
Comparison of the effects of del nido cardioplegia and blood cardioplegiaon preoperative and postoperative albumin and TSH in cardiac surgeryperformed by cardiopulmonary bypass
Del nido cardioplegia and blood cardioplegia
Authors
Abstract
AimThe aim of this study was to compare the efficacy of Del Nido and blood cardioplegia in patients who underwent cardiac surgery with CPB support and required cardioplegia administration in the Department of Cardiovascular Surgery Clinic of our hospital by evaluating albumin and TSH hormones preoperatively and postoperatively.
MethodsIn this retrospective study, a total of 60 patients over the aged ≥18 years who underwent open heart surgery with CPB support between 2020 and 2024 were included. The patients were divided into two groups: 30 Del Nido cardioplegia group and 30 blood cardioplegia group. Preoperative and postoperative albumin and TSH values, cross-clamp and total bypass times, ejection fraction percentage (EF%), age and body surface area were analyzed and compared from the files of the patients in these groups.
ResultsAccording to statistical analysis of del nido and blood cardioplegia groups, age (54.31 ± 9.59, 61.79 ± 7.43) (p=0.001), cross-clamp duration (86.28 ± 22.75, 49.93 ± 14.29) (p=0.001), total duration (132.86 ± 29.53, 82.76 ± 16.93) (p=0.001) and preop-TSH (1.66 ± 1.3, 2.16 ± 1.2) (p=0.040) values were found to be statistically significant (p<0.05). However, Body surface area, ejection fraction, preop and postop-albumin and postop-TSH were not found to be statistically significant between the groups (p>0.05).
ConclusionAccording to our data, there was no significant difference in albumin and TSH parameters after CPB, indicating that the effects of Del Nido and blood cardioplegia were similar.
Keywords
Introduction
Cardiopulmonary bypass (CPB) is a mechanism that temporarily assumes the function of the heart and lungs. It mechanically oxygenates the blood in the extracorporeal circulation and circulates it throughout the body.1 Cardioplegic solutions are used to temporarily stop the heart to create a bloodless space and provide myocardial protection during surgery using the CPB technique. Dr. Melrose reported the first cardioplegia used in cardiopulmonary bypass (CPB) in the early 1950s. Dr. Melrose also demonstrated that high doses of potassium citrate temporarily stopped the heart so that it could restart.2 Potassium used in cardioplegic solutions depolarizes the myocardial membrane, triggering its contraction. As a result of this contraction, calcium ions are released, followed immediately by their retention. This causes the heart to stop in diastole.3 As the spread of the cardioplegia solution increases and its components are washed away along with the products of anaerobic cellular metabolism, electrical activity begins to manifest itself. Therefore, dosing of cardioplegia needs to be re-adjusted. However, there are other ions other than potassium used in cardioplegia. These are magnesium, sodium and calcium, etc. All of these ions reduce myocardial contraction. In this way they are effective in myocardial protection. In addition to these ions, it is also possible to provide further protection with some compounds such as bicarbonate and lidocaine.4 Various cardioplegic solutions are used to maintain the safety of CPB.5 These solutions include hypothermic cardioplegia, warm blood cardioplegia and Del Nido. Cardioplegic solutions can be administered anterograde or retrograde, or both, and must be of adequate volume.6 During administration, the rate, components, volume, pressure and temperature of the solution are adjusted by the perfusionis.7 In patients undergoing open heart surgery, changes in some electrolyte and protein levels may be observed due to CPB technique. Albumin, the most abundant protein in the blood 8 can be measured at low levels in the preoperative or postoperative period in open heart surgery using CPB technique. This is an important risk factor that increases preoperative and postoperative mortality and morbidity.9 Albumin has antithrombotic, antioxidant and antiinflammatory functions. It helps to transport certain substances and drugs and maintain the oncotic pressure of the blood. Results from studies show that it is a strong marker of cardiovascular (CV) risk. Protects against cardiovascular diseases (CVD) such as hypertension, congenital heart disease, atrial fibrillation and heart failure.10 The reference range for adult human serum albumin is accepted as 3.5-5 g/dl. However, the pathologic limit may vary according to the tests used. Serum albumin levels are slightly higher in men than in women. It tends to decrease with age.11 Another factor that increases the likelihood of CV morbidity and mortality is hyper- and hypothyroidism.12 Plasma thyroid-stimulating hormone (TSH or thyrotropin) level is a widely used marker to monitor thyroid status. According to the Turkish Society of Endocrinology and Metabolism (TEMD), the reference range for TSH is between 0.5-4 mU/L.13 TSH is <4.0 mIU/L in subclinical hyperthyroidism and TSH>0.4 mIU/L in subclinical hypothyroidism. However, free thyroxine and free triiodothyronine levels are within reference ranges.14
CV risks should be determined as a function of TSH. Only a few studies have looked at it from this perspective.15
The cardioplegies we use in our center to temporarily stop the heart to create a bloodless area and to provide myocardial protection are Del Nido and blood cardioplegia. Del Nido cardioplegia consists of; Patient blood (200 ml, 20% del Nido cardioplegia solution), Balanced electrolyte solution (1000 ml), Mannitol 20% (17 ml), MgSO₄ 15% (14 ml), KCI 1 mEq/ ml (26 ml), NaHCO₃ 8.4% (13 ml), Lidocaine 2% (6.5 ml).5 The cardioplegia content in KCI 1 mEq/ml and MgSO₄ 15% is calculated by completing the patient’s initial blood gas potassium value to 22 ml. Potassium and magnesium are used in a 1:1 ratio.
The aim of this study was to compare the efficacy of Del Nido and blood cardioplegia in patients who underwent cardiac surgery with CPB support and required cardioplegia administration in the Department of Cardiovascular Surgery Clinic of our hospital by evaluating albumin and TSH hormones preoperatively and postoperatively.
Materials and Methods
Working GroupsIn this retrospective study, a total of 60 patients aged ≥18 years who underwent open heart surgery with CPB support between 2021 and 2024 were included. The patients were divided into two groups: 30 Del Nido cardioplegia group and 30 blood cardioplegia group. Preoperative and postoperative albumin and TSH values, cross-clamp and total bypass times, ejection fraction percentage (EF%), age and body surface area were analyzed and compared from the files of the patients in these groups.
Inclusion and Exclusion CriteriaPatients over 18 years of age who underwent surgery with CPB support were included in the study. Patients under the age of 18 and patients who did not receive CPB support were excluded from the study.
Ethical ApprovalThis study was approved by Ethics Committee of the Harran University Clinical Research (Date: 22.07.2024, Decision No: 24/10/37).
Statistical AnalysisThe conformity of the data to normal distribution was tested with Kolmogorow-Smirnov and Shaphiro-Wilk tests. Independent samples t test was used for the comparison of numerical variables in two independent groups for those with normal distribution and Mann-Whitney U test was used for the comparison of numerical variables in more than two independent groups. One-way analysis of variance (ANOVA) and LSD multiple comparison tests were used for normally distributed characteristics and Kruskal Wallis test and All pairwise multiple comparison test were used for non-normally distributed characteristics. Mean±standard deviation for numerical variables and number and % values for categorical variables were given as descriptive statistics. SPSS Windows version 25.0 package program was used for statistical analysis and p<0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Table 1 shows the numbers and percentages of the Gender and Surgery Frequency Analysis. According to gender, a total of 60 patients were included in the study, 22 female (36.70%) and 38 male (63.30%). According to the surgery performed, 45 of the 60 surgeries were CABG (75.00%), 4 CABG+MVR (6.70%), 6 AVR (10.00%) and 5 MVR (8.30%) surgeries.
Table 2 shows the statistical analyses of the Del Nido and Blood cardioplegia groups. According to this analysis, mean age (54.31 ± 9.59; 61.79 ± 7.43) (p=0.001) and preoperative TSH (1.66 ± 1.3; 2.16 ± 1.2) (p=0.040) values were lower in the Del Nido group than in the Blood cardioplegia group. It was found to be statistically significant (p<0.05). Cross-clamp time (86.28 ± 22.75; 49.93 ± 14.29) (p=0.001) and total bypass time (132.86 ± 29.53; 82.76 ± 16.93) were longer in the Del Nido group (p=0.001). It was found to be statistically significant (p<0.05). Postoperative albumin values were slightly lower than preoperative albumin values in both groups. In addition, postoperative TSH values also showed a slight decrease compared to preoperative values in both groups. However, this was not statistically significant (p>0.05). In addition, body surface area and ejection fraction were not statistically significant between the groups (p>0.05).
Correlation analysis is given in Table 3. According to this analysis;
There is a low level negative significant correlation between age and Cross-clamp and Total bypass duration.
There is a low level negative significant correlation between Cross-Clamp and Age and Preoperative TSH.
There is a highly significant positive correlation between CrossClamp and Total bypass duration.
Discussion
Albumin has antithrombotic, antioxidant and anti-inflammatory functions. It is protective against CVD such as hypertension, congenital heart disease, atrial fibrillation and heart failure (HF).10 Albumin can be measured at low levels preoperatively or postoperatively in open heart surgery using CPB technique. This is an important risk factor that increases preoperative or postoperative mortality and morbidity.9
After 15 years of observation, a cohort study reported that hypoalbuminemia independently predicted both disease-related (such as CVD and cancer) and all-cause mortality.16 To determine the prognostic implications and phenotypic correlates of serum albumin, Prenner et al. conducted a study using magnetic resonance imaging. In this study, 118 adult patients with heart failure with preserved ejection fraction (HFpEF) had all-cause death and/or heart failure-related hospitalizations during 57.6 months of follow-up. The study reported that serum albumin was associated with detrimental pulsatile aortic hemodynamics, myocardial fibrosis and prognosis in HFpEF.17 Studies have reported that hypoalbuminemia is seen in approximately 25% of patients with HF. It has also been shown to be a serious predictor of negative results in HF with low EF.18 In a study of 2907 elderly individuals observed for 9.4 years, hypoalbuminemia was reported to be associated with the progression of HF onset with the actual preserved ejection fraction except for the risk factors of HF.19 In a study describing the adverse consequences of low albumin and CVDs in patients with coronary artery disease, it was reported that patients with hypoalbuminemia were at risk for major CVDs and had a 1.5-year increase in all-cause mortality.20 In our retrospective study, the preop-albumin value was slightly lower in the Del Nido group compared to the blood cardioplegia group. However, it was not found to be statistically significant. Postop-albumin values after CPB were slightly higher in the Del Nido group. However, there was no significant difference in both groups. Preop and postop albumin values were close to each other in both Del Nido and blood cardioplegia groups. It was observed to be within the range of normal reference values. Another factor that increases the likelihood of CV morbidity and mortality is hyper- and hypothyroidism.12 Changes in thyroid function cause changes in blood pressure and CV risk factors. Late clinical recognition of subclinical structures of thyroid dysfunction (subclinical hypo- and hyperthyroidism) leads to negative CV outcomes.21 It has been reported to increase CV risk. The association between atrial fibrillation and hyperthyroidism has been shown as an example.22 In a cohort study involving euthyroid individuals, high-normal TSH levels were compared with moderate-normal TSH levels. Highnormal TSH levels have been linked to increased CVD mortality rates associated with all causes.23 In contrast, other studies have not found an association between TSH levels in the normal range and mortality in the general population. A cohort study of 212,456 individuals with a follow-up of 4.3 years reported that plasma TSH levels in the normal reference range were not associated with mortality.24
Limitations
The fact that the study was conducted in a single center and with a small number of patients.
Conclusion
In our study, preoperative TSH values of patients in the Del Nido and blood cardioplegia groups before CPB were found to be statistically significant. Preoperative albumin levels were not found to be significant. However, no significant difference was observed in postoperative albumin and TSH values after CPB in both Del Nido and blood cardioplegia groups. Although these values showed a slight decrease after CPB compared to the preoperative values, they were not found to be statistically significant. This suggests that the effects of Del Nido and blood cardioplegia on these parameters were similar.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ANOVA: analysis of variance
AVR: aortic valve replacement
CABG: coronary artery bypass grafting
CPB: cardiopulmonary bypass
CV: cardiovascular
CVD: cardiovascular disease
EF: ejection fraction
HF: heart failure
HFpEF: heart failure with preserved ejection fraction
LSD: least significant difference
MVR: mitral valve replacement
TSH: thyroid stimulating hormone
References
-
Padak M, Dikme R. Kardiyopulmoner baypasta gelişebilen böbrek hasarında miRNA’ların biyobelirteç olma rolü [The role of miRNAs as a biomarker in kidney damage developing in cardiopulmonary bypass]. J Nephrol Nurs. 2022;17(1):21-28. doi:10.47565/ndthdt.2022.50
-
Ali JM, Miles LF, Abu-Omar Y, et al. Global cardioplegia practices: results from the Global Cardiopulmonary Bypass Survey. J Extra Corpor Technol. 2018;50(2):83-93. doi:10.1051/ject/201850083
-
Chambers DJ, Fallouh HB. Cardioplegia and cardiac surgery: pharmacological arrest and cardioprotection during global ischemia and reperfusion. Pharmacol Ther. 2010;127(1):41-52. doi:10.1016/j.pharmthera.2010.04.001
-
Matte GS, del Nido PJ. History and use of del Nido cardioplegia solution at Boston Children’s Hospital. J Extra Corpor Technol. 2012;44(3):98-103. doi:10.1051/ject/201244098
-
Amaç B, Selçuk M, Bölükbaş S, et al. Use of del Nido cardioplegia in adult cardiac surgery. Eur Res J. 2022;8(1):139-144. doi:10.18621/eurj.970465
-
Lopes JB, Santos CCMD. Coronary perfusion pressure during antegrade cardioplegia in on-pump CABG patients. Braz J Cardiovasc Surg. 2017;32(3):171-176. doi:10.21470/1678-9741-2017-0035
-
Baker RA, Bronson SL, Dickinson TA, et al. Report from AmSECT’s International Consortium for Evidence-Based Perfusion: American Society of Extracorporeal Technology standards and guidelines for perfusion practice: 2013. J Extra Corpor Technol. 2013;45(3):156-166. doi:10.1051/ject/201345156
-
Rabbani G, Ahn SN. Structure, enzymatic activities, glycation and therapeutic potential of human serum albumin: a natural cargo. Int J Biol Macromol. 2019;123:979-990. doi:10.1016/j.ijbiomac.2018.11.053
-
Bağış MZ. Açık kalp cerrahisinde preoperatif albümin değerinin renal fonksiyonlar üzerine etkisi [Effect of preoperative albumin levels on renal functions in open heart surgery]. EAHSJ. 2023;1(1):29-34
-
Manolis AA, Manolis TA, Melita H, et al. Low serum albumin: a neglected predictor in patients with cardiovascular disease. Eur J Intern Med. 2022;102:24-39. doi:10.1016/j.ejim.2022.05.004
-
Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52(1):8-12. doi:10.1016/j.ejim.2018.04.014
-
Corona G, Croce L, Sparano C, et al. Thyroid and heart, a clinically relevant relationship. J Endocrinol Invest. 2021;44(12):2535-2544. doi:10.1007/s40618-021-01590-9
-
Türkiye Endokrinoloji ve Metabolizma Derneği. Tiroid hastalıkları tanı ve tedavi kılavuzu. Subklinik hipotiroidi [Diagnosis and treatment guide for thyroid diseases: subclinical hypothyroidism]. Ankara: Tuna Matbaacılık; 2013:13-15
-
Biondi B, Cooper DS. Subclinical hyperthyroidism. N Engl J Med. 2018;378(25):2411-2419. doi:10.1056/nejmcp1709318
-
Dalila N, Frikke-Schmidt R, Nordestgaard BG, Tybjærg-Hansen A. Plasma TSH and cardiovascular disease in the general population: a Mendelian randomization study of 105,224 individuals. Atherosclerosis. 2023;376(1):26-33. doi:10.1016/j.atherosclerosis.2023.05.018
-
Umeki Y, Adachi H, Enomoto M, et al. Serum albumin and cerebro-cardiovascular mortality during a 15-year study in a community-based cohort in Tanushimaru, a cohort of the seven countries study. Intern Med. 2016;55(20):2917-2925. doi:10.2169/internalmedicine.55.6931
-
Prenner SB, Pillutla R, Yenigalla S, et al. Serum albumin is a marker of myocardial fibrosis, adverse pulsatile aortic hemodynamics, and prognosis in heart failure with preserved ejection fraction. J Am Heart Assoc. 2020;9(3):e014716. doi:10.1161/jaha.119.014716
-
Horwich TB, Kalantar-Zadeh K, MacLellan RW, Fonarow GC. Albumin levels predict survival in patients with systolic heart failure. Am Heart J. 2008;155(5):883-889. doi:10.1016/j.ahj.2007.11.043
-
Gopal DM, Kalogeropoulos AP, Georgiopoulou VV, et al. Serum albumin concentration and heart failure risk: the health, aging, and body composition study. Am Heart J. 2010;160(2):279-285. doi:10.1016/j.ahj.2010.05.022
-
Chien SC, Chen CY, Leu HB, et al. Association of low serum albumin concentration and adverse cardiovascular events in stable coronary heart disease. Int J Cardiol. 2017;241:1-5. doi:10.1016/j.ijcard.2017.04.003
-
Berta E, Lengyel I, Halmi S, et al. Hypertension in thyroid disorders. Front Endocrinol (Lausanne). 2019;10:482. doi:10.3389/fendo.2019.00482
-
Neves JS, Fontes-Carvalho R, Borges-Canha M, et al. Thyroid hormones within the normal range and cardiac function in the general population: the EPIPorto Study. Eur Thyroid J. 2021;10(2):150-160. doi:10.1159/000508407
-
Inoue K, Tsujimoto T, Saito J, Sugiyama T. Association between serum thyrotropin levels and mortality among euthyroid adults in the United States. Thyroid. 2016;26(10):1457-1465. doi:10.1089/thy.2016.0156
-
Zhang Y, Chang Y, Ryu S, et al. Thyroid hormones and mortality risk in euthyroid individuals: the Kangbuk Samsung Health Study. J Clin Endocrinol Metab. 2014;99(7):2467-2476. doi:10.1210/jc.2013-3832
Tables
Table 1. Gender and surgery frequency analysis
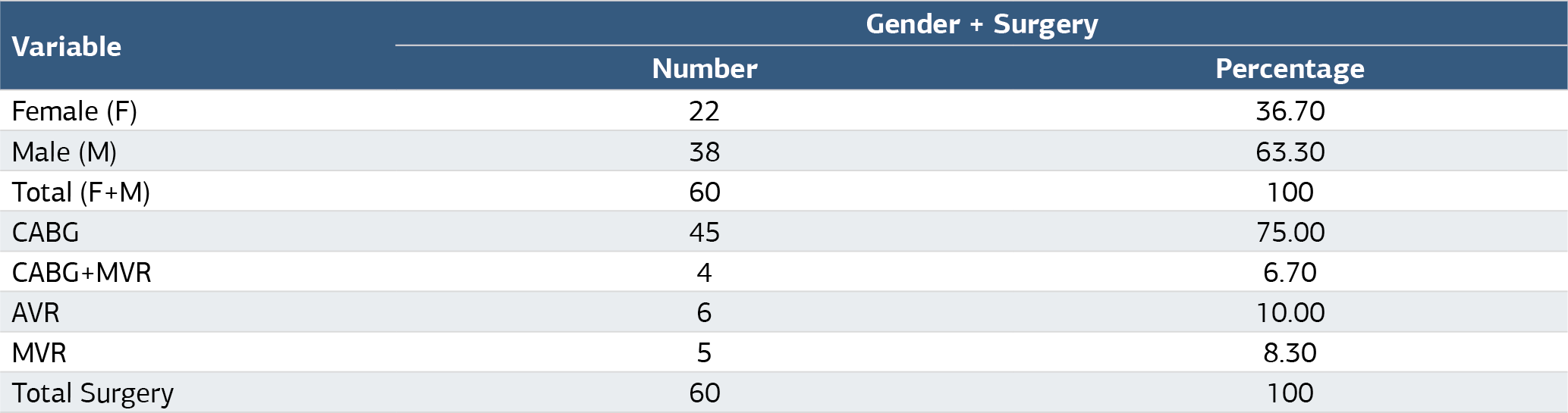
AVR: Aortic valve replacement, CABG: Coronary artery bypass graft, MVR: Mitral valve replacement
Table 2. Statistical analysis of groups

a. Mann-whitney U test * p<0.05, **p<0.001, Del nido cardioplegia (n=30), Blood cardioplegia (n=30). BSA: Body surface area, EF: Ejection fraction, kg: Kilogram, m: Meter, min: Minute, TSH: Thyroid-stimulating hormone
Table 3. Correlation analysis

Spearman’s correlation test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yasemin Hacanlı, Murat Ziya Bağış. Comparison of the effects of del nido cardioplegia and blood cardioplegiaon preoperative and postoperative albumin and TSH in cardiac surgeryperformed by cardiopulmonary bypass. Ann Clin Anal Med 2025;16(1):57-61. doi:10.4328/ACAM.22348
- Received:
- July 31, 2024
- Accepted:
- September 2, 2026
- Published Online:
- October 29, 2024
- Printed:
- January 1, 2025