
Evaluation of percutaneous fiducial marker placement under computedtomography guidance for stereotactic radiotherapy for lung lesions
Fiducial marker for stereotactic radiotherapy to lung lesions
Authors
Abstract
AimWe aimed to observe the feasibility and technical aspects of percutaneous fiducial marker placement in lung lesions for Sterotactic Radiotherapy, to investigate its complications, how these complications can be reduced, and whether there is a relationship between them.
MethodsThis retrospective study included patients who underwent percutaneous reference marker placement in lung lesions under CT guidance between 2017 and 2019. The study included 32 patients, 34 lesions and 98 fiducials, and 2 patients had 2 lesions. Images of the cases taken during the procedure and during follow-up were examined and any complications that developed were recorded. The data were analyzed with Mann Whitney U test and Fisher’s Exact test.
ResultsA statistically significant relationship was found between migration and tract length, and tract length was found to be shorter in the migration group. In our study, migration was observed in only 8 of 98 fiducials. The most common complication was pulmonary hemorrhage with 73.5%. Other complications were mild pneumothorax in 44.1%, chest tube insertion pneumothorax in 11.7%, migration in 11.7%, subcutaneous emphysema in 8.8% and hemothorax in 5.8%. There was no significant difference in lesion volume and fiducial distance between those with and without migration.
ConclusionCT-guided fiducial placement can be performed successfully in lung lesions, which ensures that normal tissues around the lesion are exposed to less radiation during treatment. Complications that develop are generally self-limiting and do not require intervention. For this reason, it can be applied to every patient without contraindications.
Keywords
Introduction
Radiosurgery was first developed for the treatment of wellcircumscribed brain metastases using high radiation doses.1 Because of their fixed position, consistent doses can be delivered to these lesions. When this technique is specifically modified to treat lung tumors, accurate delivery of radiation doses becomes difficult as a result of tumor movement due to respiration. On the other hand, it causes increased toxicity in the surrounding tissue. To prevent this situation, stereotactic localization techniques have been developed.2
Stereotactic radiotherapy (SRT) is the application of high doses of radiation to a stereotactically marked target volume in single or small fractions. It provides serious advantages over other radiotherapy techniques, especially in dose distribution in target volumes smaller than 4 cm. It has the ability to send beams to the target from many different angles. Thus, while the highest dose is given to the target volume, sudden dose reductions are provided right next to the tumor and the surrounding tissues are protected. To determine the target volume before treatment and to monitor the target volume radiographically during treatment, special metallic markers, called fiducials and usually made of stainless steel or gold, are placed in and/or around the tumor. The device checks the position of the target each time before irradiation begins.3
Computed Tomography (CT) and multislice computed tomography (MSCT), which are high-resolution, fast crosssectional imaging methods, are the most frequently used methods after direct roentgenogram in thoracic examinations. MSCT systems allow taking many thin-section images much faster than conventional CT systems and performing threedimensional evaluation by reformating these images.4 CT is also valuable in guiding percutaneous biopsy and fiducial placement of lung lesions. During these procedures, CT provides very important information in evaluating the lesion, predicting risks and complications, determining the needle plane, determining the needle entry site and detecting post-procedure complications.5 Fiducials are small gold marks that are implanted into the soft tissues or inside the lesion. They provide spatial information for the system to accurately direct radiation distribution. Gold is denser than surgical clips and appears unique on imaging with characteristic line artifacts. Fiducials are typically required for tumors in the chest, abdomen, pelvis, or other soft tissues. Ideally, a fiducial should be centered on the treatment area (at the center of the lesion).6 In this study, we aimed to determine the complications of fiducial placement performed percutaneously under computerized tomography (CT) guidance for the purpose of SRT.
Materials and Methods
This study was conducted by Dr. Abdurrahman Yurtaslan Ankara Oncology Health Application and Research Center Department of Radiology between 09.13.2017-11.26.2019. Patients who underwent percutaneous reference marker placement in lung lesions under CT guidance were included in the study. The study included 32 patients, 34 lesions and 98 fiducials, and 2 patients had 2 lesions. Images of the cases taken during the procedure and during follow-up were examined and any complications that developed were recorded. Before the procedure, the purpose of the procedure and possible complications were explained to all patients, and an informed consent form was obtained from all patients.
Before starting the procedure, the patients’ existing images (such as CT, PET) were evaluated and the position of the patients was determined accordingly.
Sections were taken from a limited area with the patient in the determined position. The section where the lesion was located was marked on the sections taken and re-sections were taken with a segmented opaque marker placed on the skin. Based on the sections taken, it was determined from which compartments the needle would be inserted. After the skin was cleaned and sterilized with a povidone iodide solution, local anesthesia was applied to the relevant areas. In the light of the images obtained, the needle was advanced to the desired length in the skin, subcutaneous and soft tissues with the needle angle appropriate to the targeted area. Needles that were not in the appropriate position were re-pulled to ensure they were positioned appropriately. The needles in appropriate positions were advanced into the lung tissue to the determined length.
In the sections taken later, if the needle was far from the target, it was withdrawn and if it was close, it was pushed to reach the determined localization. When the needle reached the targeted area, fiducial markers were placed into the tissue. Afterwards, the fiducial location and complication status were determined by taking a CT image without changing the patient’s position. It was planned to place at least 3 fiducials in all patients. Failure to place any of the fiducials was considered procedure failure. In addition, placement of at least one fiducial within or 2 cm close to the lesion was considered a success of the procedure.
Ethical ApprovalThis study was approved by the Ethics Committee of the Dr. Abdurrahman Yurtaslan Ankara Oncology Health Application and Research Center (Date: 13.01.2021, Decision No: 2021-01/941).
Statistical AnalysisQuantitative data were summarized with mean±standard deviation and median (minimum-maximum), and qualitative data were summarized with frequency and percentage, n(%). In addition, descriptive statistics were presented. Gender, age, primary/metastasis variables were evaluated based on the number of patients (n = 32). Lobe and complication variables are based on the number of lesions (n = 34); Fiducial lesion distance, fiducial number and migration variables were evaluated based on fiducial number (n = 98). Comparisons between groups were made using the Mann Whitney U test for quantitative data and Fisher’s Exact test for qualitative data. p<0.05 value was considered statistically significant. R v.3.6.3 statistical programming language was used for analyses
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
At least one fiducial was placed in or around all lesions, and the success of the procedure was found to be 100%. Of the 32 patients included in the study, 25 (78.1%) were male and 7 (21.9%) were female, the average age was 62.6±10 (min: 37- max: 83). 17 (53.1%) of the patients were detected as primary and 15 (46.9%) as metastasis. In the study, the lesion requiring fiducial placement was most frequently encountered in the eft upper lobe (32.4%), while the right middle lobe lesion was observed least frequently (11.8%). In terms of complications, pulmonary hemorrhage was the most common complication and was observed in 25 lesions, mild pneumothorax in 15 lesions, pneumothorax with chest tube insertion in 4 lesions, migration in 4 lesions, and subcutaneous emphysema in 3 lesions. The least observed complication was hemothorax (n = 2). No complications were observed in 4 lesions.
While there were 55 (56.1%) fiducials with fiducial lesion distance of 1-20 mm, there were 32 (32.7%) on the edge, 7 (7.1%) with 21-40 mm and 4 (4.1%) inside. There were 27 (79.4%) lesions with a fiducial number of 3 placed in one lesion, 3 (8.8%) with 1, 3 (8.8%) with 4 and 1 (2.9%) with 2 lesions. Tract length was found to be statistically significantly lower in the group with migration than in those without [respectively, median (min-max): 8.5(0-28); 22.5(0-71); p=0.015]. There was no statistically significant difference between those with and without migration in terms of lesion volume and fiducial distance (p=0.755, p=0.299, respectively) (Table 1).
The relationship between procedure termination due to pneumothorax and total pneumothorax and fiducial termination type was examined. Of the 31 fiducials for which no procedure termination was observed due to pneumothorax, 21 (67.7%) were placed using FRM 1 (Figure 1), where the needle is removed after the first fiducial is placed and the same process is repeated for the subsequent fiducials. The remaining 10 (32.3%) were placed using FRM 2 (Figure 2), where the needle is not removed after the first fiducial is placed and the needles are removed together after the other necessary fiducials are placed. All 3 fiducials in which procedure termination was observed due to pneumothorax had fiducial release method 1 (p=0.539). Of the 15 fiducials in which no pneumothorax was observed, 4 (26.7%) had FRM 2 and 11 (73.3%) FRM 1. Of the 19 fiducials with total pneumothorax, 6 (31.6%) had FRM 2 and 13 (68.4%) had FRM 1 (p=1.000) (Table 2). Rates of total pneumothorax numbers were 6/7 (85.7%) in the right upper lobe, 3/4 (755%) in the right middle lobe, 2/5 (40%) in the right lower lobe, 4/11 (36.4%) in the left upper lobe, 4/11 (36.4%) in the left lower lobe. In the lobe, it was 4/7 (57.1%) (p=0.282).
Discussion
Stereotactic radiosurgery refers to the precise delivery of a highly concentrated radiation dose to a small target area in one session, minimizing radiation exposure to the surrounding healthy tissue under three-dimensional computerized imaging.7 Fiducials are markers made of 99% gold, 5 mm long and 0.5 mm in diameter, that are implanted by interventional radiologists on an outpatient basis through CT-guided preloaded fiducial needles or aspiration needles.8 In this study, we investigated the complications arising from fiducial placement in lung lesions and the relationship between the complications. In order to apply stereotactic radiotherapy to lung lesions, a marker must be placed in the lung parenchyma. However, the fact that the lung parenchyma is largely filled with air causes the markers to not remain fixed in place and to be easily separated. Therefore, reimplantation using new fiducials becomes necessary. This situation reduces the chance of stereotactic radiotherapy and makes it necessary to switch to conventional radiotherapy. In the literature, Harada et al. in their study examining the feasibility of real-time tumor monitoring radiation therapy (RT) treatment in lung cancer patients, reported that 5 of 19 fiducial markers placed by bronchofiberoscopy migrated and the migration rate was 26%.9 Moreover, they also reported that they successfully treated 13 (65%) of 20 tumors in total with RT. They concluded that the excellent initial response and low incidence of clinical complications suggest that high-dose hypofractionated focal irradiation using the RT system may be a good local treatment for peripheral-type lung tumors.
In the study by Imura et al. the fixation rate of markers using the bronchial placement technique, the reliability of the setup using markers around the target volume, the dislocation of markers after real-time tumor tracking RT, and the long-term toxicity of marker placement were investigated. They reported that gold markers were detected in 115 of 154 markers (75%) during the treatment period. As a result of their research, they hypothesized that the relationship between the markers and tumor can change significantly after 2 weeks, suggesting that adaptive four-dimensional RT is required.10 In our study, 8 fiducials placed in 4 lesions were shown to migrate, which is consistent with the literature. In our study, we concluded that there is no need to stay away from this procedure due to the risk of migration.
On the other hand, there are also studies in the literature that report migration rates at very low levels. De Mey et al. In their study evaluating a technique for implanting radiopaque markers into lung nodules as an adjunct to extracranial stereotactic radiation therapy reported that no markers migrated. As a result of the study, they concluded that lung nodules can be marked safely and accurately with radiopaque implants with this technique.11 Similarly, in the study published by Patel et al., the rate of migrating markers was reported as 4%, and in the study published by Kothary et al., it was reported as 9%.12,13 In our study, it was determined that 8 fiducials placed in 4 lesions migrated. Our rates were found to be 11% on a lesion basis and 8% on a fiducial basis, which are similar to the literature. When we look at the migration rate we obtained in our study and the migration rates obtained in the literature, we think that there is no need to stay away from the application of this procedure due to the risk of migration.
In the present study, it was determined that there was a statistically significant relationship between tract length and migration rates. Accordingly, tract length was found to be statistically significantly lower in the migration group compared to the non-migration group. We concluded that the reason for this situation may be due to the fact that the fiducials were placed without passing the visceral pleura. In addition, we thought that the fact that migrating fiducials are seen in very distant areas in some cases is due to the fact that this potential space into which the fiducials fall is the pleural space and that the fiducial can escape to any point within this space. We think that when placing fiducials into the lung parenchyma, it would be beneficial to adjust the tract distance to be long and complete the release process after ensuring that the visceral pleura is passed. In our study, the relationship between migration and lesion volume, lesion fidusial distance, pneumothorax and lobar anatomy where the lesion is located was examined. No statistically significant difference was detected between migration and parameters. Another important issue discussed in the literature regarding fiducial placement in lung lesions is the risk of pneumothorax complications. The majority of these are mild pneumothorax cases that show rapid regression as a result of follow-up. In the study by Bhagat et al. the mild pneumothorax rate was reported to be 82% when an 18G needle was used for fiducial placement, 40% when a 19G needle was used, and 67% in total.1 In our study, the needles used for fiducial insertion were 19G, and we found our total pneumothorax rate to be 55%, similar to these studies.
The most common procedure for placing fiducial markers in lung lesions is pulmonary hemorrhage (PH). Similarly, in our study, the most common complication was PH. In the literature, PH rates vary significantly. It was found to be 67% in the study of Ohta et al., 33% in the study of Trumm et al., and 18% in the study of Kothary et al.14,15,16 In our study, this rate was found to be 73.5%. We think that the reason for this difference may be due to the difference in the number of fiducials placed per lesion and the tract length. As the number of fiducials and tract length increases, the amount of damaged tissue will increase and the likelihood of hemorrhage will increase. In our study, the pulmonary hemorrhages that occurred in our patients were mild and local, self-limited, and did not cause any problems in the follow-up of the patients.
In our study, a rare hemothorax complication was detected in 2 patients and its rate was 5.8%. In addition, subcutaneous emphysema was observed in 2 of our patients. This complication was detected during the fiducial placement procedure in 3 lesions and our rate was 8%. Total pneumothorax and migration with the lung lobe where the lesion is located no statistically significant difference was detected between them. We think that the development of pneumothorax is not related to the lesion location. While the FMR 1 was previously used in the fiducial placement process at the center where the study was conducted, it was later switched to the FMR 2 with the idea that we could reduce the possibility of pneumothorax. After this method change, fewer cases of pneumothorax were encountered with fiducial release method 2. As a result of no pneumothorax developing after the first fiducials placed using the FMR 2, other fiducials were placed. For this reason, we think that using the FMR 2 is a more accurate approach when placing fiducial markers in the lung.
Limitations
This retrospective, single-center study with a small sample size and no long-term follow-up may limit generalizability.
Conclusion
As a result of the study, fiducial placement of lung lesions via CT was successfully performed. The complications that occur are at a limiting level that do not require intervention. Although no pneumothorax requiring procedure termination was observed with the FMR 2 in the study, we think that it would be very useful to conduct prospective multicenter studies with more patients. In addition, we concluded that in order to reduce migration rates, paying attention to the tract length and making sure that the visceral pleura is passed is the best approach.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CT: Computed tomography
FRM: Fiducial release method
MSCT: Multislice computed tomography
PET: Positron emission tomography
RT: Radiotherapy
SRT: Stereotactic radiotherapy
References
-
Bhagat N, Fidelman N, Durack JC, et al. Complications associated with the percutaneous insertion of fiducial markers in the thorax. Cardiovasc Intervent Radiol. 2010;33(6):1186-1191. doi:10.1007/s00270-010-9949-0
-
Abreu CE, Ferreira PP, de Moraes FY, et al. Stereotactic body radiotherapy in lung cancer: an update. J Bras Pneumol. 2015;41(4):376-387. doi:10.1590/s1806-37132015000000034
-
Csiki E, Simon M, Papp J, et al. Stereotactic body radiotherapy in lung cancer: a contemporary review. Pathol Oncol Res. 2024;30:1611709. doi:10.3389/pore.2024.1611709
-
Beigelman-Aubry C, Dunet V, Brun AL. CT imaging in pre-therapeutic assessment of lung cancer. Diagn Interv Imaging. 2016;97(10):973-989. doi:10.1016/j.diii.2016.07.010
-
Hawkes White E, Boswell W, Whang G, et al. CT-guided fiducial marker placement for stereotactic radiosurgery. Appl Radiol. 2011;40(5):24. doi:10.37549/ar1823
-
Sotiropoulou E, Stathochristopoulou I, Stathopoulos K, et al. CT-guided fiducial placement for cyberknife stereotactic radiosurgery: an initial experience. Cardiovasc Intervent Radiol. 2010;33(3):586-589. doi:10.1007/s00270-009-9748-7
-
Chang JY, Senan S, Paul MA, et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: a pooled analysis of two randomised trials. Lancet Oncol. 2015;16(6):630-637. doi:10.1016/s1470-2045(15)70168-3
-
Casutt A, Kinj R, Ozsahin EM, et al. Fiducial markers for stereotactic lung radiation therapy: review of the transthoracic, endovascular and endobronchial approaches. Eur Respir Rev. 2022;31(163):210149. doi:10.1183/16000617.0149-2021
-
Imura M, Yamazaki K, Shirato H, et al. Insertion and fixation of fiducial markers for setup and tracking of lung tumors in radiotherapy. Int J Radiat Oncol Biol Phys. 2005;63(5):1442-1447. doi:10.1016/j.ijrobp.2005.04.024
-
de Mey J, Van de Steene J, Vandenbroucke F, et al. Percutaneous placement of marking coils before stereotactic radiation therapy of malignant lung lesions. J Vasc Interv Radiol. 2005;16(1):51-56. doi:10.1097/01.rvi.0000142599.48497.6b
-
Patel A, Khalsa B, Lord B, et al. Planting the seeds of success: CT-guided gold seed fiducial marker placement to guide robotic radiosurgery. J Med Imaging Radiat Oncol. 2013;57(2):207-211. doi:10.1111/j.1754-9485.2012.02445.x
-
Casamassima F, Cavedon C, Francescon P, et al. Use of motion tracking in stereotactic body radiotherapy: evaluation of uncertainty in off-target dose distribution and optimization strategies. Acta Oncol. 2006;45(7):943-947. doi:10.1080/02841860600908962
-
Yousefi S, Collins BT, Reichner CA, et al. Complications of thoracic computed tomography-guided fiducial placement for the purpose of stereotactic body radiation therapy. Clin Lung Cancer. 2007;8(4):252-256. doi:10.3816/clc.2007.n.002
-
Kothary N, Heit JJ, Louie JD, et al. Safety and efficacy of percutaneous fiducial marker implantation for image-guided radiation therapy. J Vasc Interv Radiol. 2009;20(2):235-239. doi:10.1016/j.jvir.2008.09.026
-
Ohta K, Shimohira M, Iwata H, et al. Percutaneous fiducial marker placement under CT fluoroscopic guidance for stereotactic body radiotherapy of the lung: an initial experience. J Radiat Res. 2013;54(5):957-961. doi:10.1093/jrr/rrt020
-
Trumm CG, Häussler SM, Muacevic A, et al. CT fluoroscopy-guided percutaneous fiducial marker placement for CyberKnife stereotactic radiosurgery: technical results and complications in 222 consecutive procedures. J Vasc Interv Radiol. 2014;25(5):760-768. doi:10.1016/j.jvir.2014.01.004
Figures

Figure 1. CT with axial lung window image of the fiducial needle placed with fiducial release method 1

Figure 2. CT with axial maximum intensity projection reconstruction image of fiducial needles placed with fiducial release method 2
Tables
Table 1. Relationship between migration and tract length, lesion volume and fiducial lesion distance
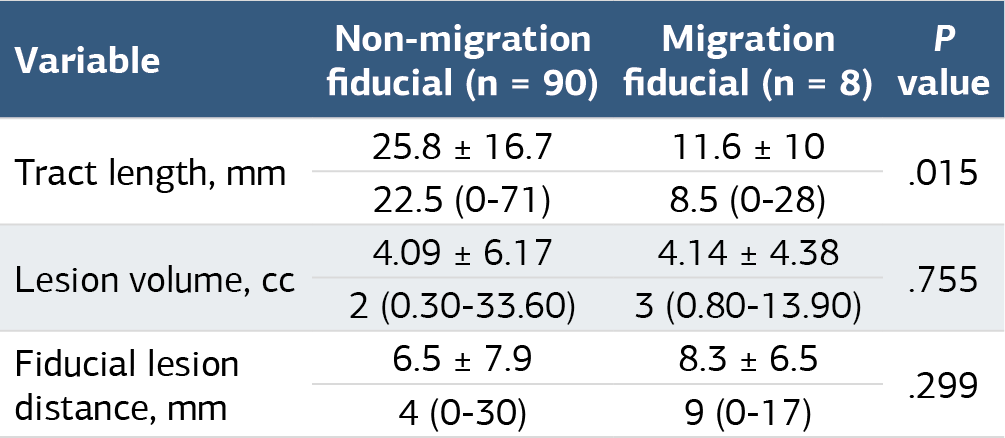
Mean±standard deviation and median (minimum-maximum) values are given for quantitative variables, and frequency and percentage, n(%), values are given for qualitative variables. p values were obtained as a result of the Mann Whitney U test
Table 2. Comparisons between fiducial release form

Frequency and percentage, n(%), values are given. p values were obtained as a result of Fisher's Exact test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mehmet Erdal, Ahmet Bayrak, Çetin İmamoğlu. Evaluation of percutaneous fiducial marker placement under computedtomography guidance for stereotactic radiotherapy for lung lesions. Ann Clin Anal Med 2025;16(1):36-40. doi:10.4328/ACAM.22182
- Received:
- April 4, 2024
- Accepted:
- May 27, 2026
- Published Online:
- November 11, 2024
- Printed:
- January 1, 2025