
An innovative approach: prompt withdrawal of the drain allows for fistula closure in some prolonged postoperative pancreaticobiliary fistulas
The drain itself prevents the fistula from closing
Authors
Abstract
AimIn the literature, there are different approaches to the treatment of postoperative pancreaticobiliary fistulas. In this study, we present our clinical experience, emphasizing that drains can prevent the closure of some fistulas.
MethodsIn patients with fistulas, drain flow was monitored until the fistula tract developed. In general, we waited until the 15th day to ensure that the fistula tract fully matured. Then, we promptly removed the drain without replacing or shortening it. The patients were followed up with clinical and imaging methods.
ResultsWe had a total of 20 patients with pancreaticobiliary fistulas. The mean age of the patients was 44.6 (10-81) years. Fifteen (75%) patients were male, and five (25%) were female. Twelve patients had pancreatic fistulas, and eight had biliary fistulas. Especially in patients with biliary fistulas, we removed the drains according to the criteria we determined. After the drain was removed, no clinically or radiologically negative finding was detected in any of the patients.
ConclusionWe consider that our experience based on a limited number of patients will contribute to the literature by presenting the thesis that the drain itself prevents fistula closure in some patients.
Keywords
Introduction
In general surgery, a fistula is a tract with two mouths that connects two epithelial surfaces and is covered with granulation tissue. There are important issues in the management of patients with fistulas, including the content, duration, and length of fistulas, the surfaces between which the fistula develops, continuous or intermittent functioning of the fistula, flow rate, and whether it develops after surgery. The fistula may contain bile, intestinal content, pus, blood, pancreatic fluid, and lymph fluid. Sometimes only one type of content may come from the fistula, whereas two (bile and pancreatic fluid), three or mixed contents may also come from it.1,2,3 Perianal fistulas are beyond the scope of the current study.
Fistulas are surgeons’ nightmare. The conservative closure of fistulas is a time-consuming process. It can be worrying for both the patient and the physician. In general, fistulas first have a period of leakage, followed by a period of fistula formation. Especially in postoperative fistulas, there is usually a drain at the surgical site. In these cases, the emergence, displacement, or obstruction of the drain may lead to a fluid accumulation, requiring drainage and a clinical picture that may lead to sepsis. Our experience has shown that in some patients, a prolonged drain stay causes the fistula to persist. We have observed that in these cases, fistulas close abruptly in the event of the rapid or accidental removal of the drain. However, we cannot attribute the cause of every prolonged fistula to the presence of a drain. For example, in Strasberg type E bile duct injuries, the drain cannot be considered a cause of fistulas. We have experienced that the rapid withdrawal of the drain provides the closure of biliary fistulas (BFs) in some cases with minimal bile duct damage, some pancreatic fistulas (PFs), patients with bile leakage after hepatectomies, and in selected patients that meet certain criteria after the fistula tract is fully formed.
In this paper, we present a novel approach to the management of pancreaticobiliary fistulas (PBFs) that developed after abdominal surgery. We attempted to close the fistulas by withdrawing the drains promptly. Since this method has not been previously reported in the literature, our study is the first of its kind.
Materials and Methods
Trial DesignThis retrospective study was carried out at the General Surgery Department of the University of Health Sciences Konya City Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the principles of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Participants and Eligibility CriteriaPatients who underwent hepatobiliary and pancreatic surgery in our clinic between January 1, 2016, and January 1, 2021 were screened from patient files, and those who developed postoperative PBFs were identified. Patients with other fistulas were excluded from the study. Among the patients with PBFs, only those who were followed up and treated with the method we described were included in the sample.
We used the following criteria for the decision to promptly withdraw the drains in patients with BFs:
1) Normal liver function test values.
2) Absence of septic findings.
3) Presence of defecation.
4) Fistula flow rate not exceeding 250-400 cc/day.
5) No signal loss, such as full-thickness incision on MRCP
6) Absence of suspicious findings, such as aberrant canal injury on MRCP.
7) No type E damage according to the Strasberg classification (only minor injuries were included).
8) Persistence of the fistula despite ERCP (papillotomy + stenting).
9) Maturity of the fistula tract (at least two weeks after the fistula begins to develop).
OutcomesFrom the patient files, demographic information, clinical data, and laboratory and radiological records were obtained and analyzed.
Ethical ApprovalThis study was approved by the Ethics Committee of Hamidiye Institute of Health Sciences (Date: 26.11.2021, Decision No: 21-695).
Statistical AnalysisDescriptive statistics, including mean, standard deviation, median, minimum, maximum, frequency, and percentage values were obtained. For statistical analyses, the Statistical Package for the Social Sciences (SPSS), version 22.0 (SPSS Inc., Chicago, IL, USA) was used.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
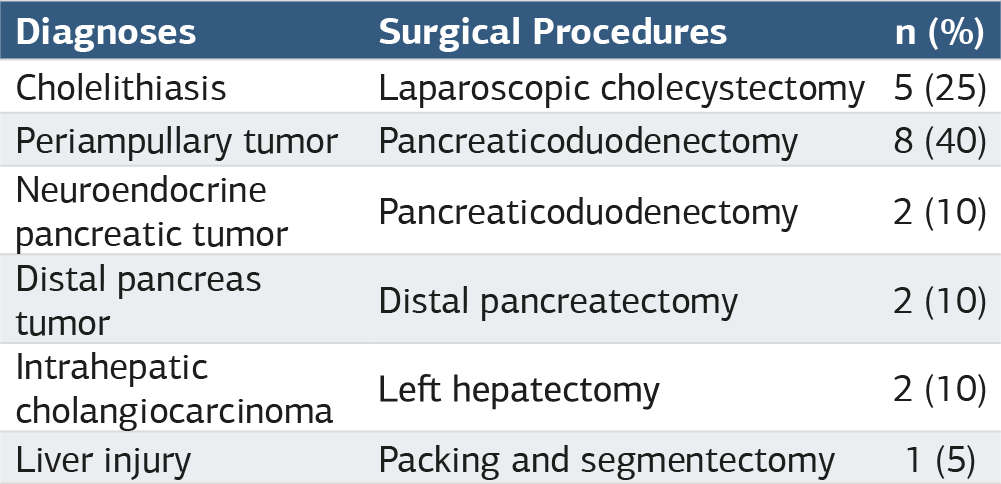
From January 1, 2016, through January 1, 2022, 3.856 laparoscopic cholecystectomy (LC), 97 pancreaticoduodenectomy (PD), 21 distal pancreatectomy (DP), and 18 hepatectomy procedures were performed in our clinic. Postoperative PBFs developed in 43 of these patients. After excluding the 23 cases in which other follow-up and treatment methods were used, 20 patients were included in the study. Twelve patients developed PFs and eight developed BFs. The flow diagram of the study is shown in Figure 1. The mean age of the patients was 44.6 years. Fifteen (75%) of the 20 patients were male, and five (25%) were female. The demographic characteristics of the patients are given in Table 1, and their diagnoses and the surgical procedures performed are summarized in Table 2. Additional interventional procedures were required in only five patients (5/20, 25%), of whom two underwent endoscopic retrograde cholangiopancreatography (ERCP) (2/20, 10%) and three underwent percutaneous drainage (3/20, 15%). Figure 2 presents the fistulography image of a case in which stenting was performed with ERCP for bile leakage. No additional intervention was undertaken in any of the remaining patients. Eight patients had prolonged BFs. Five of these patients underwent LC for symptomatic cholelithiasis, two had hepatectomies with the diagnosis of intrahepatic cholangiocarcinoma, and one underwent packing and segmentectomy due to traumatic liver injury. All of these patients had BFs persisting for weeks at different flow rates. In these cases with persistent fistulas, we attempted to promptly withdraw the drains and observed that all the fistulas were closed. There was no biloma or sepsis during hospital stay and outpatient follow-up after discharge.
Eight patients with periampullary tumors and two with pancreatic neuroendocrine tumors developed PFs after PD, and two patients developed PFs after DP. Amylase was studied in the fluid taken from the drain in all patients with PFs, and it was found to be above the serum reference level. Fistula duration was longer than 10 days in all patients. Although the flow rate of PFs decreased, it continued to drain between 100-150 cc/day. Similar to the BFs, the PFs closed on the next day after drain removal without any leakage from the drainage area. Figure 3 shows the CT image taken one month after drain removal in a patient who developed PF after PD. No problems related to fistula were observed in any of the patients during the first-week, monthly, or yearly follow-up.
Discussion
A postoperative PF is the most important clinical complication after PD, with an incidence ranging from 9.9% to 28.5%. This complication causes a prolonged hospital stay and increased morbidity and mortality.4,5,6,7,8 In our cases with PFs, we continued to keep the drain in place postoperatively. If the drain placed during the operation did not function properly in patients with leakage, we used interventional radiological methods to place another catheter in the area. We did not consider the drain-tract-targeted approach in type B and C fistulas (as in our two patients) in the very early period, since this approach requires technical skills, and the rate of clinical response is around 60%, even in skilled hands.5,6,7,8,9
While holding the drain in place in PFs, we waited for the fistula tract to mature and performed fistulographies (Figure 1). After the tract fully matured, we promptly removed the drain without shortening it. We believe that once the tract has matured, the drain itself prevents the fistula from closing. The most common type of fistula was a PF, which developed after PH in 12 patients. In the follow-up of these patients, the drain was removed between the 20th and 30th postoperative days, and no problems were encountered in the following days.
BFs develop usually secondary to surgery. Endoscopic modalities, such as endoscopic sphincterotomy, stenting, and the insertion of nasobiliary drains have replaced surgery as the first-line approach in the management of minor bile duct injuries. Surgical reconstruction is recommended for major injuries.10,11,12 BFs were seen in 10 patients in our series. These patients had undergone surgery for various reasons and developed BFs during the follow-up period. Their fistulas closed after the drains were promptly removed on different days.
Concerning why the drain may prevent the fistula from closing, the inner surface of the fistula is covered with granulation tissue that the drain prevents from filling the lumen completely. Shortening or replacing the drain with a thin one does not allow for the fistula to close. When the drain is promptly removed, the wall covered with granulation collapses, and the passage is closed. If the drain is removed as described, there will be no stasis remaining, and neither sepsis nor leakage will occur because the tract is completely closed. Our study is the first in the literature to advocate that prolonged fistulas can be caused by drains, and that they can be closed with the prompt removal of the drains.
In the literature, some studies have indicated that in patients with biochemical leakage according to the last classification of the International Study Group of Pancreatic Fistula (grade A PF in the old classification), the drain can be removed early without causing any problems.10,13,14 In a study from Japan, Ito et al. reported that they were able to keep the drains in BFs for months after complex liver interventions, and injected ethanol into the tract to close the fistulas.15 However, in the current study, we showed that the same successful results can be achieved with the direct removal of the drain without the need for other methods, such as ethanol injection into the tract.
Limitations
Our study has certain limitations. We only had 20 patients, and all had PBFs. We are aware that there is no approach that can be applied to all fistulas; therefore, it is difficult to generalize our results. In addition, it should be kept in mind that our approach is appropriate in selected patients with persistent fistulas who do not have clear indications for surgical treatment.
As we showed in our limited number of patients, drains can be promptly removed in cases where there is no possibility of a problem when the fistula tract is closed.
Conclusion
Based on our knowledge and experience with a small number of patients over a long period, drains can prevent the closure of fistulas in some patients with PBFs, and the prompt removal of the drain in these cases can result in the closure of the fistula.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BF: Biliary fistula
ERCP: Endoscopic retrograde cholangiopancreatography
PBF: Pancreaticobiliary fistula
PD: Pancreaticoduodenectomy
PF: Pancreatic fistula
References
-
Evenson AR, Fischer JE. Current management of enterocutaneous fistula. J Gastrointest Surg. 2006;10(3):455-464. doi:10.1016/j.gassur.2005.08.001
-
Schecter WP. Management of enterocutaneous fistulas. Surg Clin North Am. 2011;91(3):481-491. doi:10.1016/j.suc.2011.02.004
-
Berry SM, Fischer JE. Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am. 1996;76(5):1009-1018. doi:10.1016/s0039-6109(05)70495-3
-
Søreide K, Labori KJ. Risk factors and preventive strategies for post-operative pancreatic fistula after pancreatic surgery: a comprehensive review. Scand J Gastroenterol. 2016;51(10):1147-1154. doi:10.3109/00365521.2016.1169317
-
Machado NO. Pancreatic fistula after pancreatectomy: definitions, risk factors, preventive measures, and management; review. Int J Surg Oncol. 2012;2012:602478.
-
Addeo P, Delpero JR, Paye F, et al. Pancreatic fistula after a pancreaticoduodenectomy for ductal adenocarcinoma and its association with morbidity: a multicentre study of the French Surgical Association. HPB (Oxford). 2014;16(1):46-55. doi:10.1111/hpb.12063
-
Roberts KJ, Hodson J, Mehrzad H, et al. A preoperative predictive score of pancreatic fistula following pancreatoduodenectomy. HPB (Oxford). 2014;16(7):620-628. doi:10.1111/hpb.12186
-
Søreide K, Healey AJ, Mole DJ, Parks RW. Pre-, peri-, and post-operative factors for the development of pancreatic fistula after pancreatic surgery. HPB (Oxford). 2019;21(12):1621-1631. doi:10.1016/j.hpb.2019.06.004
-
Hackert T, Werner J, Büchler MW. Postoperative pancreatic fistula. Surgeon. 2011;9(4):211-217. doi:10.1016/j.surge.2010.10.011
-
Sultan AM, Elnakeeb AM, Elshobary MM, et al. Management of post-cholecystectomy biliary fistula according to type of cholecystectomy. Endosc Int Open. 2015;3(1):E91-98.
-
Di Lascia A, Tartaglia N, Fersini A, Petruzzelli F, Ambrosi A. Endoscopy for treating minor post-cholecystectomy biliary fistula. Ann Ital Chir. 2018;89(3):270-277.
-
Krokidis M, Orgera G, Rossi M, Matteoli M, Hatzidakis A. Interventional radiology in the management of benign biliary stenoses, biliary leaks, and fistulas: a pictorial review. Insights Imaging. 2013;4(1):77-84. doi:10.1007/s13244-012-0200-1
-
Bassi C, Marchegiani G, Dervenis C, et al. The 2016 update of the International Study Group definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161(3):584-591. doi:10.1016/j.surg.2016.11.014
-
Pedrazzoli S, Brazzale AR. Systematic review and meta-analysis of surgical drain management after the diagnosis of postoperative pancreatic fistula after pancreaticoduodenectomy: draining-tract-targeted works better than standard management. Langenbecks Arch Surg. 2020;405(8):1219-1231. doi:10.1007/s00423-020-02005-8
-
Ito A, Ebata T, Yokoyama Y, et al. Ethanol ablation for refractory bile leakage after complex hepatectomy. Br J Surg. 2018;105(8):1036-1043. doi:10.1002/bjs.10801
Figures
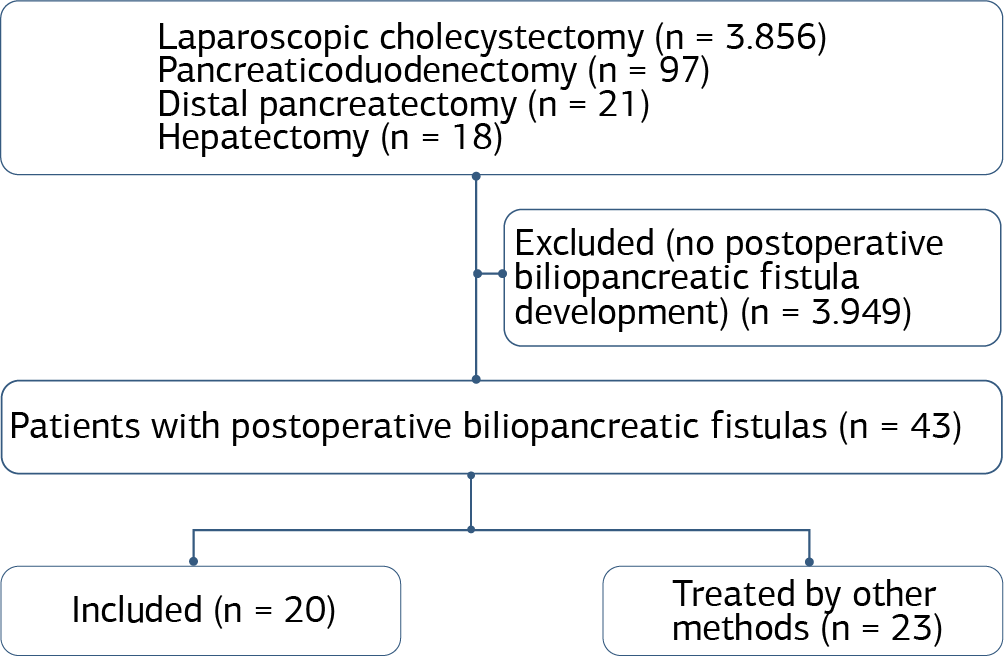
Figure 1. Flow diagram of the study

Figure 2. Fistulography image of a patient with bile leakage and stenting with endoscopic retrograde cholangiopancreatography

Figure 3. Computed tomography image taken one month after drain removal in a patient who developed pancreatic fistulas after pancreaticoduodenectomy
Tables
Table 1. Demographic and clinical characteristics of the patients
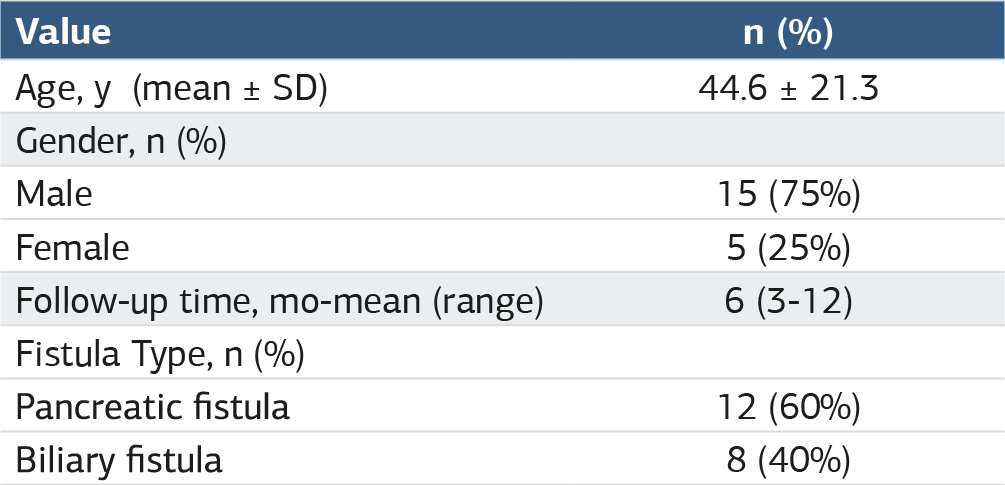
SD: standard deviation.
Table 2. Diagnosis of patients with fistulas and surgical procedures performed
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İsmail Hasırcı, Mehmet Eşref Ulutaş, Gürcan Şimşek, Ogün Erşen, Adil Kartal, Müslim Yurtçu, Selman Alkan, Kemal Arslan. An innovative approach: prompt withdrawal of the drain allows for fistula closure in some prolonged postoperative pancreaticobiliary fistulas. Ann Clin Anal Med 2025;16(5):320-324. doi:10.4328/ACAM.22185
- Received:
- March 20, 2024
- Accepted:
- October 3, 2024
- Published Online:
- December 2, 2024
- Printed:
- May 1, 2025