
Contribution of the superb microvascular imaging-based vascular index inscoring thyroid nodules according to TI-RADS
Evaluation of throid nodules
Authors
Abstract
AimIn this study, we aimed to investigate the effectiveness of the superb microvascular imaging based vascular index (SMI VI) in evaluating thyroid nodules that underwent fine needle aspiration biopsy (FNAB) after scoring according to the Thyroid Imaging Reporting and Data System (TI-RADS).
MethodsThe study comprised 61 patients with thyroid nodules. Following ultrasonographic imaging of all nodules, SMI VI measurements and TI-RADS scoring were conducted. Patients with nodules scoring TI-RADS 3-5 underwent FNAB. Subsequently, all collected data were statistically analyzed.
ResultsThe study included 4 (6.5%) men and 57 (93.5%) women, with an average age of 46.85 ± 11.62 years. Regarding thyroid nodules, 18 (29.5%) were classified as TI-RADS 3, 32 (52.5%) as TI-RADS 4, and 11 (18%) as TI-RADS 5. The TI-RADS 4-5 group exhibited a mean SMI VI of 27.67, indicating a significant difference compared to TI-RADS 3. SMI VI values were similar for benign and malignant tumors (p>0.05). Additionally, a moderately positive correlation (p=0.001, r = 0.503) was found between the TI-RADS total scores of the nodules and SMI VI values.
ConclusionComparing TI-RADS categories and total scores, as well as discriminating between benign and malignant nodules, enabled us to assign SMI VI values to each nodule type. Integrating TI-RADS with SMI VI may increase nodule characterization precision, allowing for more targeted diagnostic and treatment approaches. This emphasizes the importance of using a comprehensive assessment technique for thyroid nodule evaluation.
Keywords
Introduction
Thyroid cancer is the most prevalent endocrine malignancy.1,2 With the help of ultrasound (US) examinations, the prevalence of thyroid nodules in general population is determined to be 19–68%. However, the majority of these nodules are benign, with only 7–15% are malignant.3,4 It is crucial to accurately diagnosing thyroid nodules for determining prognosis and treatment choices. US is the primary imaging tool for assessing thyroid nodules in clinical practice.5 In 2017 a guideline named “thyroid imaging, reporting and data system (TI-RADS)” was released by the American College of Radiology (ACR) and subsequently revised for the evaluation of nodules. According to this guideline, nodules are rated considering their composition, echogenicity, form, margin, and the presence of an echogenic focus. Based on the total score, it is classified as benign (TR1), minimally suspicious (TR2), mildly suspicious (TR3), strongly suspicious (TR4), and highly suspicious (TR5). If necessary, follow-up or an aspiration biopsy (FNAB) is advised.6,7 In TI-RADS, grayscale US data are utilized, but no vascular examination is conducted. Whereas the nodules with increased vascularity are associated with increased malignancy.8
Superb Microvascular Imaging (SMI) is a new Doppler technique for analyzing and calculating the blood supply of the soft tissue parts of the body. It is more sensitive in detecting low velocity microvascular blood flow and provides quantitative information blood circulation in the selected area.9
The Vascularity index (VI) is calculable using SMI, allowing for quantitative analysis. VI is determined automatically by the device by comparing the proportion of colored pixels indicating blood supply in the drawn Region of Interest (ROI) to the total number of pixels and is expressed as a numeric value between 0 and 100.10
In this study, we aimed to compare thyroid nodules according to TI-RADS categories, TI-RADS total scores, SMI VI values and fine needle aspiration biopsy results.
Materials and Methods
IndividualsA total of 65 patients, aged between 18 and 65 years, whose thyroid nodules were evaluated with the SMI method and then underwent thyroid FNAB, were included in the study Four patients with atypia or non-diagnostic pathology results of uncertain significance were excluded from the study despite undergoing FNAB twice. The study was conducted between July 2020 and August 2022.
EvaluationThe type of thyroid nodule was determined by its composition (solid, cystic, mixed, spongiform), echogenicity (anechoic, hyperechoic, isoechoic, hypoechoic, very hypoechoic), shape, contour (well-circumscribed, lobulated, poorly circumscribed, extension beyond the thyroid gland), presence and quality of echogenic focus. According to the total score attained, (macrocalcification, peripheral calcification, punctate echogenic focus) and TI-RADS value were assigned.
Two radiologists each with over ten years of ultrasound experience and two years of SMI evaluation experience conducted the evaluations. Evaluations were conducted using an Aplio 500 Platinum ultrasound device (Toshiba-Canon Medical Systems Corporation, Japan) with a high-frequency linear transducer (frequency range, 5–14 MHz). During the SMI examination, the pulse repetition frequency was set between 200 and 230 Hz, the frame rate was greater than 50 Hz, and the color gain was set between 37 and 42 decibels. In the SMI method, the thyroid nodule contours were painstakingly drawn in free drawing mode. VI was calculated in the thyroid nodule that was traced. By dividing the number of vascular signal pixels by the total number of pixels, the device automatically calculated VI (Figure 1). TI-RADS categories of thyroid nodule and VI, FNAB results, and pathology reports were compared.
Ethical ApprovalThis study was approved by the Clinical Research Ethics Committee of Ankara Education and Research Hospital (Date: 25.06.2020, Decision No: 235/2020).
Statistical AnalysisThe study was statistically analyzed using “Statistical Package for the Social Sciences” (SPSS) Version 21.0 (SPSS Inc., Chicago, Illinois, United States). Using graphical (histograms and probability graphs) and statistical (Kolmogorov-Smirnov/ Shapiro-Wilk tests), the conformity of the variables to the normal distribution was examined. Means and standard deviations were utilized for descriptive analyses, while categorical variables are presented as numbers and percentages. To compare the differences between two independent groups, the Mann-Whitney U test was utilized. Three independent groups were compared using the Kruskal-Wallis test. For pairwise comparisons, the Mann Whitney U Test and Bonferroni correction were utilized. Spearman correlation analysis was used to determine the relationships between continuous variables. In all analyses, a p-value of 0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
A total of 61 individuals were included in the study, including 4 (6.5%) men and 57 (93.5%) women. The mean age of the sample was 46.85 ± 11.62 years.
18 thyroid nodules (29.5%) were TI-RADS 3, 32 (52.5%) were TI-RADS 4, and 11 (18%) were TI-RADS 5.
FNAB determined that 38 (62.3%) of the nodules were benign, 8 (13.1%) had atypia of uncertain significance, 11 (18%) were malignant, and 4 (6.6%) were non-diagnostic. Nodules with uncertain significance and non-diagnostic atypia were subjected to a secondary FNAB. Five of the patients with atypia of uncertain significance were benign and three were malignant after a second FNAB; it was concluded that all non-diagnostic cases were benign. Thus, it was determined that 47 (77%) of the thyroid nodules were benign, while 14 (23%) were malignant. All the malignant nodules were of the papillary variety.
17 (94.4%) of the 18 patients with TI-RADS 3 were benign, while 1 (5.6%) was malignant. 24 (75%) of those diagnosed with TI-RADS 4 were determined to be benign, while 8 (25%) were malignant. Six TI-RADS 5s were benign (54.5%), while five were malignant (45.5%).
Those with TI-RADS 3 had mean SMI VI values of 11.27, those with TI-RADS 4 had mean SMI VI values of 27.26, and those with TI-RADS 5 had mean SMI VI values of 28.86 (Figure 2A). According to the TI-RADS categories, there was a significant difference among the SMI values of the three groups (p<0.05). In paired group comparisons, TI-RADS 3-4 and 3-5 differed significantly from each other (Table 1).
The group with TI-RADS 4-5 together had a mean SMI VI of 27.67, and there was a significant difference between the two groups when compared to TI-RADS 3 (Table 2) (Figure 2B). SMI VI values of benign and malignant tumours were similar (p>0.05) (Table 3). (Figure 2C).
When examining the relationship between the TI-RADS total scores of the nodules and the SMI VI values, a moderately positive correlation was discovered (p=0.001, r = 0.503).
Discussion
Thyroid nodules are commonly observed during routine examinations. US examinations with high-resolution imaging plays an essential role in differentiating benign from malignant tumors.11 In the TI-RADS classification, US findings of malignant nodules such as solid composition, low echogenicity, contour irregularity, internal echogenic foci, and vertical growth pattern are utilized.6,7
Angiogenesis is essential for formation, development, proliferation, invasion, and metastasis of the tumours such thyroid malignancies.12,13 Blood flow visualization in thyroid nodules may aid in distinguishing benign from malignant nodules. In previous studies, it was indicated that the blood supply to the periphery may be benign while the blood supply to the interior may contain malignant nodules.14,15,16 However, color Doppler imaging (CDI) and power Doppler imaging (PDI) modalities have technical limitations for detecting microvascularity and low blood flow velocity.17,18 SMI is a recently developed method for visualizing the microvascular structure by preventing motion artifacts.18 SMI allows for the calculation of VI values. VI permits quantitative analysis as opposed to morphological evaluation. It is automatically calculated by the device using the proportion of VI-colored pixels to all pixels.10 In our investigation, we compared the SMI VI values of the nodules according to their TI-RADS categories.
Machado et al. reported that the SMI method demonstrated superior microvascularity in thyroid nodules in comparison to CDI and PDI.19 Lu et al. examined 52 thyroid nodules and discovered that SMI exhibited microvessels better than CDI/PDI.17 Using both CDI and SMI, Yi Cheng Zhu et al. discovered a significant difference in the vascular distribution and morphology of benign and malignant thyroid nodules. However, in determining the vascularity distribution in thyroid nodules, no statistically significant difference was found between CDI and SMI in their study.18
A study by Zhao Yongfeng et al. comparing SMI to Contrastenhanced ultrasound (CEUS) in the evaluation of microvascularity in thyroid nodules, it was stated that the SMI method could be used to assess the microvascularity of the nodules. Compared to CEUS, the SMI procedure has the advantages of being noninvasive, having no contraindications, and being cost-effective.1
According to the TI-RADS guidelines, the risk of malignancy for TR 3, 4, and 5 nodules is, respectively, less than 5%, 5-20%, and greater than 20%.6 Middleton et al. found that the risk of malignancy for TI-RADS 3, 4, and 5 nodules was 4.8%, 9.1%, and 35.0%, respectively.20 In our study, the malignancy risks of TI-RADS 3, 4, and 5 nodules were greater than in Middleton et al.’s study.
Malignant nodules had higher SMI VI values than benign nodules, but the difference was not statistically significant in our study. In a meta-analysis conducted by Hui Jin et al., the SMI values of malignant nodules were found to be higher than those of benign nodules.11 In several studies, grading has been performed when determining SMI values, which is insufficient for providing genuine qualitative values. Min Ji Hong et al. concluded that the SMI quantification values of malignant nodules were substantially greater than those of benign nodules.21
In their study, Lin Chen et al. demonstrated that the combination of TI-RADS and SMI improved the diagnostic performance of TI-RADS.5 According to Changfu Zhu et al.’s meta-analysis, the diagnostic efficacy of TI-RADS plus SMI in differentiating benign and malignant thyroid nodules is superior to that of TI-RADS alone.22 In our study, a moderate correlation was discovered between TI-RADS total scores and SMI VI values. Comparing the VI values of the groups, it is determined that the TI-RADS 4-5 groups was significantly higher than TI-RADS 3. It was observed that the microvascularity of thyroid nodules increased as the likelihood of risk of malignity increased.
Due to the limited number of patients with malignant pathology results, we may not have observed a significant difference in our study. Despite its limitations, in our investigation, unlike other studies, VI values were analysed, and it was believed that SMI VI evaluations could aid in TI-RADS classification. Future research will require large, multicenter investigations with quantitative results.
Limitations
Here are some potential limitations that could be associated with this study. The TI-RADS system itself may have its own limitations. It might not capture all the nuances related to thyroid nodule malignancy risk, and there might be gray areas that aren’t definitive. Any diagnostic method has a risk of producing false positives (indicating a problem when there isn’t one) or false negatives (indicating no problem when there is one). The gold standard for confirming malignancy is typically a biopsy. If not all nodules undergo biopsy, it might lead to potential errors in classification.
Conclusion
By comparing thyroid nodules using TI-RADS categories and total scores, coupled with a benign-malignant distinction, we were able to determine the SMI VI values associated with each nodule type. The integration of TI-RADS with SMI VI values can potentially enhance the precision of nodule characterization, paving the way for more targeted diagnostic and therapeutic approaches. This underscores the importance of utilizing a multi-faceted assessment strategy in the evaluation of thyroid nodules.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ACR: American college of radiology
CDI: Color doppler imaging
CEUS: Contrast-enhanced ultrasound
FNAB: Fine needle aspiration biopsy
PDI: Power doppler imaging
ROI: Region of interest
SMI: Superb microvascular imaging
SPSS: Statistical package for the social sciences
TI-RADS: Thyroid imaging reporting and data system
US: Ultrasound
VI: Vascular index
References
-
Yongfeng Z, Ping Z, Hong P, et al. Superb microvascular imaging compared with contrast-enhanced ultrasound to assess microvessels in thyroid nodules. J Med Ultrason. 2020;47(2):287-297. doi:10.1007/s10396-020-01011-z
-
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1-133. doi:10.1089/thy.2015.0020
-
Smith-Bindman R, Lebda P, Feldstein VA, et al. Risk of thyroid cancer based on thyroid ultrasound imaging characteristics: results of a population-based study. JAMA Intern Med. 2013;173(19):1788-1795. doi:10.1001/jamainternmed.2013.9245
-
Trimboli P, Guglielmi R, Monti S, et al. Ultrasound sensitivity for thyroid malignancy is increased by real-time elastography: a prospective multicenter study. J Clin Endocrinol Metab. 2012;97(12):4524-4530. doi:10.1210/jc.2012-2951
-
Chen L, Zhan J, Diao XH, et al. Additional value of superb microvascular imaging for thyroid nodule classification with the thyroid imaging reporting and data system. Ultrasound Med Biol. 2019;45(8):2040-2048. doi:10.1016/j.ultrasmedbio.2019.05.001
-
Tessler FN, Middleton WD, Grant EG, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am Coll Radiol. 2017;14(5):587-595. doi:10.1016/j.jacr.2017.01.046
-
Hoang JK, Middleton WD, Tessler FN. Update on ACR TI-RADS: successes, challenges, and future directions, from the AJR special series on radiology reporting and data systems. AJR Am J Roentgenol. 2021;216(3):570-578. doi:10.2214/ajr.20.24608
-
Chung J, Lee YJ, Choi YJ, et al. Clinical applications of Doppler ultrasonography for thyroid disease: consensus statement by the Korean Society of Thyroid Radiology. Ultrasonography. 2020;39(4):315-330. doi:10.14366/usg.20072
-
Mao Y, Mu J, Zhao J, et al. The value of superb microvascular imaging in differentiating benign renal mass from malignant renal tumor: a retrospective study. Br J Radiol. 2018;91(1082):20170601.
-
Durmaz MS, Akyürek N, Kara T, et al. Quantitative assessment of thyroid gland vascularization with vascularization index using color superb microvascular imaging in pediatric patients with Hashimoto thyroiditis. Ultrasound Q. 2019;35(3):281-289. doi:10.1097/ruq.0000000000000430
-
Jin H, Wang C, Jin X. Superb microvascular imaging for distinguishing thyroid nodules: a meta-analysis (PRISMA). Medicine (Baltimore). 2022;101(24):e29505. doi:10.1097/md.0000000000029505
-
Gilcy GK, Kuttan G. Evaluation of antiangiogenic efficacy of Emilia sonchifolia (L.) DC on tumor-specific neovessel formation by regulating MMPs, VEGF, and proinflammatory cytokines. Integr Cancer Ther. 2016;15(4):NP1-NP12. doi:10.1177/1534735416630807
-
Mancini M, Greco A, Salvatore G, et al. Imaging of thyroid tumor angiogenesis with microbubbles targeted to vascular endothelial growth factor receptor type 2 in mice. BMC Med Imaging. 2013;13:31. doi:10.1186/1471-2342-13-31
-
Kim DW, In HS, Choo HJ, et al. Solid and isoechoic thyroid nodules without malignant sonographic features: comparison of malignancy rate according to nodule size, shape and color Doppler pattern. Ultrasound Med Biol. 2013;39(2):269-274. doi:10.1016/j.ultrasmedbio.2012.09.018
-
Kim DW, Jung SJ, Eom JW, et al. Color Doppler features of solid, round, isoechoic thyroid nodules without malignant sonographic features: a prospective cytopathological study. Thyroid. 2013;23(4):472-476. doi:10.1089/thy.2012.0238
-
Papini E, Guglielmi R, Bianchini A, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002;87(5):1941-1946. doi:10.1210/jcem.87.5.8504
-
Lu R, Meng Y, Zhang Y, et al. Superb microvascular imaging (SMI) compared with conventional ultrasound for evaluating thyroid nodules. BMC Med Imaging. 2017;17(1):65. doi:10.1186/s12880-017-0241-5
-
Zhu YC, Zhang Y, Deng SH, Jiang Q. A prospective study to compare superb microvascular imaging with grayscale ultrasound and color Doppler flow imaging of vascular distribution and morphology in thyroid nodules. Med Sci Monit. 2018;24:9223-9231. doi:10.12659/msm.911695
-
Machado P, Segal S, Lyshchik A, Forsberg F. A novel microvascular flow technique: initial results in thyroids. Ultrasound Q. 2016;32(1):67-74. doi:10.1097/ruq.0000000000000156
-
Middleton WD, Teefey SA, Reading CC, et al. Multiinstitutional analysis of thyroid nodule risk stratification using the American College of Radiology Thyroid Imaging Reporting and Data System. AJR Am J Roentgenol. 2017;208(6):1331-1341. doi:10.2214/ajr.16.17613
-
Hong MJ, Ahn HS, Ha SM, et al. Quantitative analysis of vascularity for thyroid nodules on ultrasound using superb microvascular imaging: can nodular vascularity differentiate between malignant and benign thyroid nodules? Medicine (Baltimore). 2022;101(5):e28725. doi:10.1097/md.0000000000028725
-
Zhu C, Zhong L, Lin M, et al. The value of TI-RADS combined with superb microvascular imaging in distinguishing benign and malignant thyroid nodules: a meta-analysis. PLoS One. 2022;17(1):e0261521. doi:10.1371/journal.pone.0261521
Figures

Figure 1. Hypoechoic nodule with lobulated contour in the right lobe of the thyroid gland (A) and SMI VI value (B)

Figure 2. SMI VI values according to TI-RADS category (A); SMI VI values of TI-RADS 3 AND TI-RADS 4-5 groups (B); SMI VI values of benign and malignant groups (C)
Tables
Table 1. SMI VI values of TI-RADS 3, TI-RADS 4 and TI-RADS 5 nodules
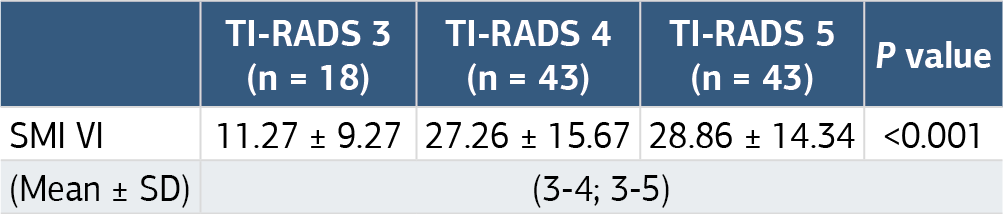
TI-RADS: Thyroid imaging, reporting and data system; SMI VI: Superb microvascular imaging vascularity index; SD: standard deviation
Table 2. SMI VI values of TI-RADS 3 and TI-RADS 4-5 nodules

TI-RADS: Thyroid imaging, reporting and data system; SMI VI: Superb microvascular imaging vascularity index; SD; standard deviation
Table 3. SMI VI values of benign and malignant tumours

SMI VI: Superb microvascular imaging vascularity index; SD: standard deviation
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Habip Eser Akkaya, Çağrı Damar, Eylem Pınar Eser, Ömer Kazcı. Contribution of the superb microvascular imaging-based vascular index inscoring thyroid nodules according to TI-RADS. Ann Clin Anal Med 2025;16(1):68-71. doi:10.4328/ACAM.22138
- Received:
- February 8, 2024
- Accepted:
- October 3, 2024
- Published Online:
- November 2, 2024
- Printed:
- January 1, 2025