
Red cell distribution width to albumin ratio and neutrophil to lymphocyte ratio as prognostic markers in elderly emergency department patients
Red cell distribution width /albumin in geriatric patient
Authors
Abstract
AimThe aim of this study was to evaluate Red Cell Distribution Width/Albumin (RAR) and Neutrophil/Lymphocyte Ratio (NLR) in the follow-up and treatment processes of geriatric emergency department patients.
MethodsWe retrospectively collected demographic, complaint, comorbidity, vital signs, and laboratory test data of elderly patients who presented to our emergency department over a 6-month period. Next, we investigated the relationship of RAR and NLR with hospitalization, discharge, and mortality.
ResultsThis study included 1625 patients 606 (37.3%) were hospitalized, whereas 35 (2.2%) died. RAR was significantly different among the discharged, hospitalized, and dead patients (all p<0.001). NLR was a significant predictor of discharge (p<0.001) but not of hospitalization or mortality (p>0.05). In hospitalized patients, the areas under the receiver operating curves for RAR and NLR were 0.662 and 0.655, respectively, with the optimal cutoffs at 3.64 and 3.75, respectively (both p<0.001). Our univariate logistic regression analysis results indicated that RAR and NLR are effective predictors of both hospitalization and mortality (both p<0.001).
ConclusionRAR strongly predicts hospitalization, discharge, and mortality in elderly emergency department patients, whereas NLR appears to predict discharge alone.
Keywords
Introduction
Population aging—an issue in both developed and developing countries—has led to an increase in the prevalence of chronic health issues.1 Consequently, the need for and frequency of use of emergency services are increasing among elderly individuals. This situation is predicted to considerably affect emergency departments (EDs) over the next three decades. In Turkey, life expectancy is increasing every year; according to 2020 Turkish Statistical Institute data, the average life expectancy in Turkey was 78.6 years in 2017—comparable to the average life expectancy in 28 European countries (including Turkey; 80.9 years).[This information is available at: http: www.data.tuik.gov.tr] Moreover, the proportion of the population aged ≥65 years in Turkey is expected to increase from 8.5% in 2017 to 11% in 2025.[This information is available at: http: www.data.tuik.gov.tr] Similarly, in the United States, one in five individuals is expected to be aged >65 years by 2030 considerably.[This information is available at: https://www.census.gov/content/dam/Census/library/publications/2015/demo/p25-1143.pdf] Currently, 10%–15% of the ED population is composed of elderly individuals, who use EDs more than younger adults. Therefore, as the aging population increases, the number of ED visits is expected to increase considerably.[This information is available at: https://www.census.gov/content/dam/Census/library/publications/2015/demo/p25-1143.pdf]
Red cell distribution width (RDW) is a quantitative expression of anisocytosis, which is calculated as the standard deviation of red blood cell volume divided by mean red blood cell volume (MCV). RDW, a common hematologic parameter, is part of the standard complete blood count in hospitalized patients. Recent studies have demonstrated that, in patients with varied clinical conditions (e.g., cardiovascular disease, stroke, septic shock, and community-acquired pneumonia), a high RDW is associated with an increased mortality risk.2,3,4 RDW is a strong predictor of mortality in middle-aged and older adults; it is also recognized as an age-related prognostic biomarker in adults aged ≥45 years.5
Serum albumin is an acute-phase protein that is used as a nutritional marker. Because its levels decrease in an inflammatory state, serum albumin is considered a negative acute-phase protein. As such, in hospitalized elderly patients, serum albumin levels are inversely correlated with morbidity and mortality.6 Moreover, high albumin levels have been correlated with a short-term improvement in the functional status of hospitalized patients.7
The RDW-to-albumin ratio (RAR) is a newer biomarker that has been used to evaluate the prognoses of patients with stroke,8 heart failure,9 and acute myocardial infarction (MI).10 In this study, we evaluated the role of RAR and the neutrophil-to-lymphocyte ratio (NLR) in assessing the outcome of elderly patients in the ED in terms of hospitalization, discharge, and mortality.
Materials and Methods
Study PopulationThis was a single-center, retrospective, observational study. We included patients aged ≥65 years who presented to the ED of a tertiary education and research hospital over 6 months (July 1 to December 31, 2022). We included only patients with a complete blood count (CBC) and serum albumin data. However, we excluded patients who left the ED voluntarily, had no patient admission information, had hematologic malignancy, and presented with trauma.
Study ProtocolPatient age, sex, comorbidity, systolic and diastolic blood pressure, temperature, pulse rate, and fingertip oxygen saturation data were collected from the included patients’ medical records. We specifically included neutrophil and lymphocyte counts, RDW, and serum albumin data from their first ED laboratory test, before treatment was initiated. The patients were classified according to their ED outcomes: discharge, hospitalization, or mortality. ED results, mortality in the ED at follow-up, hospitalization, and discharge were recorded. We calculated NLR by dividing neutrophil count (×103 μL) by the lymphocyte count (×103 μL) and RAR by dividing RDW (%) by serum albumin level (g/dL). Sensitivity and specificity for hospitalized, discharged, and dead patients were calculated according to their cutoff RARs and NLRs. Demographic, complaint, comorbidity, vital signs, laboratory tests, and NLR and RAR data of the patients were statistically analyzed according to ED outcome groups.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Training and Research Hospital (Date: 26.04.2023, Decision No: E.23/1263).
Statistical AnalysisHere, continuous data are presented as means and standard deviations or medians and interquartile ranges (IQRs), whereas categorical data are presented as numbers and percentages. We used the Kolmogorov–Smirnov test to examine the conformity of the data to normal distribution. We applied Kruskal–Wallis analysis of variance to compare continuous data between discharged, hospitalized, and deceased ED patients, followed by the Kruskal–Wallis multiple comparison test to analyze the origin of between-group differences. The chi-square and Fisher exact tests were used for group comparisons of nominal variables through cross-tabulation. The diagnostic performance of RAR and NLR was evaluated based on the areas under the receiver operating characteristic (ROC) curves (AUCs), with the Youden index used to estimate the optimal cutoff points. The diagnostic accuracy of RAR and NLR values was evaluated using the following accuracy measures: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Risk factors for hospitalization and mortality were analyzed by univariate and multivariate logistic regression analyses. In the multivariate logistic regression analysis, variables considered risk factors were first included in the univariate logistic regression, and significant variables were then included in the multivariate analysis. The goodness of fit of the model was assessed using the Hosmer-Lemeshow goodness of fit. We used SPSS for Windows 20.0 (SPSS, Chicago, IL, USA) for all statistical analyses and considered p<0.05 to indicate statistical significance.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Over our 6-month study period, 1956 patients aged ≥65 years presented to the ED; all of them underwent testing for CBC and serum albumin. However, we excluded 299 patients because they had missing data and 32 patients because they had hematologic diseases or were receiving active chemotherapy treatment. Finally, 1625 patients were included in the final analysis; their mean age was 77.04 ± 7.90 years, and 54.9% of them were female. Hypertension (70.33%) was the most common comorbidity; furthermore, of all patients, 60.6% were discharged, 37.3% were hospitalized, and 2.2% died. The patients’ characteristics are presented in Table 1.
The median (IQR) RAR was 3.67 (0.14–33.26); it demonstrated significant differences between discharged, hospitalized, and dead patients (all p<0.001). In particular, RAR was higher than in discharged patients than in both hospitalized and deceased patients; additionally, it was higher in hospitalized patients than in dead patients. The median (IQR) NLR was 4 (0.1–176.0); moreover, it was lower in discharged patients [3.3 (2.1–6.07)] than in both hospitalized [5.6 (3.0–11.4)] and deceased [6.0 (1.8–11.2)] patients. The NLRs of hospitalized and dead patients demonstrated no significant differences (p>0.05; Table 2). For RAR, the AUC was 0.662 in hospitalized patients (p<0.001); furthermore, at a cutoff of 3.64, the PPV, NPV, sensitivity, and specificity were 49.2%, 73.1%, 64.8%, and 58.8%, respectively. It was 0.825 in deceased patients (p<0.001); additionally, at a cutoff of 4.01, the PPV, NPV, sensitivity, and specificity were 9.1%, 98.9%, 77.1%, and 72.6%, respectively (Figure 1). For NLR, the AUC was 0.655 in hospitalized patients (p<0.001); moreover, at a cutoff of 3.75, the PPV, NPV, sensitivity, and specificity were 49.3%, 74.1%, 67.7%, and 57.1%, respectively. It was 0.614 in deceased patients (p<0.05); at a cutoff of 5.05, the PPV, NPV, sensitivity, and specificity were 6.7%, 98.1%, 62.8%, and 68.7%, respectively (Figure 1).
Our univariate logistic regression analysis demonstrated that the hospitalization risk was elevated in ED patients with high serum albumin and lactate levels, RDW, RAR (>3.64), and NLR (>3.75; p<0.001). When the significant parameters in this univariate analysis were included in our multivariate analysis, an increase in lactate levels by 1 mmol/L led to an increase in hospitalization by 1.229 fold, whereas an NLR of >3.75 led to an increase in hospitalization by 1.782 fold (Table 3). Moreover,
another univariate logistic regression analysis indicated that serum lactate and albumin levels, RAR, and NLR were associated with an increased mortality risk (all p<0.001). When the significant parameters in this univariate analysis were included in our multivariate analysis, an increase in lactate levels by 1
mmol/L led to an increase in mortality by 1.445-fold (Table 3).
Discussion
In this study, RAR and NLR were both associated with increased all-cause hospitalization and death in elderly ED patients; in particular, RAR predicted mortality more effectively than NLR. In a study by Ayrancı et al. that included 784 elderly patients, the median patient age was 75 years, and the most common comorbidity was hypertension (54.5%); furthermore, the ED mortality and hospitalization rates were 0.8% and 49.8%, respectively.11 Our mortality (2.2%) and hospitalization (37.3%) rates were higher than those reported by Ayrancı et al. This may be due to the differences in the locations of the study hospitals and our patients’ inability to receive adequate care services due to difficulties in accessing social support.
Studies have demonstrated that a high RDW is associated with increased mortality in many clinical conditions. A high RDW may result from malnutrition and erythrocyte fragmentation.12 Specifically, a high RDW and impaired intravascular hemodynamics are associated with vascular pathologies.12 A recent study included a large group of elderly patients admitted to a hospital for identical reasons; the authors reported that patients with a high RDW at admission stay in the hospital 1.5–2 times longer than patients with a low RDW at admission.13 Alakare et al. also demonstrated that an increased RDW is associated with increased mortality in elderly patients.14 Similarly, our results indicated that patients with a high RDW have high hospitalization and mortality risks and that a high RDW predicts hospitalization.
A study on patients aged ≥72 years reported that serum albumin levels decrease with aging.15 In hospitalized elderly patients, serum albumin levels are inversely correlated with morbidity and mortality.16 Similarly, higher serum albumin levels were associated with a shorter recovery in functional status in hospitalized patients.7 These results are corroborated by our current findings: in discharged patients, serum albumin levels were higher than those in hospitalized and deceased patients. Several studies have demonstrated that NLR is a prognostic marker of acute coronary syndromes, cerebrovascular events, cancer, and acute infections.17,18,19,20 In the current study, NLR was significantly lower in the hospitalized and deceased patients than in the discharged patients, regardless of their diagnosis. In a study by Song et al. that included 2777 elderly patients, the AUC for NLR was 0.714 in dead patients.21
RAR is a novel biomarker previously used to diagnose acute MI, aortic aneurysm, pneumonia, diabetes, and cancer; it is also considered a prognostic indicator.8,9,10 To our knowledge, this is the first study evaluating the use of RAR to predict hospitalization, discharge, and mortality in elderly ED patients. We found that RAR differed between discharged, hospitalized, and deceased ED patients. Moreover, the RARs of the discharged patients were lower than those of both the hospitalized and deceased patients, whereas the RARs of the hospitalized patients were lower than those of the dead patients. Hong Wu et al. reported that in patients with acute MI, 90-day mortality was lower when the RAR was <4.32 (p<0.001).10 Another study reported that the RAR was associated with significant 28-day mortality in 234 patients with pneumonia in another univariate [odds ratio (OR) = 1.545, 95% confidence interval (CI) = 1.282–1.862, p<0.001] and multivariate (OR = 1.379, 95% CI = 1.103–1.723, p<0.005) logistic regression analyses.22 In a study on the role of RAR in predicting mortality in 1480 patients with stroke, a high RAR was significant (all p<0.001) in 30-day, 90-day, and 1-year mortality.8 Similarly, a population-based, prospective, cohort study investigating the prognostic role of RAR found that higher RAR was associated with an increased risk of death from any disease according to multivariate analysis.23 Among a total of 50.622 patients from the United States (aged ≥18 years) and 418.950 patients from the United Kingdom (aged ≥37 years), the mean RAR for the first group was 3.15 and for the second group was 2.99.23 The reason the mean RAR in that study were lower than in ours may be due to our patient group including an older population. The authors reported that the RAR was statistically significantly higher in predicting mortality for all causes of a total of 7,590 deaths in the first group and 36.973 deaths in the second group, regardless of age. The causes of mortality that RAR predicted with statistical significance were cancer, heart disease, cerebrovascular disease, respiratory disease, diabetes, and other causes.23
In the current study, NLR and RAR were better at predicting hospitalization and mortality, respectively. This may have been due to the inclusion of all hospitalized patients in one group, without stratifying hospitalized patients based on which department they were admitted (inpatient care or intensive care unit); additionally, the mortality rate among our patients was low. RAR is thus an accessible biomarker predicting hospitalization in elderly ED patients. However, this finding warrants a larger-scale prospective study.
Limitations
The main limitation of this study is its retrospective, singlecenter design. Studies predicting mortality after discharge and mortality during hospitalization in elderly patients are warranted.
Conclusion
The current results revealed that high RAR levels predict hospitalization and mortality in elderly ED patients. Therefore, RAR is a simple, accessible prognostic biomarker that could improve the management of elderly ED patients in the future.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
AUC: Area under the curve
CBC: Complete blood count
ED: Emergency department
NLR: Neutrophil-to-lymphocyte ratio
NPV: Negative predictive value
PPV: Positive predictive value
RAR: Red cell distribution width-to-albumin ratio
RDW: Red cell distribution width
ROC: Receiver operating characteristic
References
-
Laires PA, Perelman J. The current and projected burden of multimorbidity: a cross-sectional study in a Southern Europe population. Eur J Ageing. 2019;16(2):181-192. doi:10.1007/s10433-018-0485-0
-
Xanthopoulos A, Giamouzis G, Dimos A, et al. Red blood cell distribution width in heart failure: pathophysiology, prognostic role, controversies, and dilemmas. J Clin Med. 2022;11(7):1951. doi:10.3390/jcm11071951
-
Mohindra R, Mishra U, Mathew R, Negi NS. Red cell distribution width index as a predictor of severity of acute ischemic stroke: a correlation study. Adv J Emerg Med. 2020;4(2).
-
Wu H, Liao B, Cao T, Ji T, Huang J, Ma K. Diagnostic value of RDW for the prediction of mortality in adult sepsis patients: a systematic review and meta-analysis. Front Immunol. 2022;13:997853. doi:10.3389/fimmu.2022.997853
-
Patel KV, Ferrucci L, Ershler WB, Longo DL, Guralnik JM. Red blood cell distribution width and the risk of death in middle-aged and older adults. Arch Intern Med. 2009;169(5):515-523. doi:10.1001/archinternmed.2009.11
-
Tezze C, Sandri M, Tessari P. Anabolic resistance in the pathogenesis of sarcopenia in the elderly: role of nutrition and exercise in young and old people. Nutrients. 2023;15(18):4073. doi:10.3390/nu15184073
-
Turcato G, Zaboli A, Sibilio S, et al. Prognostic role of serum albumin in predicting 30-day mortality in patients with infections in emergency department: a prospective study. J Clin Med. 2023;12(10):3447. doi:10.3390/jcm12103447
-
Zhao N, Hu W, Wu Z, et al. The red blood cell distribution width-albumin ratio: a promising predictor of mortality in stroke patients. Int J Gen Med. 2021;14:3737-3747. doi:10.2147/ijgm.s322441
-
Ni Q, Wang X, Wang J, Chen P. The red blood cell distribution width-albumin ratio: a promising predictor of mortality in heart failure patients; a cohort study. Clin Chim Acta. 2022;527:38-46. doi:10.1016/j.cca.2021.12.027
-
Li H, Xu Y. Association between red blood cell distribution width-to-albumin ratio and prognosis of patients with acute myocardial infarction. BMC Cardiovasc Disord. 2023;23:66. doi:10.1186/s12872-023-03094-1
-
Ayrancı MK, Kücükceran K, Dundar ZD. NLR and CRP to albumin ratio as a predictor of in-hospital mortality in the geriatric ED patient. Am J Emerg Med. 2021;44:50-55. doi:10.1016/j.ajem.2021.01.053
-
Ananthaseshan S, Bojakowski K, Sacharczuk M, et al. Red blood cell distribution width is associated with increased interactions of blood cells with vascular wall. Sci Rep. 2022;12(1):13676. doi:10.1038/s41598-022-17847-z
-
Kim KM, Nerlekar R, Tranah GJ, Browner WS, Cummings SR. Higher red cell distribution width and poorer hospitalization-related outcomes in elderly patients. J Am Geriatr Soc. 2022;70(8):2354-2362. doi:10.1111/jgs.17819
-
Alakare J, Kemp K, Strandberg T, Castrén M, Tolonen J, Harjola VP. Red cell distribution width and mortality in older patients with frailty in the emergency department. BMC Emerg Med. 2023;23(1):24. doi:10.1186/s12873-023-00801-1
-
Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713-722. doi:10.1016/j.amjmed.2019.10.031
-
Akirov A, Masri-Iraqi H, Atamna A, Shimon I. Low albumin levels are associated with mortality risk in hospitalized patients. Am J Med. 2017;130(12):1465.e11-1465.e19. doi:10.1016/j.amjmed.2017.07.020
-
Ham SY, Yoon HJ, Nam SB, Yun BH, Eum D, Shin CS. Prognostic value of neutrophil/lymphocyte ratio and mean platelet volume/platelet ratio for 1-year mortality in critically ill patients. Sci Rep. 2020;10:21513. doi:10.1038/s41598-020-78476-y
-
Kim MS, Heo MY, Joo HJ, et al. Neutrophil-to-lymphocyte ratio as a predictor of short-term functional outcomes in acute ischemic stroke patients. Int J Environ Res Public Health. 2023;20(2):898. doi:10.3390/ijerph20020898
-
Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8-19. doi:10.4103/tjem.tjem_198_23
-
Dentali F, Nigro O, Squizzato A, et al. Impact of neutrophils to lymphocytes ratio on major clinical outcomes in patients with acute coronary syndromes: a systematic review and meta-analysis of the literature. Int J Cardiol. 2018;266:31-37. doi:10.1016/j.ijcard.2018.02.116
-
Song H, Kim HJ, Park KN, Kim SH, Oh SH, Youn CS. Neutrophil to lymphocyte ratio is associated with in-hospital mortality in older adults admitted to the emergency department. Am J Emerg Med. 2021;40:133-137. doi:10.1016/j.ajem.2020.01.044
-
Jeong JH, Heo M, Lee SJ, et al. Clinical usefulness of red cell distribution width/albumin ratio to discriminate 28-day mortality in critically ill patients with pneumonia receiving invasive mechanical ventilation, compared with lactate/albumin ratio: a retrospective cohort study. Diagnostics (Basel). 2021;11(12):2344. doi:10.3390/diagnostics11122344
-
Hao M, Jiang S, Tang J, et al. Ratio of red blood cell distribution width to albumin level and risk of mortality. JAMA Netw Open. 2024;7(5). doi:10.1001/jamanetworkopen.2024.13213
Figures

Figure 1. ROC analysis with RAR and NLR in hospitalized and dead patients
Tables
Table 1. General characteristics of the patients
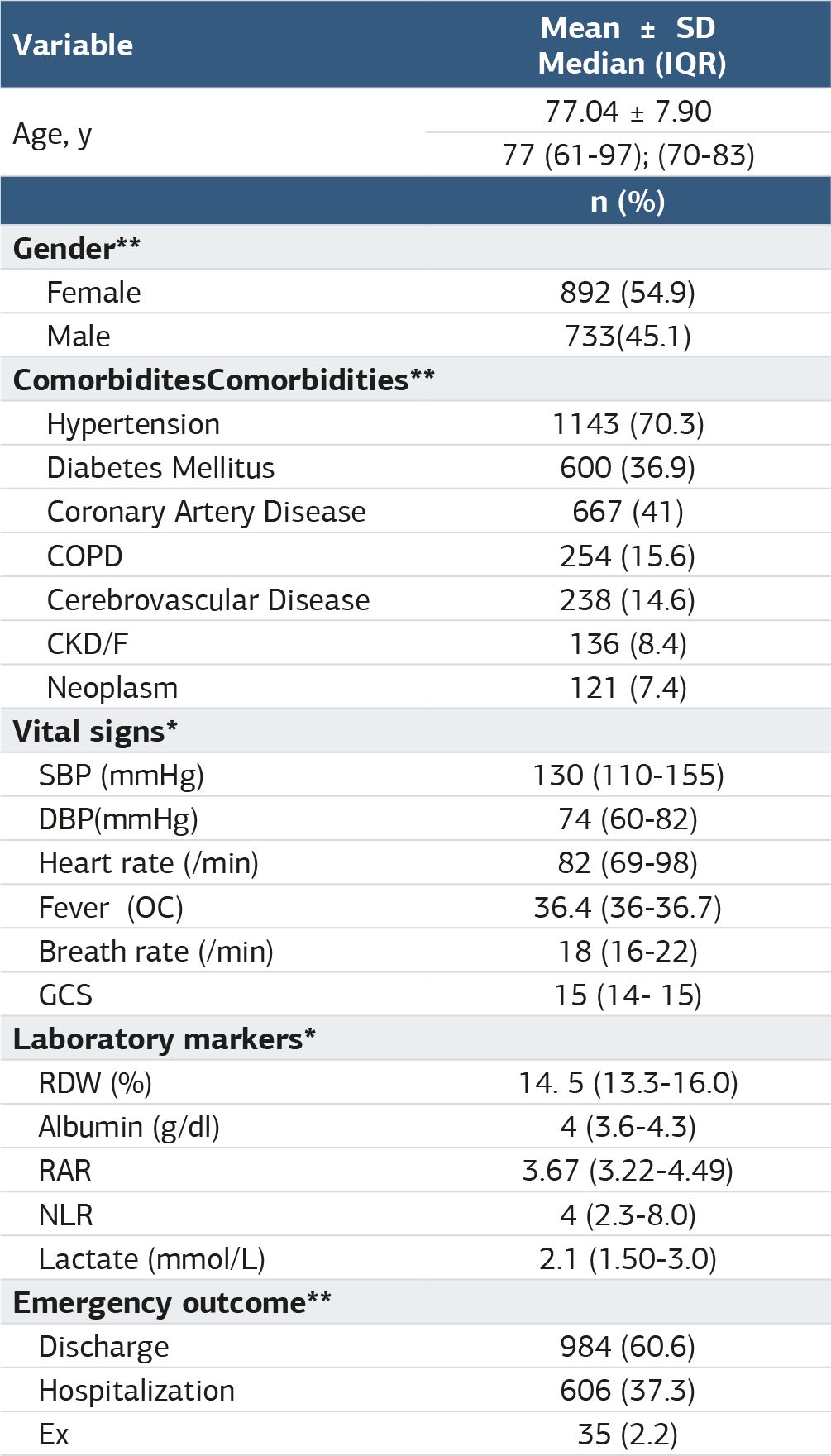
*Data are presented as median (25%–75%), **Data are presented as n (%) COPD, Chronıc obstructıve pulmonary dısease; CKD/, Chronic kidney disease, failure; SBP, Systolic blood pressure; DBP, Diastolic blood pressure; GCS, Glasgow coma scale; RDW, Red blood cell distribution width; RAR, Red blood cell distribution width albumin ratio; NLR, Neutrophil lymphocyte ratio.
Table 2. Comparison of age, gender, vital signs and laboratory findings of patients who were discharged, hospitalized and died in the emergency department

* Kruskal-wallis analysis of variance ** Ki kare test SBP, Systolic blood pressure; DBP, Diastolic blood pressure; GCS, Glasgow coma scale; RDW, Red blood cell distribution width; RAR, Red blood cell distribution width albumin ratio; NLR, Neutrophil lymphocyte ratio.
Table 3. Univariate and multivariate logistic regression analysis of risk factors for hospitalization and death

OR: Odds ratio CI: Confidence interval SBP, systolic blood pressure; DBP, Diastolic blood pressure; GCS, Glasgow coma scale; BR, Breath rate; RDW, Red blood cell distribution width; RAR, Red blood cell distribution width albumin ratio; NLR, Neutrophil lymphocyte ratio.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Dilber Üçöz Kocaşaban, Sertaç Güler, Esma Büşra Güzeş, Fatma Ceylan Çeçe, Erdal Demirtaş. Red cell distribution width to albumin ratio and neutrophil to lymphocyte ratio as prognostic markers in elderly emergency department patients. Ann Clin Anal Med 2025;16(5):325-330. doi:10.4328/ACAM.22283
- Received:
- May 25, 2024
- Accepted:
- September 24, 2024
- Published Online:
- December 9, 2024
- Printed:
- May 1, 2025