
Nervus ischiadicus variations and clinical importance: a cadaver and MRI study
Nervus ischiadicus variations
Authors
Abstract
AimIn this study, the variations, bifurcation levels, morphometric and topographic features of the ischiadicus nerve (NI), which has an important role in its protection, were investigated.
MethodsIn eighteen cadaver limb dissections, variations related to NI and musculus piriformis (MP) and NI bifurcation levels, morphometric and topographic features of NI were investigated. At the foramen infrapiriforme (FI) exit, the distance between NI and trochanter major (TM), spina iliaca anterior superior (SIAS), crista iliaca (CI), spina iliaca posterior superior (SIPS), hiatus sacralis (HS) and tuber ischiadicum (TI) was measured. NI variations were investigated in 115 hip MRIs of 59 patients in the radiology archives.
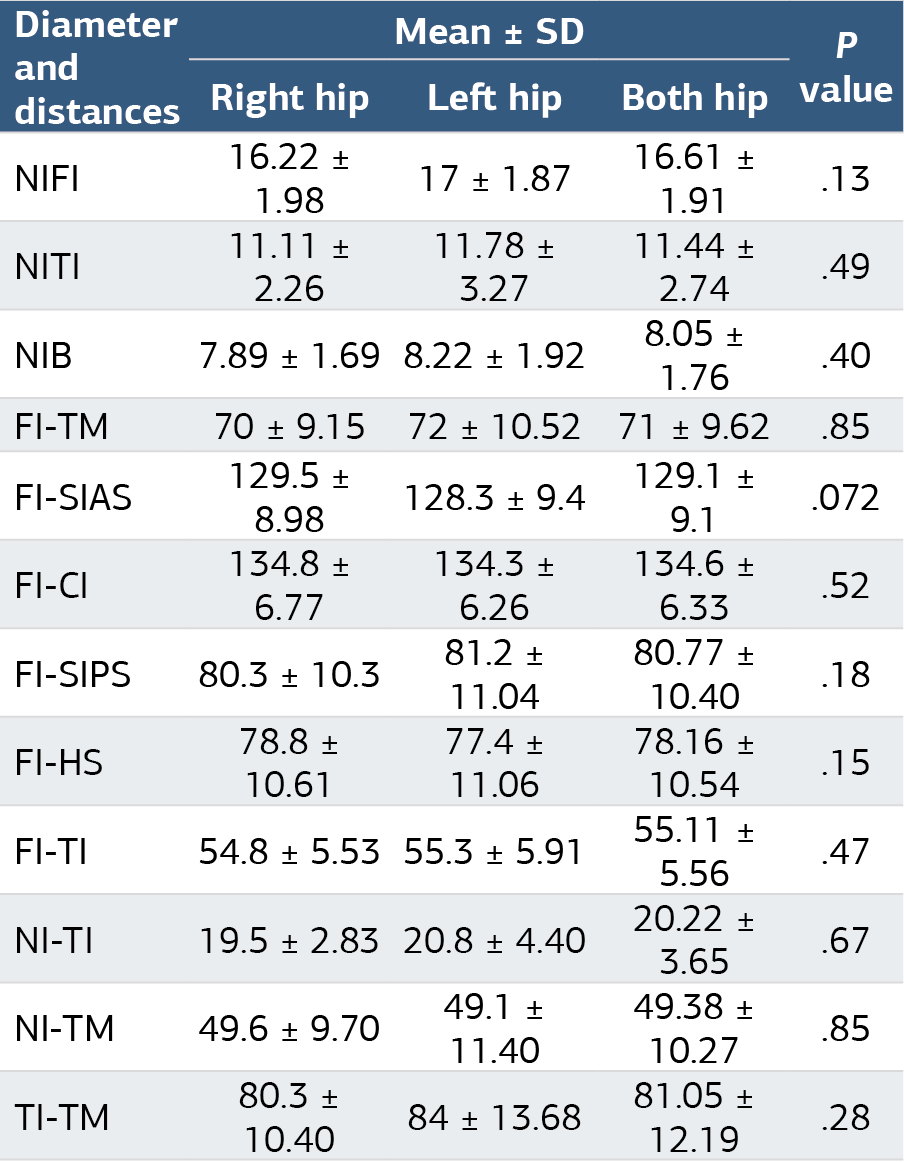
ResultsNo variation was encountered in NIs other than Type A, which is the most common and considered normal. In all lower extremities, it was observed that the NI bifurcated in the distal 1/3 of the thigh (Group E). FI-TM: 71 ± 9.62 mm, FI-SIAS: 129.56 ± 8.98 mm, FI-CI: 134.6 ± 6.33 mm, FI-SIPS: 80.77 ± 10.40 mm, FI-HS: 78.16 ± 10.54 mm and FI-TI: 55.11 ± 5.56 mm was found. 115 Magnetic resonance radiographs (MRI) showed Type B variation in 5 hips (4.34%) and Type A variation in the others (95.65%).
ConclusionWe think that our cadaver and MRI study can serve as a guide during clinical practice and will be useful in reducing NI injuries.
Keywords
Introduction
Nervus ischiadicus (NI) is the longest and thickest nerve in the human body. As the terminal branch of the plexus lumbosacralis, it passes through the foramen infrapiriforme (FI) in front of the musculus piriformis (MP), leaving the pelvis and reaching the subgluteal space. NI reaches the back compartment of the thigh by passing between the musculus gluteus maximus (GM), short external rotators of the hip, trochanter major (TM), tuber ischiadicum (TI). NI divides into the nerve tibialis (NT) and nerve fibularis communis (NFC) end branches at the upper corner of the fossa poplitea.1,2,3
Throughout its course, various anatomical variations with different clinical implications have been described regarding NI and its branches. For example, variations in the exit of the NI to the gluteal region have been associated with piriformis syndrome (PS), and it has been suggested that the nerve can be easily injured during hip injections and hip surgery.4,5,6,7 It has been suggested that a high bifurcation level may predispose to entrapment neuropathy, sciatica, restless legs syndrome and inadequate or failed nerve block.3 For this reason, it is emphasized that an adequate knowledge of the anatomical variations, morphometric and topographic features of NI and its branches is important in order to prevent nerve injuries.8 In Beaton and Anson’s study, the relationship of NI and its subdivisions with the piriformis muscle was evaluated and its variations were classified.9
Thanks to high-resolution Magnetic Resonance Imaging (MRI), it is possible to obtain detailed information about NI variations, course, morphology and topography, and non-invasive, real-time, dynamic and functional images can be obtained in living tissues.10
In the cadaveric study, variations of the NI according to the Beaton and Anson classification, bifurcation levels, and some morphometric and topographic features were tried to be determined using certain reference points. In addition, the images of patients who presented to the clinic with various prediagnoses and underwent magnetic resonance imaging (MRI) of the hip were retrospectively evaluated and NI variations were investigated.
Materials and Methods
Cadaver StudyEighteen lower extremities of 9 cadavers, 2 females and 7 males, who had no previous hip and thigh surgery, anomaly or other pathology, fixed with formaldehyde in the laboratory of the Department of Anatomy, Inönü University Faculty of Medicine, were included in the study. During the dissection process, the insertion of the GM was preserved; The ilium, sacrum and ligamentum were carefully stripped from their origin at the sacrotuberale and lifted laterally. Then, the deep subgluteal region was reached and the musculus gluteus medius (Gm), musculus gluteus minimus, MP, NI, nervus cutaneus femoris posterior and hip short external rotators were explored. The back of the thigh was reached by following the musculus quadratus femoris distally, between NI, tuber ischiadicum (TI) and TM. Dissection was continued distally to determine the bifurcation level of NI. By following the NT and NFC, the dissection was terminated in the proximal posterior part of the leg. Thus, NI in the extremities was dissected from the gluteal region to the fossa poplitea.3,8
It was investigated whether there was a variation related to NI and MP according to the modified Beaton and Anson classification.9 (Table 1A). Then, the bifurcation levels of NI in the gluteal region, back of the thigh and popliteal region, were investigated.3 (Table 1B).
FI, TM, SIAS (spina iliaca anterior superior), Crista iliaca (CI), spina iliaca posterior superior (SIPS), hiatus sacralis (HS) and TI reference points were marked in the gluteal region of the right and left lower extremities.
First, the transverse diameters of NI were measured at FI, between TI-TM and at the bifurcation level and their morphometric properties were determined (Figure 1 A, B, Figure 2). In addition, at the TI-TM distance level, the distances of NI to TI and TM were measured in millimeters. To determine the topographic features, at the FI exit, the distances between the NI midpoint and SIAS, CI, SIPS, HS, TI and TM were measured in millimeters (Figure 2).
Statistical AnalysisThe data of our study were uploaded to the IBM SPSS 26.0 (Statistical Package for the Social Sciences) program and transferred to the computer environment, and statistical analysis was performed. Summary of right and left hip data are expressed as mean ± SD (standard deviation). Minimum, maximum and mean ± SD values were summarized.
The mean and standard deviation (SD) of right and left side measurements were calculated and it was investigated whether there was a statistically significant difference between the two side measurements. Then, the mean and SD deviations of all morphometric and topographic measurements were determined.
MRI Study115 hip MRIs of 59 patients, taken between 2018 and 2020 with preliminary diagnoses such as hip pain, tendinitis, bursitis, labrum tear, degenerative arthritis and avascular necrosis, in the archives of İnönü University Faculty of Medicine, Department of Radiology, were evaluated retrospectively.
Patients aged 18 and over were included in the study. Shots with artifacts due to movement or metallic implants, and images of children and pregnant patients were excluded from the study. Unilateral hip MRI was requested in 50 patients, and bilateral hip MRI was requested in 9 patients. Evaluated MRI of 45 hips of 23 male patients with an average age of 46.8 years (27-75 years), excluding one right side where a healthy image could not be obtained. 70 hip MRIs of 36 female patients with an average age of 50.7 (26-79 years) were evaluated, except for the two right sides where healthy images could not be obtained. NI variations were investigated in 115 hip MRIs. Evaluations were performed blindly with clinical and diagnostic information by a Radiologist with 5 years of general radiology experience. Images of each hip joint were examined in all sequences on the PACS (Picture Archiving and Communication Systems) workstation, and the findings were categorized according to six anatomical variant types in accordance with the modified Beaton and Anson variation classification. The incidence rates of the detected variants according to gender, side and overall were calculated.
All MRI scans were performed on a 3 Tesla MRI device (3T MR device Skyra, Siemens, Erlangen, Germany), with the patient in the supine position, using an 18-channel body coil in the anterior and a 32-channel body coil (Torso Coil) in the posterior.
Ethical ApprovalThis study was approved by Ethics Committee of İnonu University Malatya Clinical Research (Date: 01.06.2020, Decision No:2020/50).
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
Cadaver StudyNI variations: In this study, no variation was encountered other than Type A, which is the most common and considered normal according to the Beaton and Anson classification.
Bifurcation level: In all lower extremities, NI was observed to branch into branches in the distal 1/3 of the thigh (Group E).
Morphometric feature: Transverse diameters of NI at the FI exit (NIFI), between TI and TM (NITI) and at the bifurcation (NIB) level, right and left sides were measured in millimeters (mm) and the data were compared (Table 2).
Topographic feature: At the FI exit, the distances between NI and TM, SIAS, CI, SIPS, HS, TI, the distance between TI and TM, and between TI and TM, the distances of NI to TI and TM were measured and compared on the right and left sides. When the data of the two sides were compared, no statistically significant difference was found (p>0.05). Additionally, the mean and SD of data from both sides were obtained (Table 3). By determining the mean and SD of the data obtained from all measurements on the right and left sides, the morphometric and topographic features of NI in the lower extremities used in our study were determined (Table 2).
MRI StudyType A (95.65%) variation, which is considered normal, was determined in 110 hip MRIs of 115 hips. 45 hip MRIs of 23 male patients were evaluated. According to the Beaton and Anson classification, Type B variation, in which the NT passes in front of the muscle and the NFC passes through the muscle, was detected in a total of 3 hips, one patient on the right side and one patient bilaterally. 70 hip MRIs of 36 female patients were evaluated. Type B variation according to Beaton and Anson classification was detected in one patient’s bilateral hips. Among 115 hip MRIs, Type B variation was detected in 5 (4.34%) hips. No other types of variations were encountered (Figure 3).
Discussion
Due to variations of NI, iatrogenic nerve injuries may occur during clinical applications such as gluteal region injections, nerve blocks, USG-guided pelvic abscess drainage, hip replacement surgeries and hip arthroscopies. The probability of encountering a NI variation before a surgical or interventional application to the gluteal region is 17%, and the type of variation is 80% Type B.11,12
The most common cause of NI injuries in developing countries is incorrect injections. Since the nerve will be close to the safe area in the presence of variation, there is a risk of injury even if the injection is made in the appropriate area.13
During hip arthroscopy and hip replacement surgeries, the risk of iatrogenic nerve injury may be increased in patients with NI variation. Additionally, if there is nerve variation during the hip surgery due to the pressure of the retractors and maneuvers such as flexion, adduction, internal-external rotation, and traction, the nerve with decreased mobility may be stretched and injured.14 In a study involving 1000 total hip replacement surgeries, possible causes were listed in patients with postoperative NI palsy, and it was reported that anatomical variations came first.15
NI variation was detected in 21 (16.2%) of 130 patients who underwent surgery with a preliminary diagnosis of Piriformis syndrome (PS). Despite the studies suggesting that there is no significant difference between the variation rate in those diagnosed with PS and the variation rates in the normal population, there are also studies reporting that the most common cause of PS is NI variations.16 In the study of Pecina and Hernando, it was reported that especially Type B variations were more closely related to PS.17,18
Based on their study on 34 fetal cadavers, Özbağ et al. suggested that knowing the NI variations, their location and course relative to reference points, before all clinical applications for the gluteal region and back of the thigh could reduce iatrogenic nerve injuries.8 In our study, adult cadavers were used and NI morphometry was evaluated with diameter measurements at different levels, NI topography and bifurcation levels were evaluated by measuring the distances between NI and certain reference points at the FI exit.
NI bifurcation can occur at any level from the plexus sacralis to the distal fossa poplitea. It may arise from the NI plexus sacralis as two separate branches. The most common bifurcation level is the upper corner of the fossa poplitea. The incidence of NI bifurcation within the pelvis has been reported to be 16-24%. At upper levels, the bifurcation may lead to failure in popliteal block anesthesia. Variations related to the level of bifurcation may predispose to PS, sciatalgia and other entrapment neuropathies. It is recommended that bifurcation levels and variations be taken into account when planning any medical application around NI and its branches.19,20,21
Marco et al., in their study of 59 cadavers, encountered 21.64% Type B and 6.49% Type C variation, and reported variation in 38.89% of male cadavers and 14.29% of female cadavers. They reported that they measured the NI transverse diameter at the FI level as an average of 21.1 mm, while in other studies the average was 17 ± 0.37 mm.22 In our study, the average NI diameter at the FI level was determined to be 16.61 mm, and the NI bifurcation level was in the upper corner of the fossa poplitea in all cadavers.
Variation rates detected during cadaver studies and surgical interventions vary between 1.5% and 35.8%.3 Pokorny et al. encountered bilateral Type B variation in only one of 91 cadavers.5
In our cadaver study, no variations were encountered according to the Beaton and Anson classification and NI bifurcation levels. Factors such as difficulties in supplying cadavers, supplying cadavers from different countries and different races, models in medical education, the prominence of visual and virtual reality materials, negative effects of cadavers on student psychology, harmful odors caused by fixation, deformation, decomposition, and the cost of storage have a negative effect on the number of cadavers. We think that we did not encounter any variation due to this reason.
It is difficult to explain the pathophysiology of PS and iatrogenic nerve injury mechanisms through studies on solidified, deformed and decomposed cadavers with unknown history. MRI, which offers the opportunity to study living and moving bodies, is a gold standard method for detecting NI variations.23 The course, size, fascicular pattern of the nerve, and lesions that cause irritation along the nerve can be easily determined. Khan et al. retrospectively evaluated 93 hip and pelvis MRIs of 88 patients diagnosed with sciatalgia. They detected Type A variation in 52 (55.9%) patients, Type B variation in 39 (41.9%) patients, and Type C variation in 2 patients. They encountered much higher variation than expected and suggested that there was a strong connection between NI variations and sciatalgia.24
Variation rates reported in MRI studies vary between 9-13%. In our study, 95.6% Type A and 4.3% Type B variation were detected according to the Beaton and Anson classification.
In clinical studies, 50% of the causes of NI injuries after hip replacement surgeries could not be explained.25 Based on this result, it can be thought that at least some of the 50% of unexplained nerve injuries after hip replacement may be due to NI variations. Therefore, by performing a preoperative MRI in patients planned for hip surgery, the course and variations of NI can be detected and nerve injuries due to variations can be prevented.
Limitations
The small number of hip MRIs we had and the fact that the MRIs were not specifically aimed at imaging NI variations may have led to some variations being overlooked. For this reason, the variation rates we detected in MRI may be less than in previous studies. Despite this, we observed that variations can be demonstrated in routine hip MRIs.
Conclusion
During interventional procedures such as gluteal region injections and nerve blocks, good knowledge of NI variations, bifurcation levels, morphometric and topographic features can protect the nerve or minimize iatrogenic nerve injuries. The risk of iatrogenic nerve injury may be increased in patients with NI variation during hip replacement surgery and hip arthroscopy. These variations can be detected in advance with imaging techniques and surgical planning can be made accordingly. Additionally, unnecessary spinal surgeries can be prevented by differentiating spinal and extraspinal sciatalgia with imaging techniques.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Written informed consent was waived due to the retrospective design of the MRI component of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
FI: Foramen infrapiriforme
GM: Gluteus maximus
MP: Musculus piriformis
MRI: Magnetic resonance imaging
NFC: Nervus fibularis communis
NI: Nervus ischiadicus
NT: Nervus tibialis
PACS: Picture archiving and communication systems
PS: Piriformis syndrome
SD: Standard deviation
References
-
Carro LP, Hernando MF, Cerezal L, Navarro IS, Fernandez AA, Castillo AO. Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement and sciatic nerve release. Muscles Ligaments Tendons J. 2016;6(3):384-396.
-
Barbosa ABM, Santos PVD, Targino VA, et al. Sciatic nerve and its variations: is it possible to associate them with piriformis syndrome? Arq Neuropsiquiatr. 2019;77(9):646-653. doi:10.1590/0004-282x20190093
-
Javia MD, Vikani SK. Cadaveric study on variations in the level of bifurcation of sciatic nerve and its clinical implications. Int J Anat Radiol Surg. 2019;8(2):29-32.
-
İkiz ZAA, Bilge O, Üçerler H, Çelik S, Boduç E. Variant anatomy of sciatic nerve and their clinical implications. Ege Tip Derg. 2018;57(2):88-93
-
Pokorny D, Jahoda D, Veigl D, Pinskerova V, Sosna A. Topographic variations of the relationship of the sciatic nerve and the piriformis muscle and its relevance to palsy after total hip arthroplasty. Surg Radiol Anat. 2006;28(1):88-91.
-
Natsis K, Totlis T, Konstantinidis GA, Paraskevas G, Piagkou M, Koebke J. Anatomical variations between the sciatic nerve and the piriformis muscle: a contribution to surgical anatomy in piriformis syndrome. Surg Radiol Anat. 2014;36(3):273-280. doi:10.1007/s00276-013-1180-7
-
Benzon HT, Katz JA, Benzon HA, Iqbal MS. Piriformis syndrome: anatomic considerations, a new injection technique, and a review of the literature. Anesthesiology. 2003;98(6):1442-1448. doi:10.1097/00000542-200306000-00022
-
Davut O, Yakup G, Sevgi B, et al. The topographical features and variations of nervus ischiadicus in human fetuses. Bratisl Lek Listy. 2011;112(8):475-478.
-
Atoni AD, Oyinbo CA, Francis DAU, Tabowei UL. Anatomic variation of the sciatic nerve: a study on the prevalence, and bifurcation loci in relation to the piriformis and popliteal fossa. Acta Med Acad. 2022;51(1):52-58. doi:10.5644/ama2006-124.370
-
Petchprapa CN, Rosenberg ZS, Sconfienza LM, Cavalcanti CFA, La Rocca Vieira R, Zember JS. MR imaging of entrapment neuropathies of the lower extremity: part 1, the pelvis and hip. Radiographics. 2010;30(4):983-1000. doi:10.1148/rg.304095135
-
Gomes BA, Ramos MRF, Fiorelli RKA. Topographic anatomical study of the sciatic nerve relationship to the posterior portal in hip arthroscopy. Rev Col Bras Cir. 2014;41(6):440-444. doi:10.1590/0100-69912014006010
-
Tomaszewski KA, Graves MJ, Henry BM, et al. Surgical anatomy of the sciatic nerve: a meta-analysis. J Orthop Res. 2016;34(10):1820-1827. doi:10.1002/jor.23186
-
Kaya K, Çekin N. Enjeksiyon sonrası gelişen nöropati: komplikasyon/malpraktis ayrımında ince bir çizgi. Kahramanmaras Sutcu Imam Univ Tip Fak Derg. 2018;13(2):63-66. doi:10.17517/ksutfd.394213
-
Park JW, Lee YK, Lee YJ, Shin S, Kang Y, Koo KH. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. Bone Joint J. 2020;102-B(5):556-567. doi:10.1302/0301-620x.102b5.bjj-2019-1212.r1
-
Navarro RA, Schmalzried TP, Amstutz HC, Dorey FJ. Surgical approach and nerve palsy in total hip arthroplasty. J Arthroplasty. 1995;10(1):1-5. doi:10.1016/s0883-5403(06)80057-4
-
Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequence: a review. Clin Anat. 2010;23(1):8-17. doi:10.1002/ca.20893
-
Poutoglidou F, Piagkou M, Totlis T, Tzika M, Natsis K. Sciatic nerve variants and the piriformis muscle: a systematic review and meta-analysis. Cureus. 2020;12(11). doi:10.7759/cureus.11531
-
Hernando MF, Cerezal L, Perez-Carro L, Abascal F, Canga A. Deep gluteal syndrome: anatomy, imaging, and management of sciatic nerve entrapments in the subgluteal space. Skeletal Radiol. 2015;44(7):919-934. doi:10.1007/s00256-015-2124-6
-
McCrory P, Bell S. Nerve entrapment syndromes as a cause of pain in the hip, groin and buttock. Sports Med. 1999;27(4):261-274. doi:10.2165/00007256-199927040-00005
-
Sawant SP. The study of division of sciatic nerve in 100 specimens with its clinical significance. Int J Sci Res. 2013;2(2):306-309.
-
Berihu BA, Debeb YG. Anatomical variation in bifurcation and trifurcations of sciatic nerve and its clinical implications: in selected university in Ethiopia. BMC Res Notes. 2015;8:633. doi:10.1186/s13104-015-1626-6
-
Marco C, Miguel-Perez M, Perez-Bellmunt A, et al. Anatomical causes of compression of the sciatic nerve in the pelvis: piriform syndrome. Rev Esp Cir Ortop Traumatol (Engl Ed). 2019;63(6):424-430.
-
Benli IT, Çapar B. Piriformis sendromu. J Turk Spinal Surg. 2011;22(3):215-222.
-
Khan H, Ling S, Ali S, et al. Sciatic nerve variants in patients diagnosed with sciatica: is there a correlation? J Comput Assist Tomogr. 2019;43(6):953-957. doi:10.1097/rct.0000000000000919
-
DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999;7(2):101-111. doi:10.5435/00124635-199903000-00003
Figures

Figure 1. NI morphometric distance measurements in the deep subgluteal space. 1. Diameter of NI at FI, 2. Distance between NI and TI, 3. Distance between TI and TM, 4. Distance between NI and TM, 5. Diameter of NI between TI and TM. Figure 1B. NI diameter in the bifurcation region

Figure 2. Measurements between FI and TM, SIAS, CI, SIPS, HS, TI reference points

Figure 3. Type A variation(1,2), Straight white arrrow: Single block MP (m. Piriformis), ovoid circle : single block NI ( n. İschiadicus). Type B variation (2, 3). NFC passes through the divided MP. Curved arrow: NFC (n. fibularis communis), asterix:NT ( n.tibialis)
Tables
Table 1. Modified Beaton-Anson variation classification
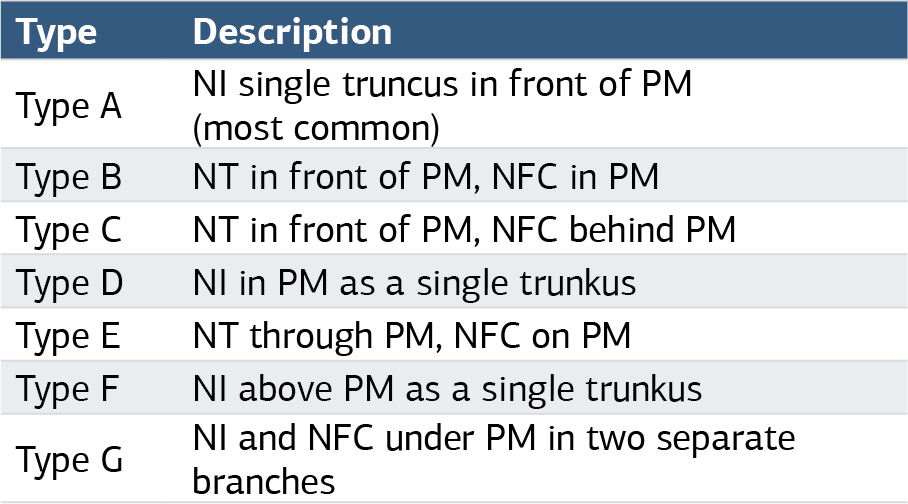
NI: nervus ischiadicus, PM: piriformis muscle, TN: tibialis nerve, NFC: Peronealis communis nerve
Table 2. Comparison of right and left side NI morphometric and topographic features and Mean ± SD data of both sides. No significant difference was observed between the right and left hip measurements (p>0.05)

NI: Nervus Ischiadicus, NIFI. Diameter of NI at the exit of FI. NITI: NI diameter at the TI, NIB: NI diameter at the bifurcation level, FI: Foramen infrapiriforme, TM: Trochanter major, SIAS: Spina iliaca anterior Superior, CI: Crista iliaca highest point, SIPS: Spina iliaca poste- rior superior, HS: Hiatus sacralis, TI: Tuber ischiadicum
Table 3. NI bifurcation levels
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ferhat Taş, Davut Özbağ, Murat Ögetürk, Zeynep Maraş Özdemir, Nur Betül Karatoprak, Furkan Çevirgen, Furkan Arpacı, Turgay Karataş. Nervus ischiadicus variations and clinical importance: a cadaver and MRI study . Ann Clin Anal Med 2025;16(1):10-14. doi:10.4328/ACAM.22161
- Received:
- February 28, 2024
- Accepted:
- July 29, 2024
- Published Online:
- October 29, 2024
- Printed:
- January 1, 2025