
Multi-centric comparative analysis of the clinical and functional outcomes of two neuromuscular island flaps for fingertip defects: Hetero-digitalversus reverse homo-digital
Hetero- versus reverse homo-digital
Authors
Abstract
AimThe goal of fingertip injury reconstructions should be mainly to restore the sensation of the tip with similar pulp volume, texture, and tissue preserving the contour. Regarding this aim, many flap techniques have been defined in the literature. Herein this manuscript, aimed to present and compare clinical outcomes of two different local flap procedures, hetero-digital artery island flap, reverse homo-digital artery island flap, widely used for the reconstruction of fingertip defects.
MethodsA 8-year prospectively followed-up, retrospectively statistical analyzed 83 patients undergoing reconstruction of fingertip defects of 2-5 digits by hetero-digital artery island flap (Group 1, n =56), reverse homo-digital artery island flap (Group 2, n =52) was performed. All participants were assessed using the Quick Disability of Arm, Shoulder, and Hand (Q-DASH) score, the cold intolerance symptom severity score (CISS), static 2-point discrimination, the time taken to return to work, and the range of motion (ROM) values for each operated finger joint.
ResultsThe mean age of patients was 36.9 years with a male-to-female ratio of 2.6:1 and a mean follow-up of 26.72 months. There were no significant differences in average scores for Q-DASH, CISS, static 2-point discrimination, time to return to work, and DIP ROM between the study groups. However, the average ROM values for the PIP and MCP joints were significantly lower in Group 2 compared to Group 1.
ConclusionThe use of hetero-digital artery island flap for fingertip reconstruction is a reliable one-stage option in terms of improved ROM of finger joints. However, the surgical experience is of most importance to reduce postoperative morbidity of the procedure. Homo-digital artery island flap can be seen as another attractive option for less experienced surgeons with excellent postoperative results regarding DASH and CISS scores, static 2-point discrimination and time to return to work.
Keywords
Introduction
The primary objective of fingertip injuries reconstructions should be to reestablish the sensation of the tip by maintaining the form and ensuring equal pulp quantity, texture, and tissue. The literature has described numerous flap strategies that align with this objective.1 Each technique presented and applied in a therapeutic setting carries its own set of benefits and drawbacks.2 The two most frequently employed strategies are homo-digital and reverse hetero-digital neuro-vascular island flaps. Each of these two strategies possesses unique qualities. In the case of, the crushing injuries potentially harm the pedicle vessels, and the soft-tissue defect’s shape or subsequent lacerations on the wounded finger limit the flap’s use, homo-digital neuro-vascular island flaps may not be suitable.3 In such situations, it may be advisable to consider a hetero-digital island flap. This procedure offers substantial coverage of soft tissue from a distant place with a reliable blood supply. Additionally, it can restore sensation in a single operation without compromising the sensitivity of the donor finger. On the other hand, reverse hetero-digital neuro-vascular island flaps might keep digits immobile in positions that are not natural.4 This can limit joint range of motion and cause stiffness and contractures in both the donor and recipient fingers, as well as pain at the donor finger sites.
This study commences by examining which type of flap application yields the most beneficial outcomes for fingertip injuries. This study’s goal is to compare the two most common procedures in terms of how well they work and how long the flap lasts. The outcomes that will be looked at are static 2-point discrimination, cold intolerance, time to return to work, length of follow-up, defect size, and joint range of motion (ROM).
Materials and Methods
The local ethics committee, with the reference number 2023-4258, granted ethics approval. In five tertiary-level hand trauma centers from December 2014 to March 2023, a retrospective statistical review of prospective follow-up data was conducted on 108 patients who underwent reconstruction of the fingertip defects of the second to fourth digits using a hetero-digital neuro-vascular island flap (Group 1, n =56) and a reverse homo-digital neuro-vascular island flap (Group 2, n =52). The study was omitted from thirteen patients due to the absence of data. Before participating in the study, all patients gave their informed consent, meaning they understood the risks and benefits of taking part. The research was also carried out according to the ethical guidelines set out in the Declaration of Helsinki.
The PNB classification system was employed to evaluate all cases in terms of age, gender, etiology of trauma, duration of follow-up, and the severity of the injury.5 And also, postoperative Quick Disability of Arm, Shoulder, and Hand Score (Q-DASH),6 post-operative cold intolerance symptom severity score (CISS),7 post-operative static 2-point discrimination test, ROM value of phalangeal joints and time to return to work were performed.
Reconstruction of the fingertip defect was initiated with local radical debridement and lavage following routine upper extremity preparation and draping. Surgical planning was initiated with a digital Allen’s test and Doppler examination to verify the functionality of the digital arteries of both the donor and recipient digits. A tie-over dressing is employed in all cases to conceal the donor site defect with full-thickness skin obtained from the severed portion or from an alternative appropriate location, if available. All patients were administered antibiotics and analgesics within 24 hours of surgery. All patients were discharged within 24 hours of surgery in this investigation. Following the surgery, 100 mg of acetylsalicylic acid was administered and maintained for a period of one week. In addition to the postoperative restoration of motion, patients must collaborate with a hand therapist to undergo sensory reeducation of the affected digit
Surgical TechniquesHetero-Digital Neuro-Vascular Island Flap Operative ProcedureThe radial side of the digit is chosen in all cases as in the representative case presented in Figure 1 since its removal will have minimal influence on grip and pinch activities. The measurements of the flap needed are marked on the ulnar pulp of the chosen donor finger with roughly 2 to 4 mm broader (Figure 1a). The flap frequently necessitates skin harvesting from the donor finger’s distal and middle phalanges. The flap is incised, and a mid-lateral incision is created starting at the flap’s proximal end. The flap is lifted from the distal to the proximal end, and the complete neuro-vascular bundle is elevated in tandem (Figure 1b). Because the vasa vasorum of the artery is the only source of venous outflow for the flap, it is crucial to raise the neuro-vascular bundle with a reasonably thick cuff of surrounding fatty tissue encompassing the vasa vasorum of the artery. Failure to do this will result in flap congestion. To provide appropriate transposition to the recipient digit, one must dissect quite close to the palm, and the other branch of the common digital artery must be separated. To provide proper flap motion, the common digital nerve might be divided along the fascicles. A subcutaneous tunnel can then be used to transfer the flap to the index and the flap is subsequently inserted into the index finger’s recipient defect (Figure 1c-d).
Reverse Homo-Digital Neuro-Vascular Island Flap Operative ProcedureAfter determining the defect’s size and shape, a flap is designed and marked along the mid-lateral axis of the proximal phalanx of the same finger showing the defect (Figure 2a). The junction of the dorsal and volar skin in the lateral aspect of the digit forms a line in which a lazy- S skin incision is continued distally after the division of the proximal end of the digital artery which is the enthesis region of the flexor digitorum profundus. The flap is raised in a proximal to distal direction after identification of neuro-vascular bundle with attention not to use the dominant digital artery. The vascular pedicle should be dissected to the level where the flap may easily reach the defect, with a thin cuff of tissue left surrounding that as well (Figure 2b). To preserve a good cuff of subcutaneous tissues around the vascular pedicle to allow adequate venous drainage, it has to be secure. With the division of the lateral digital sheet, the dissection proceeds in a distal to proximal orientation, releasing the digital artery and nerve up to the proximal interphalangeal joint level. Nerve dissection should never be performed more than 3-5mm from the distal interphalangeal joint. After dissection and elevation, the flap is inset into the defect, which can be advanced or rotated 180o to cover the fingertip defect (Figure 2c).
Ethical ApprovalThis study was approved by the Ethics Committee of Necmettin Erbakan University (Date: 17.03.2023, Decision No: 2023/4248).
Statistical AnalysisThe PASW version 17.0 software (SPSS Inc., Chicago, IL, USA) was employed to analyze the statistics. In order to verify the Gaussian distribution of the continuous variables, Kolmogorov– Smirnov tests were implemented. All continuous variables with a Gaussian distribution were subjected to T-tests. The study used a significance level of p < 0.05 for all statistical comparisons. This means that any result with a p-value less than 0.05 was considered statistically significant. Different statistical tests were used depending on the type of comparison: The concordance and disparities between intra- and interobserver measurements of various scoring systems, including Q-DASH, CISS, static 2-point discrimination, and phalangeal joints’ ROM values, were evaluated in the outcomes of all patients using a two-way mixed-effects model. These measurements were assessed using Interclass Coefficients (ICC). It was determined that the intra- and inter-observer measurements were highly reliable (ICC: 0.935–0.986), –good (ICC: 0.879–0.981), excellent (ICC: 0.911–0.686) –outstanding (ICC: 0.927–0.906), excellent (ICC: 0.955–0.946) –good (ICC: 0.843–0.921), and excellent (ICC: 0.955–0.921) –good (ICC: 0.899–0.831), respectively.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The average follow-up period was 26.72 ± 2.7 months, and the mean age of all patients was 27.4 ± 5.1 years. Work-related injuries (n = 61) were the most prevalent cause, followed by home-related injuries (n = 25), motor vehicle-related injuries (n = 17), and others (n = 5). The most prevalent presentations were PNB 400 (palmar oblique loss, no nail injury, and no bone injury) in 71 cases, PNB 521 in 19, and PNB 665 in 18 cases, according to the PNB classification system.5 Two patients in Group 2 experienced complete flap loss as a result of potential iatrogenic pedicle laceration during dissection. Despite the fact that 35 cases (32.4%) were observed to have transient venous congestion, only four patients experienced partial flap loss, which was treated conventionally (Table 1). The mean of the Q-DASH score, CISS score, static 2-point discrimination, duration to return to work, and ROM value of the DIP joint did not differ significantly between the groups (p<0.05) (Table 2). While the average ROM in the PIP and MCP joints was considerably lower in Group 2 compared to Group 1, this difference was not statistically significant (p>0.05).
Similarly, although Group 2 had lower ROM values than Group 1, this difference was also not statistically significant (p>0.05). In comparison to the homo-digital neuro-vascular island flap, the hetero-digital neuro-vascular island flap has a statistically significant detrimental effect on the ROM of the donor digit’s DIP, IP, and MCP joints (p<0.05) (Table 3).
Discussion
The reconstructive strategy for fingertip injuries is determined by the surgeon’s expertise and skills. Naturally, every proficient surgeon chooses their reconstructive approach based on multiple surgical indications and patient-specific considerations. The patient’s sociodemographic, injury type, and severity characteristics are altered by these factors. This research assessed and compared the clinical outcomes of the three most often employed surgical techniques for fingertip injuries. The findings of this study will have a favorable impact on the decision-making process of surgeons.
The vitality of a flap is the paramount result of these two reconstruction procedures, and it varies across different investigations. Roberto et al. found that all neuro-vascular island flaps with different fingers survived in a study of 22 patients.8 Wang et al. recently reported a 100% survival rate for all hetero-digital neuro-vascular island flaps, used in 14 patients.9 Regmi et al. conducted a study on the results of 8 clinical trials including the use of the reverse homo-digital neuro-vascular island flaps technique. They found that the average survival rate was 98%.10 The flap survival rate in our patients was 98.2% for hetero-digital neuro-vascular island flaps and 96.1% for reverse homo-digital neuro-vascular island flaps.
Temporary venous congestion can be identified in nearly all procedures utilized for fingertip injury restorations, occurring at different frequencies. Venous congestion may occur in the early postoperative period, particularly within the first 24 hours, with reverse homo-digital neuro-vascular island flaps. This is likely caused by the rotation of the flap during the insertion of the fingertip defect. In hetero-digital neuro-vascular flaps, venous congestion occurs due to extensive dissection of the pedicle, rather than the inclusion of fatty tissue cuff on the pedicle that contains venae comitantes for proper venous drainage. In our research, postoperative venous congestion was clinically determined in 14 patients of hetero-, and 16 patients of homodigital neuro-vascular island flaps.
Postoperative neuropathic pain is more prevalent in patients who had a reverse homo-digital neuro-vascular island flap compared to those who received a hetero-digital neuro-vascular island flap. This was seen in a study involving 18 patients. The most significant adverse consequence of the reverse homodigital neuro-vascular island flap is likely due to compression of the digital nerve following the rotation of the flap to repair the fingertip defect. Kim SK proposed in his article which should keep in mind that retaining a tiny amount of adipose tissue beneath the donor site on the fingertip could potentially reduce neuropathic discomfort associated with this condition.11
Another important result of fingertip injury healing is the improvement of static 2-point discrimination. Based on the statistical analysis conducted on patients, there is no significant difference observed in 2-point discrimination. However, upon comparing the individual results in each group to the existing literature, it was discovered that they were all comparable.12,13,14
The precise etiology of cold intolerance remains unclear, but alterations in brain and/or vascular pathways have been implicated. The CISS scale spans from zero to one hundred points. The diagnosis of cold intolerance is determined using a cut-off value of 30 points,7 based on the 95 percent confidence interval in a healthy population. Our study found no significant statistical difference between the groups in terms of the CISS. However, patients who underwent hetero-digital neuro-vascular island flap surgery reported fewer complaints, potentially due to the characteristics of the flap. Regarding another aspect, Karjalainen and Jokihaara made the decision not to combine the data on cold intolerance in their review and meta-analysis due to the presence of heterogeneously dispersed data.15
Due to the fact that stiffness in the hand joints is the most uncertain outcome, it is recommended that thorough postoperative physical therapy be conducted following fingertip damage reconstructions. In this particular study, it was determined that the decreased range of motion (ROM) values of the PIP and MCP joints for Group 1 compared to Group 2 were associated with a longer period of immobilization of these joints as a result of donor site morbidity. It was believed that the flap elevation from a donor site close to the MCP joint, which may restrict the range of motion for MCP and PIP joints, was the cause of the decreased range of motion (ROM) values of PIP and MCP joints for Group 1 compared to Group 2, despite the fact that there was no significant difference between the two groups.
Limitations
The primary limitations of this research were the inability to standardize etiological components and the study’s retrospective and uncontrolled nature. Another constraint of the study is the lack of randomization in the selection of cases, as the surgeon applied his favorite procedure to his preferred patient without any random assignment.
Conclusion
In conclusion, the choice between homo-digital and heterodigital island flaps for fingertip reconstruction should be based on the specific characteristics of the injury and the desired outcomes. By comparing the clinical effects and long-term results of these techniques, healthcare providers can make informed decisions to optimize patient outcomes in fingertip reconstruction procedures.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants before enrollment in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CISS: Cold intolerance symptom severity score
DIP: Distal interphalangeal
ICC: Intraclass coefficient
MCP: Metacarpophalangeal
PIP: Proximal interphalangeal
PNB: Pulp, nail, bone
Q-DASH: Quick disability of the arm, shoulder, and hand
ROM: Range of motion
References
-
Kuwahara Y, Hara T, Kurahashi T, Kitami T, Tatebe M. Comparing clinical and aesthetic outcomes of cross-finger and homodigital reverse digital artery island flap for fingertip injuries: a single-center retrospective cohort study. J Plast Reconstr Aesthet Surg. 2024;95:411-418. doi:10.1016/j.bjps.2024.03.019
-
Chen K, Yang S, Cheng Y, Xiang W, Zhang J, Shen J, et al. Reverse homodigital artery versus reverse dorsal homodigital island flaps for fingertip defect repair: a meta-analysis. J Plast Reconstr Aesthet Surg. 2023;82:237-246. doi:10.1016/j.bjps.2023.04.015
-
Wang S, Yuan C, Ding W, Shen H, Gu J. Repair of finger pulp defect and sensory reconstruction using reverse homodigital artery island flap with palmar cutaneous branches of the proper digital nerve. Ann Plast Surg. 2023;90(6):559-563. doi:10.1097/sap.0000000000003591
-
Rinkoff S, Ruston J, Nikkhah D. Digital artery flaps: homodigital and heterodigital island flaps. In: Nikkhah D, Rawlins J, Pafitanis G, eds. Core Techniques in Flap Reconstructive Microsurgery: A Stepwise Guide. 2023:259-269. doi:10.1007/978-3-031-07678-7_27
-
Evans DM, Bernardis C. A new classification for fingertip injuries. J Hand Surg Br. 2000;25(1):58-60. doi:10.1054/jhsb.1999.0305
-
Koldas Dogan S, Ay S, Evcik D, Baser O. Adaptation of Turkish version of the Questionnaire Quick Disability of the Arm, Shoulder, and Hand in patients with carpal tunnel syndrome. Clin Rheumatol. 2011;30(2):185-191. doi:10.1007/s10067-010-1470-y
-
Töre NG, Gömüşsoy M, Oskay D. Validity and reliability of the Turkish version of the Cold Intolerance Symptom Severity Questionnaire. Turk J Med Sci. 2019;49(4):1221-1227.
-
Adani R, Marcoccio I, Tarallo L, Fregni U. The reverse heterodigital neurovascular island flap for digital pulp reconstruction. Tech Hand Up Extrem Surg. 2005;9(2):91-95. doi:10.1097/01.bth.0000158973.08273.1f
-
Wang H, Yang X, Chen C, Huo Y, Wang B, Wang W. Modified heterodigital neurovascular island flap for sensory reconstruction of pulp or volar soft tissue defect of digits. J Hand Surg Am. 2020;45(1):67-67. doi:10.1016/j.jhsa.2019.04.014
-
Regmi S, Gu JX, Zhang NC, Liu HJ. A systematic review of outcomes and complications of primary fingertip reconstruction using reverse-flow homodigital island flaps. Aesthetic Plast Surg. 2016;40(2):277-283. doi:10.1007/s00266-016-0624-y
-
Kim SK. Digital artery perforator flaps. J Reconstr Microsurg. 2015;24(2):50-55. doi:10.15596/arms.2015.24.2.50
-
Ekinci Y, Gürbüz K. Is the cross-finger flap a good option at the extensor zone defect? Jt Dis Relat Surg. 2020;31(2):267-272. doi:10.5606/ehc.2020.73030
-
Gurbuz K, Dogar F, Yontar Y. Comparison of clinical outcomes of heterodigital neurovascular island flap, reverse homodigital neurovascular island flap, and cross-finger flap used for fingertip reconstruction. Indian J Orthop. 2022;56(5):847-855. doi:10.1007/s43465-022-00605-8
-
Usami S, Kawahara S, Yamaguchi Y, Hirase T. Homodigital artery flap reconstruction for fingertip amputation: a comparative study of the oblique triangular neurovascular advancement flap and the reverse digital artery island flap. J Hand Surg Eur Vol. 2015;40(3):291-297. doi:10.1177/1753193413515134
-
Karjalainen T, Jokihaara J. A review and meta-analysis of adverse events related to local flap reconstruction for digital soft tissue defects. Hand Clin. 2020;36(1):107-121. doi:10.1016/j.hcl.2019.08.009
Figures

Figure 1. Intraoperative hetero- digital flap surgical technique and clinical outcome. a)Flap recipient side and donor side clinical view and planning. b) Flap dissection and elevation from the donor side. c) Flap placement to the fingertip defect side. d) Postoperative clinical view of the case at 6th week

Figure 2. Intraoperative homo- digital flap surgical technique and clinical outcome. a) Clinical view of the fingertip defect on index digit, donor side clinical view and planning. b) Flap dissection, elevation from the donor side and placement to the fingertip defect side. c) Postoperative clinical view of the case at 6th week
Tables
Table 1. Complications and flap survivals in each group
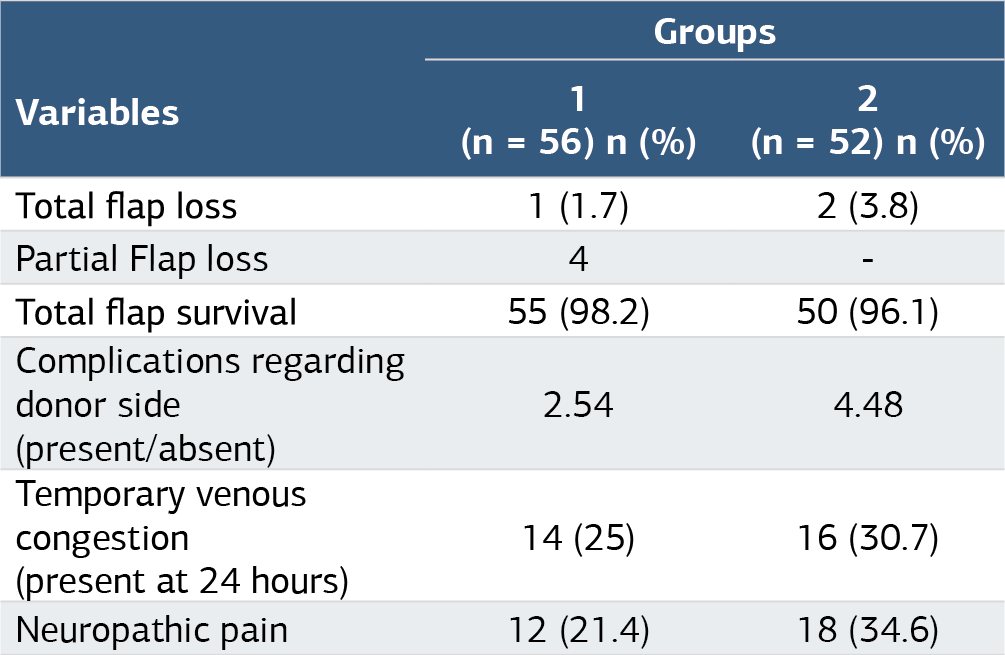
Table 2. Clinical Outcomes in each group

Quick-DASH: Disability of the Arm, Shoulder, and Hand questionnaire score CISS: Cold Intolerance Severity Score.
Table 3. ROM of each joint in each group

*when compared with group 1, statistically significant, Anova .03 MCP, metacarpopharangeal; PIP, proksimal interphalangeal; DIP, distal interphalangeal.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Feridun Arat, Burak Kuscu, Kadir Ismail Dere, Kaan Gurbuz. Multi-centric comparative analysis of the clinical and functional outcomes of two neuromuscular island flaps for fingertip defects: Hetero-digitalversus reverse homo-digital. Ann Clin Anal Med 2025;16(4):260-264. doi:10.4328/ACAM.22358
- Received:
- August 7, 2024
- Accepted:
- September 24, 2024
- Published Online:
- November 23, 2024
- Printed:
- April 1, 2025