
Comparison of Hinchey classification with leukocyte and CRP values incolonic diverticular disease
CRP and WBC by Hinchey stage
Authors
Abstract
AimThe Hinchey classification helps determine the severity of diverticulitis. We investigated how inflammatory markers like white blood cell (WBC) count and C-reactive protein (CRP) levels vary across Hinchey stages.
MethodsWe analyzed data from patients surgically treated for colonic diverticular disease between 2018-2023. Data included demographics, disease characteristics, surgical approach, follow-up, and the link between WBC/CRP levels at presentation and Hinchey classification.
ResultsOur study included 50 patients (mean age 58.46, mostly male). Most diverticula were in the sigmoid colon (88%). WBC (p=0.012) and CRP (p=0.002) levels differed significantly across Hinchey stages. Pairwise comparisons showed higher CRP levels in Hinchey IV compared to stages I (p=.009) and III (p=.041). WBC levels were significantly higher in stage IV compared to stage II (p=0.012).
ConclusionIncreases in WBC and CRP levels, especially in Hinchey stage IV, highlight a stronger inflammatory response in advanced diverticulitis. These markers could potentially help assess disease severity and guide treatment decisions.
Keywords
Introduction
Diverticular disease is exceedingly common in Western societies, with epidemiological data documenting its prevalence above 60% in individuals over 65 years and between 60-80% in those over 80 years. Although most cases of colonic diverticular disease are asymptomatic, 10-25% of these patients may develop acute diverticulitis and other complications such as abscess, fistula, and perforation.1,2,3
In the emergency department (ED), early identification of patients with acute diverticulitis requiring urgent surgical intervention can be crucial for decision-making. The distinction between complicated and uncomplicated diseases carries significant clinical implications. The ability to accurately assess the severity of the condition can aid in clinical decision-making, such as determining the need for percutaneous drainage or surgical intervention, and evaluating hospital stay duration and antibiotic administration. The Hinchey classification is widely used to grade disease severity but is based on descriptive surgical findings and not designed for evaluating diverticulitis cases treated conservatively.4,5,6,7
Computed tomography (CT) plays a vital role in the ED for confirming diverticulitis, assessing complications, and ruling out alternative diagnoses. However, CT findings alone in all patients with acute diverticulitis in the ED may not predict the need for urgent surgical intervention. Serum inflammatory markers are utilized to differentiate the severity of acute diverticulitis and predict the need for surgical intervention. An optimum biochemical or hematological marker has not been established to determine disease severity in the diagnosis of diverticular disease or acute diverticulitis. White blood cell count (WBC) and C-reactive protein (CRP) values have been suggested to assist in distinguishing between complicated and uncomplicated acute diverticulitis.1,6,7,8
In this study, we aimed to investigate the correlation between WBC and CRP values and Hinchey classification in patients with the diverticular disease who underwent surgical treatment
Materials and Methods
Following the approval from the local ethics committee on December 8, 2023, under protocol number 139/38, this study included patients who underwent elective and emergent surgical treatment for diverticular disease of the colon in our clinic between January 2018 and January 2023. Patients with incomplete medical records, a pathology result indicating malignancy, and those under 18 years of age were excluded from the study. A dataset was created using electronic files and medical records, and data were retrospectively analyzed.
The analysis focused on demographic data such as age and gender, disease duration, number of attacks, location, history of percutaneous drainage, type and timing of operation, need for a stoma, postoperative complications, and WBC and CRP levels at presentation with diverticulitis episode and their correlation with Hinchey classification.
CT reports. Patients were classified into four stages according to the Hinchey classification, based on abdominal CT findings.9 The management of diverticular disease, both elective and emergency, at our institution followed the recommendations of the American Society of Colon and Rectal Surgeons.10
Ethical ApprovalThis study was approved by the Ethics Committee of Çukurova University (Date: 08.12.2023, Decision No:139/38).
Statistical AnalysisStatistical analysis was conducted using SPSS version 22.0. Categorical data were expressed as numbers (percentages). The normal distribution of numerical data was assessed using the Kolmogorov-Smirnov test. Numerical data conforming to normal distribution were expressed as mean ± standard deviation, while data not conforming were expressed as median (interquartile range). Comparisons between groups were made using the Kruskal-Wallis test. Pairwise comparisons were evaluated with Bonferroni correction. A p-value less than 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Our study included 50 patients with a mean age of 58.46, and a predominance of male gender (72%). The diverticula were most commonly located in the sigmoid colon (88%). Percutaneous drainage had been performed in 44% of the patients. Percutaneous drainage was administered to Hinchey 3 patients. Additionally, percutaneous drainage was applied to certain Hinchey 4 patients who were considered responsive to medical management and drainage. Some patients progressed to Hinchey 4 during the course of percutaneous drainage treatment. The most common Hinchey stage encountered was stage 4 (42%). Demographic and clinical characteristics are shown in Table 1.
Emergency admissions constituted 64% of the cases, and open surgery was more common, accounting for 70%. Stomas were created in 58% of the patients, with the rate of end colostomy being 38%. The most frequent complication was surgical site infection (18%). Perioperative period data are presented in Table 2.
Significant differences in WBC (p=0.012) and CRP levels (p=0.002) were found across the Hinchey stages. In pairwise comparisons to understand differences between groups, a significant increase in CRP levels was observed between Hinchey stages I and IV (adjusted p=.009) and stages III and IV (adjusted p=0.041). For WBC, a significant difference was noted between stages II and IV (adjusted p=0.012). These findings are illustrated in Figure 1, Figure 2 and Table 3.
Discussion
In this study, which investigated the relationship between the Hinchey score and inflammatory parameters (CRP and WBC) in patients with diverticular disease who underwent surgical treatment, we demonstrated a correlation between elevated CRP and WBC levels and higher Hinchey scores.
In acute diverticulitis, treatment options range from conservative to surgical interventions, depending on the patient’s condition and the severity of the disease. Literature indicates that while medical treatment is preferred in cases with lower Hinchey classification, surgical treatments are more likely chosen for cases in higher Hinchey stages.9,10 With advancements in treatment and approach, the Hinchey classification has gradually lost its importance in forming treatment protocols. Consequently, researchers have focused on identifying parameters that can be used in conjunction with or as an alternative to the Hinchey classification, aiming to predict disease progression more accurately.1,4,5,7,8
In their study on patients with acute left-sided colonic diverticulitis, Sağıroğlu and colleagues found a correlation with the Hinchey classification. Their multivariate analyses revealed that CRP was a marker of severity (p=0.001, 95% CI=0.036–0.147, OR=1.094).11 Mäkelä et al. identified a CRP value over 150 mg/L as an independent risk factor for acute left-sided colonic diverticulitis. A CRP value exceeding 150 mg/L, along with the presence of free intraperitoneal fluid on CT, was a predictor of postoperative mortality.2 Similarly, Kechogias et al., while examining CRP for predicting the severity of acute diverticulitis, found a correlation with the Hinchey classification.12 Another study indicated that a CRP level over 200 mg/L at presentation had a 69% positive predictive value for indicating the degree of inflammation and perforation in cases of acute diverticulitis, while a CRP level below 50 mg/L had a 79% negative predictive value, associating with lower levels of inflammation and reducing the likelihood of perforation.13 However, contrary to these published studies, when reviewing the literature, Elsing and colleagues found no statistically significant relationship between clinical severity and CRP levels in cases of acute diverticulitis.14 This suggests that while CRP can be a useful marker in many cases, its predictive value may not be universally applicable across all scenarios of diverticulitis, highlighting the need for a multifaceted approach in diagnosis and treatment planning.
Bokenstein et al., in their meta-analysis, revealed that both CRP and WBC were significant risk factors for acute complicated diverticulitis in all studies, although the levels of significance varied.15 In the study by Demircioglu et al., an elevation in WBC was shown to be associated with an increased risk of postoperative complications.16 Chang CY et al. demonstrated a correlation between elevated WBC and complicated diverticulitis.17 Kechagias A et al. in their series, showed a relationship between inflammatory markers CRP and WBC and the Hinchey score, with higher values observed in patients with Hinchey stages 3-4.18 Conversely, from a different perspective in the literature, Kargın et al. examined the diagnostic and prognostic value of inflammatory parameters in acute diverticulitis and reported no significant difference between the Hinchey groups in terms of CRP-WBC, stating that WBC-CRP was not a useful parameter for making surgical decisions.8 Similarly, another study found that WBC did not predict treatment selection in patients with acute diverticulitis.19
Given the severity of inflammation in complicated diverticulitis, it is not surprising to find high biomarkers known as positive acute phase reactants correlating with disease severity. In our study, we demonstrated this correlation with disease severity.
Limitations
The limitations of our study include its single-center, retrospective nature, and the relatively limited number of patients.
Conclusion
In conclusion, particularly in Hinchey Stage IV, the increase in WBC and CRP levels indicates a heightened inflammatory response in the advanced stages of diverticulitis. These findings highlight the potential of these markers in assessing disease severity and guiding clinical interventions. This underscores the importance of considering these biomarkers in the management and treatment planning of diverticulitis, especially in its more severe forms.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
AI Usage Disclosure
The authors declare that no AI-assisted technologies were used.
Abbreviations
CRP: C-reactive protein
CT: Computed tomography
ED: Emergency department
WBC: White blood cell
References
-
Mäkelä JT, Klintrup K, Takala H, Rautio T. The role of C-reactive protein in prediction of the severity of acute diverticulitis in an emergency unit. Scand J Gastroenterol. 2015;50(5):536-541. doi:10.3109/00365521.2014.999350
-
Standards Committee of the American Society of Colon and Rectal Surgeons, Rafferty J, Shellito P, Hyman NH, Buie WD. Practice parameters for sigmoid diverticulitis. Dis Colon Rectum. 2006;49(7):939-944. doi:10.1007/s10350-006-0578-2
-
Stollman N, Raskin JB. Diverticular disease of the colon. Lancet. 2004;363(9409):631-639. doi:10.1016/s0140-6736(04)15597-9
-
van de Wall BJM, Draaisma WA, van der Kaaij RT, Consten ECJ, Wiezer MJ, Broeders IAMJ. The value of inflammation markers and body temperature in acute diverticulitis. Colorectal Dis. 2013;15(5):621-626. doi:10.1111/codi.12072
-
Nizri E, Spring S, Ben-Yehuda A, Khatib M, Klausner J, Greenberg R. C-reactive protein as a marker of complicated diverticulitis in patients on anti-inflammatory medications. Tech Coloproctol. 2014;18(2):145-149. doi:10.1007/s10151-013-1044-5
-
Kaser SA, Fankhauser G, Glauser PM, Toia D, Maurer CA. Diagnostic value of inflammation markers in predicting perforation in acute sigmoid diverticulitis. World J Surg. 2010;34(11):2717-2722.
-
Kang HS, Cha YS, Park KH, Hwang SO. Delta neutrophil index as a promising prognostic marker of emergent surgical intervention for acute diverticulitis in the emergency department. PLoS One. 2017;12(11). doi:10.1371/journal.pone.0187629
-
Kargın S, Tanrıkulu Y. Diagnostic and prognostic significance of inflammatory parameters in acute diverticulitis: a retrospective cohort study. Ulus Travma Acil Cerrahi Derg. 2021;27(3):325-330.
-
Kaiser AM, Jiang JK, Lake JP, et al. The management of complicated diverticulitis and the role of computed tomography. Am J Gastroenterol. 2005;100(4):910-917. doi:10.1111/j.1572-0241.2005.41154.x
-
Al-Sahaf O, Al-Azawi D, Fauzi MZ, El-Masry S, Gillen P. Early discharge policy of patients with acute colonic diverticulitis following initial CT scan. Int J Colorectal Dis. 2008;23(8):817-820. doi:10.1007/s00384-008-0492-2
-
Sağıroğlu J, Beyazadam D, Gök AFK, et al. Factors predicting severity level, progression and recurrence risk of acute left colonic diverticulitis in Turkey: a multicenter study. Ulus Travma Acil Cerrahi Derg. 2021;27(1):132-138.
-
Kechagias A, Rautio T, Kechagias G, Mäkelä J. The role of C-reactive protein in the prediction of the clinical severity of acute diverticulitis. Am Surg. 2014;80(4):391-395. doi:10.1177/000313481408000423
-
Tan JP, Barazanchi AW, Singh PP, Hill AG, Maccormick AD. Predictors of acute diverticulitis severity: a systematic review. Int J Surg. 2016;26:43-52. doi:10.1016/j.ijsu.2016.01.005
-
Elsing C, Ernst S, Stremmel W. Value of lipopolysaccharide binding protein, interleukin-6 and C-reactive protein as biomarkers of severity in acute diverticulitis: a prospective study. Clin Lab. 2012;58(1-2):145-151.
-
Bolkenstein HE, van de Wall BJM, Consten ECJ, Broeders IAMJ, Draaisma WA. Risk factors for complicated diverticulitis: systematic review and meta-analysis. Int J Colorectal Dis. 2017;32(10):1375-1383. doi:10.1007/s00384-017-2872-y
-
Demircioglu MK, Demircioglu ZG, Celayir MF, Kaya C, Mihmanli M. The effects of diverticulum localization and Hinchey classification on recurrence and complications in acute colonic diverticulitis. Sisli Etfal Hastan Tip Bul. 2020;54(4):451-456. doi:10.14744/semb.2020.03453
-
Chang CY, Hsu TY, He GY, et al. Utility of monocyte distribution width in the differential diagnosis between simple and complicated diverticulitis: a retrospective cohort study. BMC Gastroenterol. 2023;23(1):96. doi:10.1186/s12876-023-02736-0
-
Kechagias A, Sofianidis A, Zografos G, Leandros E, Alexakis N, Dervenis C. Index C-reactive protein predicts increased severity in acute sigmoid diverticulitis. Ther Clin Risk Manag. 2018;14:1847-1853. doi:10.2147/tcrm.s160113
-
Bates DD, Fernandez MB, Ponchiardi C, et al. Surgical management in acute diverticulitis and its association with multidetector CT, modified Hinchey classification, and clinical parameters. Abdom Radiol. 2018;43(8):2060-2065. doi:10.1007/s00261-017-1422-y
Figures
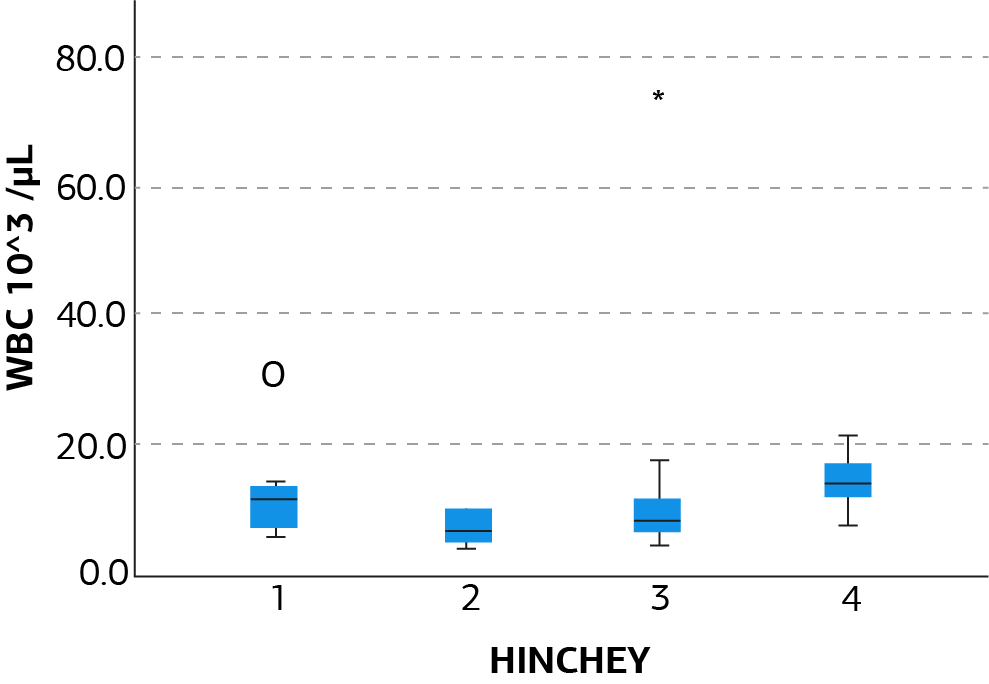
Figure 1. Correlation of WBC and Hinchey classification
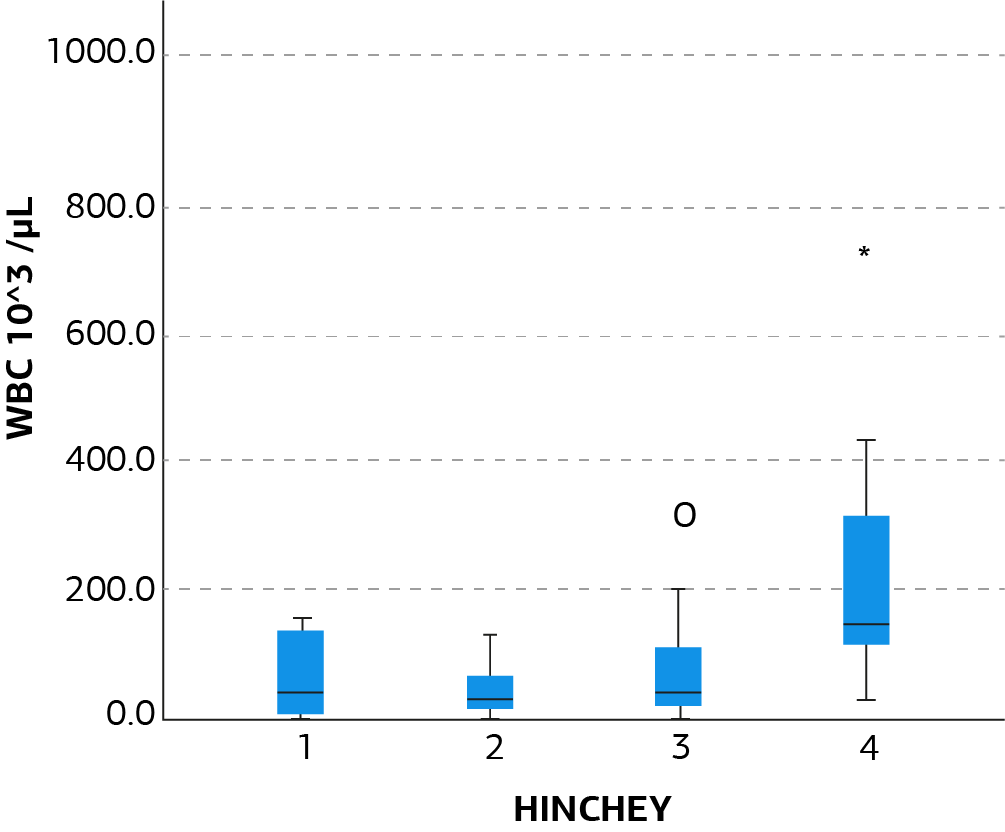
Figure 2. Correlation of CRP and Hinchey classification
Tables
Table 1. Demographical and clinical data

Table 2. Perioperative data
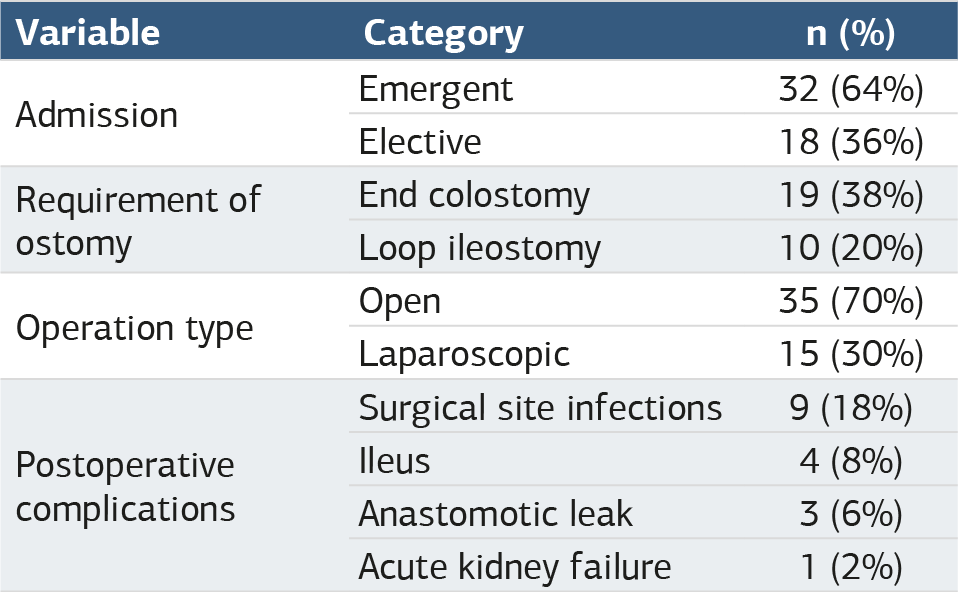
Table 3. Comparison of WBC and CRP across Hinchey classification groups
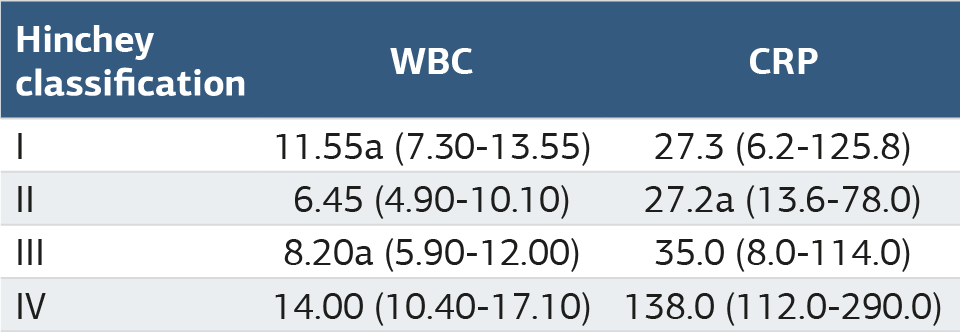
a: Statistically significant difference with Hinchey IV
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İshak Aydın, Uğur Topal, Batuhan Kaya, Yunus Kaycı, Burak Yavuz, Orçun Yalav, İsmail Cem Eray. Comparison of Hinchey classification with leukocyte and CRP values incolonic diverticular disease. Ann Clin Anal Med 2025;16(1):6-9. doi:10.4328/ACAM.22180
- Received:
- March 14, 2024
- Accepted:
- May 13, 2024
- Published Online:
- August 18, 2024
- Printed:
- January 1, 2025