variables. C/S: Cesarean section, ICU intensive care unit, NSVD: Normal spontaneous vaginal delivery, RDS: Respiratory distress syndrome, SGA: Small for gestational age, USG: Ultrasonography.
Table 2. Distribution of the mean placental volume by delivery type, indication for cesarean section, admission to the intensive care unit, and the presence of gestational diabetes mellitus and hypertension

Data are expressed as median (min–max) C/S: Cesarean section, ICU intensive care unit, NSVD: Normal spontaneous vaginal delivery, RDS: Respiratory distress syndrome, SGA: Small for gestational age, ICU intensive care unit.
Table 3. Correlation between the maternal and neonatal characteristics and the mean placental volume
r: Spearman correlation coefficient, USG: Ultrasonography.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Tevfik Giray Ozkırım, Mustafa Torehan Aslan, Ozlem Sevinc Ergul, Ilke Ozer Aslan. Can pregnancy, delivery, and early neonatal complications be predicted using the ultrasonographically measured first trimester placental volume? aprospective study. Ann Clin Anal Med 2025;16(4):237-241. doi:10.4328/ACAM.22098
- Received:
- January 6, 2024
- Accepted:
- March 19, 2024
- Published Online:
- November 24, 2024
- Printed:
- April 1, 2025