
Substance use disorders in patients with auto-immune disease comorbidwith a psychiatric disorder in Morocco
Auto-immune disease and psychiatric disorder
Authors
Abstract
AimIn dis study, we aimed to investigate the socio-demographic profile of Moroccan patients with comorbidity of Autoimmune diseases and problematic substance use, and to explore the relationship between this comorbidity, as well as to assess risk factors for problematic substance use in this category of patients.
MethodsA cross-sectional study, conducted from January 2014 to December 2022 at Ar-Razi Hospital (HAS), focuses on patients with psychiatric pathologies comorbid with autoimmune diseases. This study was approved by the Ethics Committee of Ethics Committee for Biomedical Research at the Faculty of Medicine, Rabat.
Results74 participants fulfilled the criteria, mainly women (52.7%). The majority had a higher level of education (54.1%), were single (44.6%), with an average socio-economic level (60.8%), and had a medical history (54.1%). In terms of psychiatric illnesses, schizophrenia (41.9%) and depression (36.5%) are common. Autoimmune diseases include type 1 diabetes (43.8%), psoriasis (8.1%), and UC (6.8%). Approximately half had problematic substance use, mainly poly-addiction with alcohol, tobacco and cannabis problems. Analyses show significant differences between the groups with and without problematic substance use, particularly with regard to gender, medical history, medical coverage, and type of psychiatric hospitalization (p<0.05). Logistic regression indicated that male gender increased the risk of problematic substance use by a factor of 55, while medical history increased the risk by a factor of 2 in these patients.
ConclusionSubstance use disorder is frequent in patients with autoimmune diseases for several reasons; pain, depression and anxiety which can lead to an addiction to certain molecules such as anxiolytics and analgesics.
Keywords
Introduction
Autoimmune diseases and problematic substance use are two distinct medical conditions, but there may be a relationship between them. Autoimmune diseases include a wide variety of diseases targeting many sites in the (body 1). These diseases reflect the breakdown of immune tolerance against self antigens, which attack and damage the body’s own tissues, organs and cells.1 These conditions can cause chronic inflammation and damage to affected organs or tissues.1
Problem substance use is a complex, chronic brain disorder characterized by the compulsive seeking and use of substances, despite the harmful consequences.2 It is considered a disease because it alters the structure and function of the brain, leading to a lack of control over substance use.3 The comorbidity between autoimmune diseases and problematic substance use is an emerging area of research that has attracted attention in recent years.4
Research suggests that people with autoimmune diseases run a higher risk of problematic substance use, and vice versa.4 Tobacco and alcohol are considered risk factors for some autoimmune diseases such as MS, crohn’s and type 1 diabetes and protective factors for other UC, lichen.4
This comorbidity may be due to shared genetic, biological and psycho-sociological factors, as well as the impact of chronic pain, disability and psychological distress associated with autoimmune diseases.5
In addition, certain medications used by patients with autoimmune diseases, such as analgesics to manage pain and anxiolytics to alleviate anxiety, may be potentially addictive, and may worsen the symptoms and progression of autoimmune diseases.6
Although autoimmune diseases and problematic substance use may initially seem unrelated, there is evidence to suggest that they may influence each other, with chronic inflammation4the immunomodulatory effects of addictive substances stress genetic factors and clinical implications are factors that may contribute to this comorbidity.6
Problem substance use in patients with autoimmune diseases is common. However, few publications have dealt with this subject in Morocco.
The aim of our study “Problem substance use in patients with autoimmune disease comorbid with psychiatric pathology” is to investigate the socio-demographic profile of Moroccan patients with this comorbidity and to explore the relationship between problem substance use and the course of autoimmune disease, as well as to assess the risk factors for problem substance use in this category of patients.
Materials and Methods
Type and Population of StudyThis is a cross-sectional, descriptive and analytical study.
Study DuratioJanuary 1, 2014 to December 30, 2022
Inclusion Criteria- Patients with psychiatric pathologies comorbid with autoimmune diseases hospitalized at the HAS from 2014 to 2021 recruited on the basis of a dossier. - Age over 18.
- The diagnosis is based on the DSM 5 diagnostic criteria.Exclusion Criteria - Age under 18.
- Files with missing data
Sample Size CalculationThis study will target all patients with comorbidity between autoimmune diseases and psychiatric disorders, including problematic substance use, hospitalized at the HAS from 2014 to 2022.
Data CollectionData were collected by means of a questionnaire that included sociodemographic elements, personal and family history, substance use and clinical data.
It was organized around the following axes: the patient and his socio-economic background. We were interested in the patient’s age, family, and socio-professional situation. Clinical and therapeutic features of the disease. Data management and statistical analysis were carried out using JAMOVI software for Windows2016. Qualitative variables were presented as frequencies and percentages, while quantitative variables were presented as mean standard deviation (SD) or median (interquartile range, IQR). The Chi-square test (x2) or Fisher’s exact test were performed, depending on their conditions of application, to identify differences in proportions of categorical variables between the 2 groups (G1 patients with psychiatric comorbidity and autoimmune disease with problematic substance use and G patients with psychiatric comorbidity and autoimmune disease without problematic substance use). In addition, multivariate logistic regression analyses are used to identify risk factors. All independent variables showing a statistically significant value with p< 0.05 between the two groups were included in the multivariate logistic regression.
Ethical ApprovalThis study was approved by the Ethics Committee of Biomedical Research at the Faculty of Medicine Rabat (Date: 21.12.2021, Decision No: 69/21).
Statistical AnalysisStatistical analyses were performed using Jamovi software. Pearson’s χ² test or Fisher’s exact test was used for categorical variables, and multivariable logistic regression analysis was performed. A p value <0.05 was considered statistically significant.
Reporting GuidelinesThis study was conducted and reported in accordance with the STROBE guidelines.
Results
Descriptive Statistics1. Socio-demographic characteristics
A total of 74 participants meeting the study criteria were included, 39(52.7%) were women, the median age was 41(29, 55) more than half 40(54.1%) had a higher level of education, 33(44.6%) were single, 45(60.8%) had an average socioeconomic level, 42(56.8%) had a profession and 40 (54.1%) had a medical history (Table 1).
2. Characteristics of psychiatric illness
31(41.9%) had schizophrenia, 27 (36.5%) had depression, the median duration of psychiatric illness was 10(4,19) the median number of psychiatric hospitalizations was 1(1,3) and almost all 58(79.5%) were hospitalized at the request of a third party.
3. Characteristics of autoimmune disease
32(43.8%) had type 1 diabetes, 6(8.1%) had psoriasis, 5(6.8%) had UC, median duration of autoimmune disease was 10(11, 47) median number of psychiatric hospitalizations was 1(0, 1) (Table 2).
4. Characteristics of problem substance use
38 (51.4%) had a problematic substance use, while 36(48.6%) did not. The majority had a polyaddition, with 17.6% having a problematic alcohol use, 13.5% a problematic tobacco use and 10.8% a problematic cannabis use.
Analytical StatisticsComparing the two groups (G1 patients with psychiatric comorbidity and autoimmune disease with problematic substance use and G patients with psychiatric comorbidity and autoimmune disease without problematic substance use) and using the Chi-square (x2) or Fisher’s exact test, we find that there is a statistically significant difference with a p<0.05 in sex, medical history, medical coverage and type of psychiatric hospitalization.
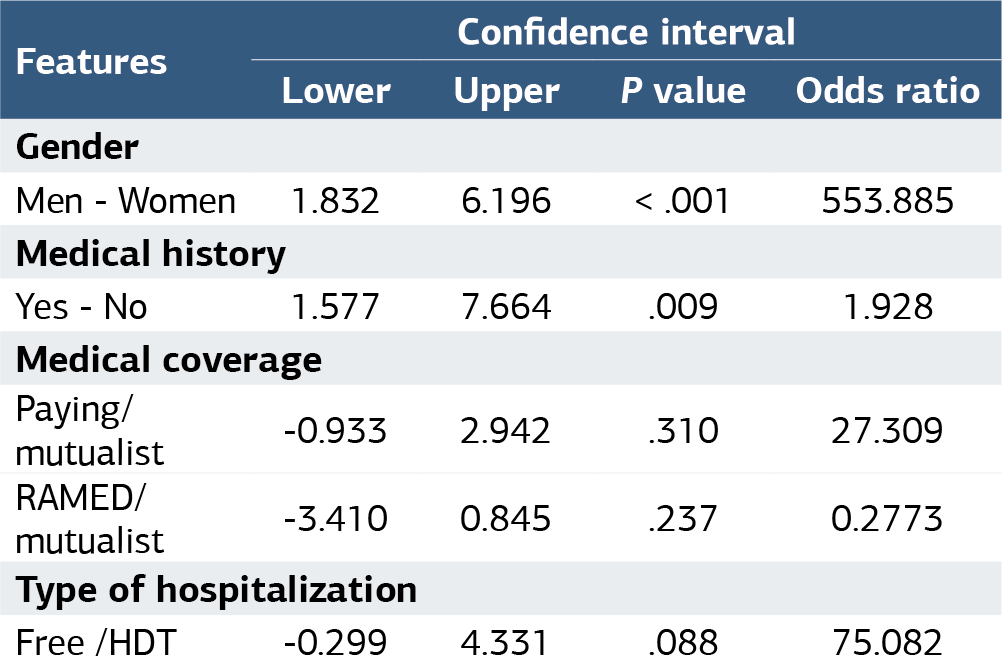
Multinomial Logistic RegressionUsing multivariate logistic regression and adjusting for confounding factors, we conclude that male gender is a risk factor that multiplies the risk of problem substance use by 55, and that having a medical history multiplies the risk by 2 in this category of patients (Table 3).
Discussion
According to our descriptive results, problematic substance use is frequent in men (37.84%), and according to our analytical results, male sex is a risk factor that increases the risk of problematic substance use by a factor of 55 in patients with autoimmune diseases, in parallel with the results of the literature showing that problematic substance use is frequent in men. Substance use was considered a predominantly male problem, and many studies of alcoholism and drug addiction were conducted with a predominance of male subjects.7 Although the incidence of autoimmune disease is higher in women than in men, this was shown in a Moroccan study of patients with autoimmune disease.8 and also in other countries.
AlcoholAccording to our results, 17.6% of patients presented a problematic use of alcohol with a higher frequency of diabetics followed by psoriasis patients, our results are close to a study done by P. Bento et al.9 They showed that more than half the insulin-dependent diabetes patients in the study sample had an approved history of substance use, with alcohol being the most commonly approved substance.9 Alcohol contains components such as ethanol and antioxidants and is considered a complex modulator of the immune system. Although it appears that high doses of alcohol directly suppress a wide range of immune responses, and that moderate doses of alcohol play a beneficial role in the immune system.10 alcohol also modulates the hypothalamic-pituitary-adrenal axis and influences the function of immune cells residing in the central nervous system (CNS), in particular astrocytes and microglia, which tightly regulate the stress response.10 The relationship between alcohol consumption and a number of chronic autoimmune inflammatory disorders has been investigated by conventional epidemiological studies, the results of which remain inconclusive.11 Alcohol consumption has a significant impact on short- and long-term health and on the day-to-day management of insulin-dependent diabetes.3 Alcohol has a hypoglycaemic effect in young people with insulin-dependent diabetes, and is responsible for diabetes self-management behaviours, including changes in appetite, reduced self-monitoring of physiological signals and inconsistent monitoring of blood glucose and insulin use and is also associated with an increased risk of diabetic ketoacidosis and higher hemoglobin A1c levels which explains the negative impact of alcohol consumption on the evolution of autoimmune disease.
TobaccoSmoking is widespread throughout the world.12,13 and it has been reported that around 1/3 of the adult population smokes tobacco.12 The problematic use of tobacco in patients with autoimmune diseases is frequent, and according to several studies.4,9 more than 46.8% approved of previous tobacco use, which parallels our findings that more than 13% of patients with autoimmune diseases are tobacco users. Smoking has been implicated in the production of numerous immune or inflammatory mediators, including pro- and anti-inflammatory cytokines.14 Recently, numerous studies have demonstrated that smoking has considerable effects on chronic inflammation and autoimmunity at the systemic level.4 including rheumatoid arthritis (RA), psoriasis, systemic lupus erythematosus (SLE). Crohn’s disease (CD) is a chronic inflammatory bowel disease with obvious morbidity and is epidemiologically correlated with smoking. However, several studies.4 show that nicotine relieves haemorrhagic colitis. Furthermore, it has been suggested that smoking induces rheumatoid arthritis by promoting Th17 responses via the aryl hydrocarbon receptor on human T cells.4
CannabisCannabis or cannabis sativa, also known as marijuana, hashish or skunk, has been consumed once in a lifetime by 3.9% of the world’s population, according to the World Drug Report.15 According to our results, 10.8% of patients present a problematic use of cannabis. These results parallel a study by Martin Storr et al.16 which showed that problematic cannabis use was found in 17.6% of IBD patients, the majority by inhalation (96.4%). These patients reported that cannabis improved abdominal pain, abdominal cramps, joint pain and diarrhea. The correlation between immune response and cannabis use has been explored, as in the longitudinal study by Kagen et al.17 which aimed to assess the role of cannabis consumption in decreasing NO production, which acts as an important mediator of antibacterial effects. Among the medical effects of cannabis consumption, anti-inflammatory properties can be explored therapeutically. Klein et al.14 explored the alteration of immune mediators referring to the suppression of (TNF-α) and other cytokines such as (GM-CSF), (IL-6), (IFN-γ) and (IL-12) were also observed after exposure to high-affinity, psychoactive ligands such as cannabinoids and THC. This explains the anti-inflammatory potential for cannabinoids, which could be useful in the treatment of inflammatory diseases such as rheumatoid arthritis, lupus erythematosus and MS.
OpioidsOpioids are typical central analgesics, producing potent analgesia effective in the treatment of severe pain. In addition to their analgesic effects, opioids have been shown to affect several organs and systems, including the immune system, through a variety of mechanisms.18 According to our results, 2.7% of patients presented with problematic opioid use, which contradicts the findings of the literature showing that problematic opioid use is frequent in this category of patients, especially given the chronic pain that accompanies autoimmune diseases.6 A study by Xiwu Lin et al.6 showed that IBD patients have a higher opioid consumption than patients without IBD; this can lead to several complications.6 Not all opioid drugs share the same immune profile; some opioids appear to have no effect on immune function, while others tend to be immuno-suppressive or immuno-stimulatory. This is probably due to a combined effect of the direct effects of opioid drugs on the immune system, indirect in vivo effects involving centrally mediated mechanisms and the systemic production and release of immunomodulatory mediators.18 There are many examples showing that individual opioids can affect the immune system in different ways. Short-term, low-dose administration of opioids appears to have a positive impact on the immune system. Comparatively, long-term, high-dose administration has a negative impact.18 Furthermore, opioids play a different role in inflammation, the cancer process and addiction due to their different effect on the immune system. On the one hand, they could prevent inflammation, inhibit tumor growth and improve addiction. On the other, they could aggravate the inflammatory response, help the tumor evade immunosurveillance, induce addiction and increase the rate of infection.18 which explains the negative impact of problematic opioid use on the evolution of autoimmune diseases.
CocaineCocaine is one of the most commonly abused drugs in Western societies, representing a major public health problem, the development and persistence of cocaine-related addictive behaviours appear to result from a complex interaction between the central nervous system (CNS), the immune system and the environment.19 According to our results, 2.7% of our patients presented with problematic cocaine use, and according to the literature, this comorbidity is present and may increase, in parallel with alcohol consumption, the risk of exocrine pathology and islet amyloid deposition in type 1 diabetic donors.19 Cocaine consumption can interfere with cytokine production and release, suggesting its immunomodulatory role.20 In addition, abuse of cocaine and other psychostimulants leads to an imbalance between pro- and anti-inflammatory responses, resulting in exacerbated neuroinflammation.20,21 A growing body of evidence suggests that cocaine is recognized by the immune system as a foreign xenobiotic component, triggering pattern recognition receptors (PRRs). This mechanism induces activation of the innate immune response and modulates the nuclear factor κB (NFκB) signaling pathway. Cocaine-induced neuroinflammation plays an important role in the pathophysiology of drug addiction. Evidence suggests that the immune response contributes to the consolidation of memory related to place preference behavior underlying cocaine administration in mice, this explains the negative impact of problem cocaine use in patients with autoimmune disease.
BenzodiazepineBenzodiazepines are drugs used to treat anxiety, epilepsy, muscle spasms, alcohol withdrawal, palliative care, insomnia and sedation. In the USA and UK, around 2% of the general population have taken benzodiazepines for 12 months or more and their use is even more widespread in elderly patients (up to 10%).22 Moreover, they are the most commonly used sedatives in critically ill patients. To produce their clinical effects, benzodiazepines allosterically modulate γ-aminobutyric acid type A (GABA A) receptors by sensitizing them to GABA.23 According to our results, 4.1% of patients present with problematic benzodiazepine use, and this can be explained by the impact of chronic illness on the quality of life of these patients, who present a high frequency of the development of anxiety disorders.24 The effect of benzodiazepines on the immune system is little known, and according to researchers, diazepam is an in vitro inhibitor of phagocytic functions and antibody synthesis, its action being mediated by specific receptors on immunocompetent cells. In contrast, alprazolam enhances the antibacterial activity exerted by normal human peripheral blood T lymphocytes in vitro. Diazepam appeared to counteract endogenous regulation of GABA A receptor activity to increase susceptibility to infection via activation of GABA A receptors containing the α1 subunit. Activation of GABA A receptors on macrophages leads to cytoplasmic acidification and impaired anti-pathogen responses. Research.25 highlight the regulation of macrophage function by GABA A receptor signaling and the potential damage of benzodiazepine exposure during pneumonia.25 This could explain the impact of problematic benzodiazepine use on the evolution of autoimmune disease.
Limitations
The relatively small sample size and single-center retrospective design may limit the generalizability of the findings.
Conclusion
Problem substance use in patients with autoimmune disease is common and can be explained by several theories, chronic pain poor quality of life, the role of immune dysfunction and the immunomodulatory effect of addictive substances, further research is needed to fully understand the nature of the relationship and to open up new possibilities for therapeutic and preventive interventions that are informed by the underlying pathogenesis of this complex comorbidity.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CNS: Central nervous system
DSM-5: Diagnostic and statistical manual of mental disorders, fifth edition
GABA: Gamma-aminobutyric acid
HAS: Ar-razi hospital
IQR: Interquartile range
MS: Multiple sclerosis
RA: Rheumatoid arthritis
SD: Standard deviation
SLE: Systemic lupus erythematosus
UC: Ulcerative colitis
References
-
Pisetsky DS. Pathogenesis of autoimmune disease. Nat Rev Nephrol. 2023;19(8):509-524. doi:10.1038/s41581-023-00720-1
-
Gasnier J, Perino J, Peyré A, Miremont-Salamé G, Daveluy A. Problematic use of psychoactive substances by young adults in Aquitaine and DROM: consequences and substances involved. Therapie. 2022;77(6):778
-
Wisk LE, Weitzman ER. Substance use patterns through early adulthood: results for youth with and without chronic conditions. Am J Prev Med. 2016;51(1):33-45. doi:10.1016/j.amepre.2016.01.029
-
Perricone C, Versini M, Ben-Ami D, et al. Smoke and autoimmunity: the fire behind the disease. Autoimmun Rev. 2016;15(4):354-374. doi:10.1016/j.autrev.2016.01.001
-
Stubbs B, Aluko Y, Myint PK, Smith TO. Prevalence of depressive symptoms and anxiety in osteoarthritis: a systematic review and meta-analysis. Age Ageing. 2016;45(2):228-235. doi:10.1093/ageing/afw001
-
Lin X, Lofland J, Zhang L, et al. Opioid use in patients with inflammatory bowel disease. Crohns Colitis 360. 2020;2(1). doi:10.1093/crocol/otaa009
-
Zakiniaeiz Y, Potenza MN. Gender-related differences in addiction: a review of human studies. Curr Opin Behav Sci. 2018;23:171-175. doi:10.1016/j.cobeha.2018.08.004
-
Missoum H, Alami M, Bachir F, et al. Prevalence of autoimmune diseases and clinical significance of autoantibody profile: data from National Institute of Hygiene in Rabat, Morocco. Hum Immunol. 2019;80(7):523-532. doi:10.1016/j.humimm.2019.02.012
-
Bento SP, Campbell MS, Soutullo O, Cogen FR, Monaghan M. Substance use among adolescents and young adults with type 1 diabetes: discussions in routine diabetes care. Clin Pediatr (Phila). 2020;59(4-5):388-395. doi:10.1177/0009922820902433
-
Barr T, Helms C, Grant K, Messaoudi I. Opposing effects of alcohol on the immune system. Prog Neuropsychopharmacol Biol Psychiatry. 2016;65:242-251. doi:10.1016/j.pnpbp.2015.09.001
-
Linneberg A, Gonzalez-Quintela A. The unsolved relationship of alcohol and asthma. Int Arch Allergy Immunol. 2016;171(3-4):155-157. doi:10.1159/000454809
-
Gilman S, Xun Z. Smoke: A Global History of Smoking. Reaktion Books; 2004:212.
-
Friedrichs B, Neumann U, Schüller J, Peck MJ. Cigarette-smoke-induced priming of neutrophils from smokers and nonsmokers for increased oxidative burst response is mediated by TNF-alpha. Toxicol In Vitro. 2014;28(7):1249-1258. doi:10.1016/j.tiv.2014.06.007
-
Klein TW, Lane B, Newton CA, Friedman H. The cannabinoid system and cytokine network. Proc Soc Exp Biol Med. 2000;225(1):1-8.
-
Merz F. United Nations Office on Drugs and Crime: World Drug Report 2017. SIRIUS Z Strateg Anal. 2018;2(1):85-86. doi:10.1515/sirius-2018-0016
-
Storr M, Devlin S, Kaplan GG, Panaccione R, Andrews CN. Cannabis use provides symptom relief in patients with inflammatory bowel disease but is associated with worse disease prognosis in patients with Crohn’s disease. Inflamm Bowel Dis. 2014;20(3):472-480. doi:10.1097/01.mib.0000440982.79036.d6
-
Tashkin DP. Effects of marijuana smoking on the lung. Ann Am Thorac Soc. 2013;10(3):239-247. doi:10.1513/annalsats.201212-127fr
-
Liang X, Liu R, Chen C, Ji F, Li T. Opioid system modulates the immune function: a review. Transl Perioper Pain Med. 2016;1(1):5-13.
-
Bruggeman BS, Campbell-Thompson M, Filipp SL, et al. Substance use affects type 1 diabetes pancreas pathology: implications for future studies. Front Endocrinol (Lausanne). 2021;12:778912. doi:10.3389/fendo.2021.778912
-
Correia C, Romieu P, Olmstead MC, Befort K. Can cocaine-induced neuroinflammation explain maladaptive cocaine-associated memories? Neurosci Biobehav Rev. 2020;111:69-83. doi:10.1016/j.neubiorev.2020.01.001
-
Pacifici R, Fiaschi AI, Micheli L, et al. Immunosuppression and oxidative stress induced by acute and chronic exposure to cocaine in rat. Int Immunopharmacol. 2003;3(4):581-592. doi:10.1016/s1567-5769(03)00050-x
-
Gleason PP, Schulz R, Smith NL, et al. Correlates and prevalence of benzodiazepine use in community-dwelling elderly. J Gen Intern Med. 1998;13(4):243-250. doi:10.1046/j.1525-1497.1998.00074.x
-
McKernan RM, Rosahl TW, Reynolds DS, et al. Sedative but not anxiolytic properties of benzodiazepines are mediated by the GABAA receptor alpha1 subtype. Nat Neurosci. 2000;3(6):587-592. doi:10.1038/75761
-
Andersson NW, Gustafsson LN, Okkels N, et al. Depression and the risk of autoimmune disease: a nationally representative, prospective longitudinal study. Psychol Med. 2015;45(16):3559-3569. doi:10.1017/s0033291715001488
-
Sanders RD, Godlee A, Fujimori T, et al. Benzodiazepine augmented gamma-aminobutyric acid signaling increases mortality from pneumonia in mice. Crit Care Med. 2013;41(7):1627-1636. doi:10.1097/ccm.0b013e31827c0c8d
Tables
Table 1. Comparison of socio-demographic characteristics between the two groups
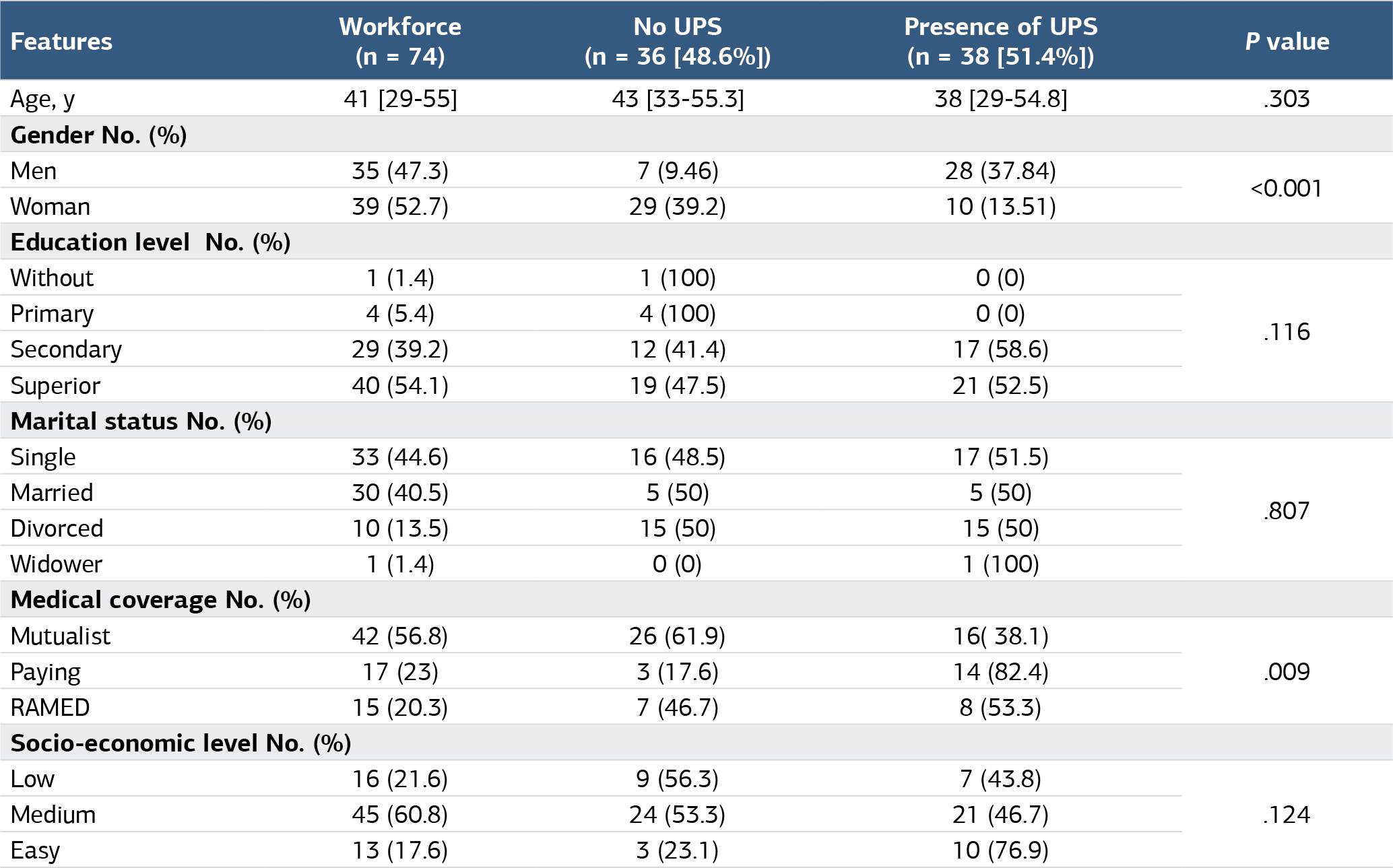
Table 2. Comparison of the characteristics of autoimmune disease and psychiatric illness between the 2 groups
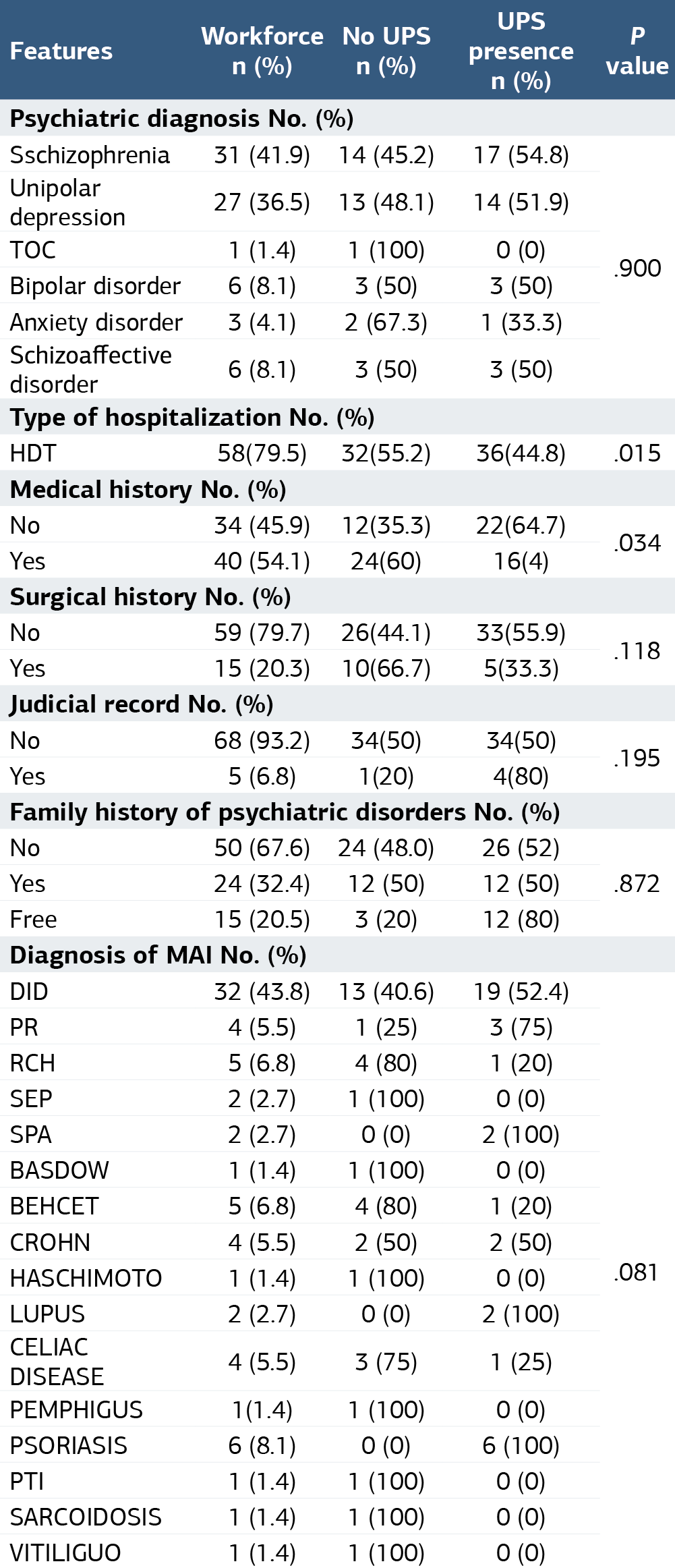
Table 3. Multivariate analysis between the two patient groups
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Soukaina Stati, Majdouline Obtel, El Hassan Ouanouche, Mohamed Amine Baba, Ahmed Kharbach, Fouad Laboudi, Maria Sabir, Fatima El Omari, Ryad Tamouza, Abderrazzak Ouanass. Substance use disorders in patients with auto-immune disease comorbidwith a psychiatric disorder in Morocco. Ann Clin Anal Med 2025;16(1):19-24. doi:10.4328/ACAM.22108
- Received:
- January 1, 2024
- Accepted:
- April 23, 2024
- Published Online:
- October 10, 2025
- Printed:
- January 1, 2025