
The role of amantadine in the anesthesia intensive care unit
Amantadine in ICU
Authors
Abstract
AimThe aim of this study is to provide information on patient-specific and clinical data relating to patients treated with amantadine in the intensive care unit, including changes in the Glasgow Coma Scale (GCS) score, patient demographics, length of stay in the Intensive Care Unit (ICU), duration of mechanical ventilation, drug dosage and route of administration.
MethodsPatients over 18 who received amantadine treatment from January 2014 to December 2019 were included in the study. Patients’ age, gender, diagnosis at hospitalization, comorbidities, history of cardiopulmonary resuscitation(CPR), history of head trauma, duration of mechanical ventilation, overall condition at the end of the treatment in the ICU, GCS score at admission and discharge, route of drug administration, and total drug dose were recorded retrospectively.
ResultsOf the 91 patients included in the study, 39 had a history of head trauma, and 25 had a history of cardiopulmonary resuscitation. 46 patients died. 43 were relocated to a level 2 ICU or award. The chosen route of administration was intravenous (I.V.) in 60.4% of the patients. The average difference between the GCS scores at admission and discharge in all patients showed an increase, but it was not statistically significant. The GCS score seemed to show a statistically significant increase in the head trauma subgroup.
ConclusionWe believe that amantadine can accelerate neurological recovery in unconscious intensive care patients, especially those with traumatic brain injury.
Keywords
Introduction
Amantadine, an N-methyl D-aspartate (NMDA) receptor antagonist, is an antiviral agent with dopaminergic effects. Another area of use for amantadine is related to improving neurological recovery in patients with traumatic brain injury.1 It is believed that amantadine stimulates and contributes to the recovery of the nervous system with its dopaminergic effect and prevents apoptosis by inhibiting the passage of calcium into the cell with its NMDA receptor antagonist effect.2 Cell culture studies have shown that amantadine increases the production of glial cell-derived neurotrophic factors (GDNF), thereby inhibiting neuroinflammation. Since reducing neuroinflammation can correct cognitive functions, researchers believe that amantadine can be used in postoperative cognitive dysfunction (POCD).3
Some publications found in the literature review report that the use of amantadine in various disorders of consciousness accelerates and contributes to neurological recovery.4 This study examined patients treated with amantadine due to impaired consciousness in our anesthesia Intensive Care Unit (ICU). It aimed to reveal the effect of the drug on the prognosis, most effective duration, dosage, and route of administration in achieving the optimal effect.
Materials and Methods
Amantadine-treated patients hospitalized in the Anesthesia ICU of Izmir Katip Çelebi University Ataturk Training and Research Hospital between January 1, 2014, and December 1, 2019, were retrospectively screened. Ninety-one patients over 18 years of age were recruited for the thesis study. The study was designed as a retrospective, comparative, and descriptive case series. The gender, age, and comorbidities of the patients were noted. Diagnoses at admission into the ICU were recorded. Regardless of patients’ diagnoses at admission, their history of cardiopulmonary resuscitation (CPR) before admission to the ICU and history of head trauma were checked, resulting in subgroups. All patients’ Glasgow Coma Scale (GCS) score at the time of admission (GCS on arrival), GCS score at the end of the ICU treatment (GCS on exit), condition at the end of the ICU treatment (dead, transferred to a ward or a level 2 ICU, discharged) were analyzed. Various parameters were investigated, including the total length of stay in intensive care (days), duration of mechanical ventilation during intensive care monitoring (days), route of administration of amantadine (I.V., tablet, I.V.+tablet), the day the drug was started after admission (start time), total dose, and duration of administration (days). GCS difference (= GCS on arrival – GKS on exit) was calculated collectively for all patients before subgrouping and then separately for the two subgroups to reveal any significant change in GCS scores for all patients. All variables were evaluated with descriptive statistics. GCS changes were compared. All subjects were grouped as ‘increased GCS’, ‘decreased GCS’, and ‘unchanged GCS’ according to the changes in their GCS scores. The groups were compared in terms of length of mechanical ventilation and length of stay in intensive care.
Ethical ApprovalThis study was approved by the Ethics Committee of İzmir Katip Çelebi University Atatürk Training and Research Hospital (Date: 09.01.2020, Decision No: 06).
Statistical AnalysisDescriptive statistics and frequency analyses (n,%) were performed for average ± standard deviation or median (range) values for all variables. The assumption of normality and homogeneity for the Glasgow Coma Scale scores on arrival and on exit was evaluated. Variables that were not distributed according to this assumption were subjected to the Wilcoxon signed-rank test separately in all patient groups, the head trauma subgroup and the CPR subgroup. The subjects were examined in three groups: increased, decreased, and unchanged GCS group according to changes in the GCS score. The Kruskall-Wallis test was applied for these non-normally and non-homogeneously distributed groups. Post hoc analysis was performed with the Tamhane test. Statistical significance was set at p<0.05. Statistical analysis was performed with SPSS 22.0 Edition software (Chicago, Ill).
Reporting GuidelinesThis study was prepared in accordance with the STROBE guideline.
Results
Descriptive statistical analysis was performed for all subjects. The mean age of the patients was 55 ± 21.29 (31.9%) were female and 62 (68.1%) were male.
Twenty-four patients had been hospitalized for motor vehicle accidents, and 15 patients had a diagnosis of fall. 6 patients had been followed up for myocardial infarction, and 8 patients had been followed up for a history of non-traumatic cerebrovascular accidents (CVA). 10 patients had been hospitalized for postoperative impaired consciousness. There were 4 patients diagnosed with pneumonia and generalized disorder. There were 2 patients for each aspiration, delirium tremens, and pulmonary edema. Three patients had been followed up for sepsis and acute renal failure. There was 1 patient follow-up for each of the following diagnoses: larynx cancer, anaphylaxis, eclampsia, electrolyte disorder, respiratory failure, disseminated intravascular coagulation, neuroleptic malignancy syndrome, and decompensated heart failure. 46 (50.5%) patients had at least one comorbidity, with hypertension (35%) and diabetes mellitus (23%) being the most common.
39 (42.9%) of the patients hospitalized in the ICU who were given amantadine had a history of head trauma. 25 (27.5%) of the amantadine-treated patients had received cardiopulmonary resuscitation before admission to the ICU. 41 (45.1%) of the patients treated with amantadine had an increase in their GCS score, while 34 (37.4%) had a decrease, and 16 (17.5%) patients did not have any change in their GCS score.
The mean GCS for all patients at admission to the ICU was 6.94 ± 3.58, the mean GCS at the end of the ICU treatment was 7.89 ± 5.09, and the mean GCS change was 0.94 ± 5.41. The median length of stay in the anesthesiology ICU was 36 (range 4-689) days. The median duration of mechanical ventilation for the patients when in the ICU was 29 (range 0-601) days. 2 (2.2%) of the treated patients were discharged home, 43
(47.3%) were transferred to a level 2 ICU or award, and 46 (50.5%) died. The mean duration of amantadine treatment in all cases was 8.6 ± 7.8 days. The median day when the drug had been started was day 8 (range 1-192).The preferred route of administration was I.V. in 55 (60.4%), tablet form in 5 (5.5%), and combined (tablet+I.V.) in 31 (34.1%). The average total dose of the administered amantadine was 2850 ± 2254 milligrams. Descriptive data are summarized in Table 1 (Table 1). The patients were divided into three groups according to the change in their GCS scores: the GCS score increased in 41 patients, decreased in 34 patients, and remained the same in 16 patients. The average duration of mechanical ventilation was 44.5 ± 71, 96.7 ± 120, and 29.5 ± 38 days, respectively, and the mean length of stay in the ICU was 76.9 ± 99, 101.7 ± 132, 32.2 ± 39 days, respectively. There was a statistical difference among these three groups in terms of duration of mechanical ventilation and length of stay in the ICU (p=0.001, p=0.001, respectively). Post-hoc analyses showed no statistically significant difference between the group with increased GCS score and the one with decreased GCS score in terms of duration of mechanical ventilation and length of stay in the ICU (p=0.089, p=0.752, respectively). The length of stay in the ICU was significantly lower in the group with unchanged GCS scores as compared to the groups with increased or decreased GCS scores. The duration of mechanical ventilation was significantly lower in the group with unchanged GCS scores as compared to the group with decreased GCS scores. Post-hoc analyses are detailed in Table 2 (Table 2).
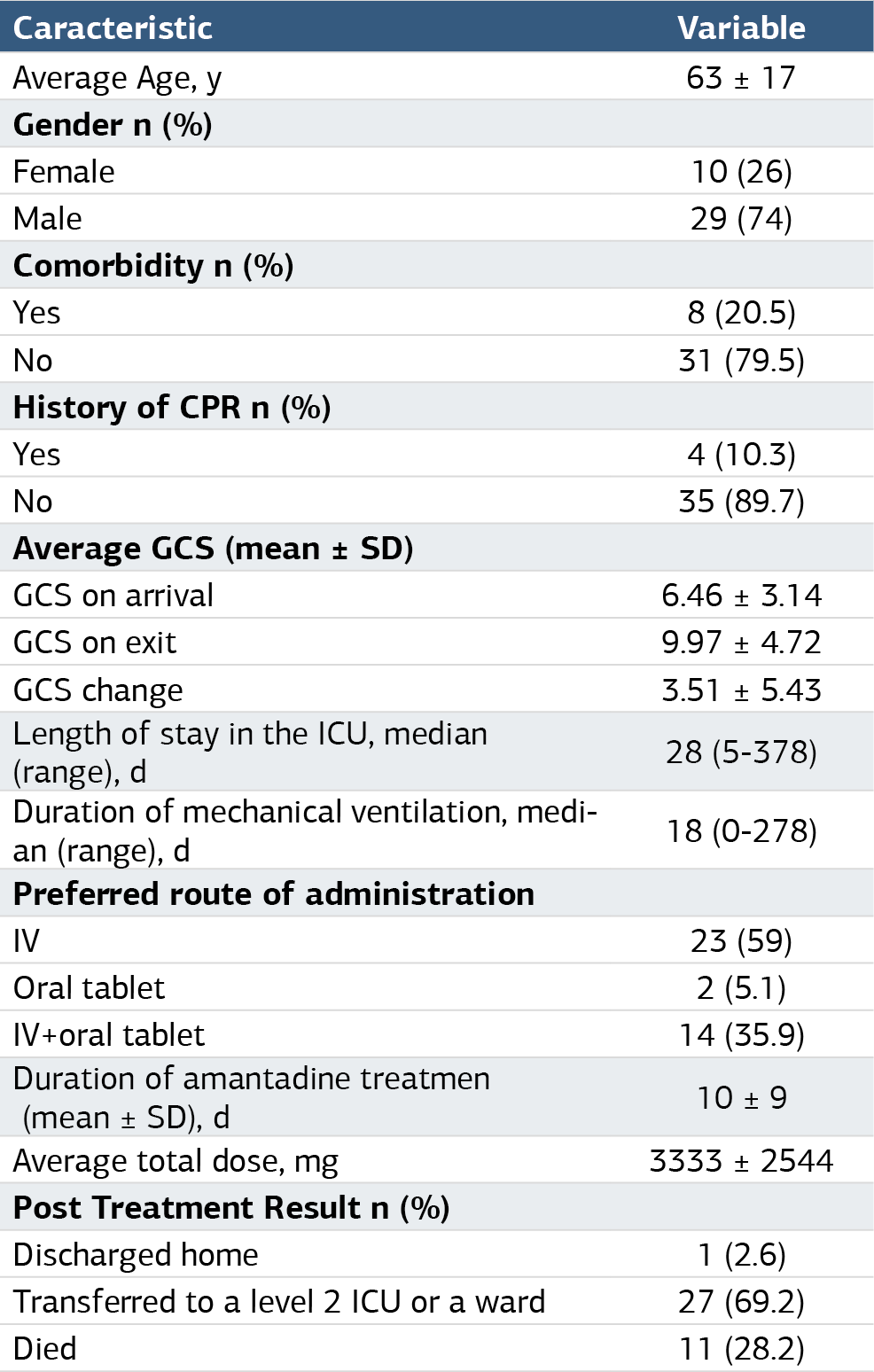
There were 39 patients in the head trauma subgroup. Their mean age was 63 ± 17; 10 (31.9%) of them were female and 29 (68.1%) were male. 8 (20.5%) of the patients in this group had at least one comorbidity.
For this subgroup, the average GCS score at admission to the ICU, GCS on exit, and GCS variation were 6.46 ± 3.14, 9.97 ± 4.72, and 3.51 ± 5.43, respectively.
The patients’ median length of stay in the anesthesia ICU and duration of mechanical ventilation were 28 days (range 5-378) and 18 days (range 0-278), respectively.
The route of administration of amantadine was I.V., tablet, and combined (I.V.+tablet) form in 23 (29%), 2 (5.1%), and 14 (35.9%) patients, respectively.
In the head trauma group, the average duration of use and the total dose of amantadine were 10 ± 9 days and 3333 ± 2544 mg, respectively. The median day when the drug had been started was day 6 (range 1-40).
Of these cases, 1 (2.6%) was discharged home, 27 (69.2%) were transferred to a level 2 ICU or a ward, while 11 (28.2%) died. Descriptive data are summarized in Table 3 (Table 3). In the subgroup of patients followed after CPR, the mean age was 55 ± 18; 8 (32%) of the subjects were female, and 17 (68%) were male. There was at least one comorbidity in 13 (52%) patients.
For this subgroup, the average GCS at admission to the ICU, GCS on exit, and GCS variation were 5.88 ± 3.59, 6.84 ± 4.70, and 0.96 ± 4.91, respectively.
The patients’ median length of stay in the anesthesia ICU and duration of mechanical ventilation were 78 days (8-689) and 63 days (4-601), respectively.
The route of administration of amantadine was I.V. in 12 (48%) patients and combined (I.V.+tablet) form in 13 (52%) patients. In the post-CPR group, the average duration of use and the total dose of amantadine were 10 ± 8 days and 3096 ± 2495 mg, respectively. The median day when the drug had been started was day 12 (range 2-91).
Of these cases, 1 (4%) was discharged home, 10 (40%) were transferred to a level 2 ICU or a ward, while 14 (56%) died. Taken together, there was no statistically significant increase in GCS scores in patients treated with amantadine (without subgrouping) (p=0.089).
The subgroup analysis examining the difference between the GCS on arrival and GCS on exit in patients admitted to the anesthesia ICU for head trauma showed a statistically significant increase in the GCS score (p=0.001). The subgroup analysis examining the difference between the GCS on arrival and GCS on exit in patients admitted to the anesthesiology ICU post-CPR found no statistically significant increase in the GCS score (p=0.275).
Discussion
When all study patients were considered together, amantadine treatment was seen to cause an increase in the GCS score, but this was not statistically significant. In the subgroup of patients with impaired consciousness caused by head trauma, amantadine treatment was found to result in a statistically significant improvement in the GCS score. Neurological recovery in head trauma patients was consistent with prior studies.1,5,6,7,8,9
One study by Ghate et al. examined 50 patients with traumatic brain injury who were treated with amantadine. In this study, all patients were evaluated before and after treatment with a Full Outline of UnResponsiveness Score (FOUR), Glasgow Outcome Scale (GOS), and Disability Rating Scale (DRS). They reported an improvement in patients’ neurological evaluation scores.6 In a study by Meythaler et al., patients with traumatic brain injury were divided into placebo and control groups and were treated with amantadine at different times. The results of their study found an improvement in DRS, GOS, and Mini-Mental State Examination (MMSE) scores at those times when patients were actively taking amantadine.7
In a study that first reported neurostimulant use in post-CPR care, neurostimulants were used in addition to therapeutic hypothermia. Patients who received neurostimulants were compared with the therapeutic hypothermia group that did not take neurostimulants and were found to have a higher chance of discharge and tended to recover better.10 Our study detected an increase in the GCS score after treatment with amantadine, but the increase was not statistically significant.
In another study, patients with CVA were given amantadine, and after three months, the treatment group was compared with the control group by using the National Institutes of Health Stroke Scale (NIHSS), Modified Rankin Scale (MRS), and Barthel Index for Activities of Daily Living. The comparison showed better neurological recovery in the group treated with amantadine.10 In our study, there were eight patients followed up for CVA of non-traumatic origin. Only 2 had an increase in their GCS score. Amantadine has been shown to be useful in improving POCD in animals.3 In a controlled study of 344 rats by Hongyin Tan et al., amantadine was shown to reduce postoperative inflammation. This study is the first to show the possible therapeutic effect of amantadine on POCD.3 In our study, there were 11 patients who were followed up in intensive care postoperatively and who were considered good candidates for amantadine treatment. Of these 11 patients, seven died, and in the remaining four patients, the GCS score on exit increased by an average of 5 points compared to the GCS score on arrival. We are of the opinion that in this patient group, neurological recovery is promising, but the results should be further supported by studies on a larger number of patients.
To date, no effective drugs have been found for the treatment and prophylaxis in the current COVID-19 pandemic. However, scientists are investigating the effectiveness or preventiveness of the known drugs used to treat other diseases against COVID-19. Recently, it has been reported that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) severely infects the brain stem in animals and humans and may cause not only respiratory but also neurological symptoms.11 A study has been conducted based on a survey to assess whether amantadine and memantine would show protective antiviral efficacy against COVID-19 in individuals with neurological diseases. This study examined ten patients with multiple sclerosis and five patients with Parkinson’s disease using amantadine, as well as seven patients with cognitive impairment using memantine, all with COVID-19 viral infection confirmed by the polymerase chain reaction (PCR) test. Patients were followed up during and at the end of the 2-week self-isolation and were found to have no symptoms of the viral infection, with also no progression in their primary neurological diseases.12
Each clinic has different experiences with the use and dose of amantadine. Although there is no clear data on dosage in the literature, our experience suggests that using 200 mg I.V. amantadine b.i.d. for five days, followed by 100 mg tablets b.i.d. for ten days, was the optimal time and dose for our clinic.
Limitations
Our study has some limitations in that it was retrospective and had an insufficient number of patients for forming different groups. Moreover, the GCS scores evaluated in our study were the GCS scores evaluated before admission into the ICU and before exit, regardless of the days when amantadine was started and discontinued. Studies using different scoring systems and different neurological evaluation methods could provide more detailed and effective results in the evaluation of neurological recovery and, thus, better clarify the effect of amantadine.
Conclusion
Post-CPR patients and patients with CVA, as well as intensive care patients in whom organic causes have been ruled out but who have not regained consciousness, and patients with postoperative disorders of consciousness, maybe the next group targeted by researchers for the use of amantadine. Prospective, randomized, controlled, and larger-scale studies are needed to better identify patient groups for amantadine treatment, to observe potential side effects, and to determine the optimal dose and duration of use of amantadine.
The unique aspect of our study is that it was not limited to one single group of patients with the same diagnosis, such as patients with a history of traumatic brain injury; instead, it covered patients who were followed up in the ICU with different diagnoses and who did not regain consciousness.
We believe that treatment with amantadine contributes to neurological recovery, especially in patients with traumatic brain injury. We could not find another study in the literature that collectively evaluated patients who were treated with amantadine for impaired consciousness in the ICU without distinguishing between the reasons for their hospitalization. This is what makes our study the first of its kind.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The need for informed consent was waived because anonymized data were used.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CPR: Cardiopulmonary resuscitation
CVA: Cerebrovascular accident
GCS: Glasgow Coma Scale
ICU: Intensive care unit
I.V.: Intravenous
NMDA: N-methyl-D-aspartate
POCD: Postoperative cognitive dysfunction
References
-
Saniova B, Drobny M, Kneslova L, Minarik M. The outcome of patients with severe head injuries treated with amantadine sulphate. J Neural Transm (Vienna). 2004;111(4):511-514. doi:10.1007/s00702-004-0112-4
-
Ghalaenovi H, Fattahi A, Koohpayehzadeh J, et al. The effects of amantadine on traumatic brain injury outcome: a double-blind, randomized, controlled, clinical trial. Brain Inj. 2018;32(8):1050-1055. doi:10.1080/02699052.2018.1476733
-
Zhang J, Tan H, Jiang W, Zuo Z. Amantadine alleviates postoperative cognitive dysfunction possibly by increasing glial cell line-derived neurotrophic factor in rats. Anesthesiology. 2014;121(4):773-785. doi:10.1097/aln.0000000000000352
-
Metin Aksu N, Senlikci H, Akkas M, Ozmen MM. The neurological improvement of a patient after amantadine infusion. J Acad Emerg Med Case Rep. 2013;4:161. doi:10.5505/jaemcr.2013.34713
-
Giacino JT, Whyte J, Bagiella E, et al. Placebo-controlled trial of amantadine for severe traumatic brain injury. N Engl J Med. 2012;366(9):819-826. doi:10.1056/nejmoa1102609
-
Ghate PS, Bhanage A, Sarkar H, Katkar A. Efficacy of amantadine in improving cognitive dysfunction in adults with severe traumatic brain injury in Indian population: a pilot study. Asian J Neurosurg. 2018;13(3):647-650. doi:10.4103/ajns.ajns_272_16
-
Meythaler JM, Brunner RC, Johnson A, Novack TA. Amantadine to improve neurorecovery in traumatic brain injury-associated diffuse axonal injury: a pilot double-blind randomized trial. J Head Trauma Rehabil. 2002;17(4):300-313. doi:10.1097/00001199-200208000-00004
-
Beers SM, Skold A, Dixon CE, Adelson PD. Neurobehavioral effects of amantadine after pediatric traumatic brain injury: a preliminary report. J Head Trauma Rehabil. 2005;20(5):450-463. doi:10.1097/00001199-200509000-00006
-
Sawyer E, Mauro LS, Ohlinger MJ. Amantadine enhancement of arousal and cognition after traumatic brain injury. Ann Pharmacother. 2008;42(2):247-252. doi:10.1345/aph.1k284
-
Krivonos OV, Amosova NA, Smolentseva IG. Use of the glutamate NMDA receptor antagonist PK-Merz in acute stroke. Neurosci Behav Physiol. 2010;40(5):529-532. doi:10.1007/s11055-010-9292-6
-
Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV-2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. 2020;92(6):552-555. doi:10.1002/jmv.25728
-
Rejdak K, Grieb P. Adamantanes might be protective from COVID-19 in patients with neurological diseases: multiple sclerosis, parkinsonism, and cognitive impairment. Mult Scler Relat Disord. 2020;42:102163. doi:10.1016/j.msard.2020.102163
Tables
Table 1. Descriptive data of all cases treated with amantadine
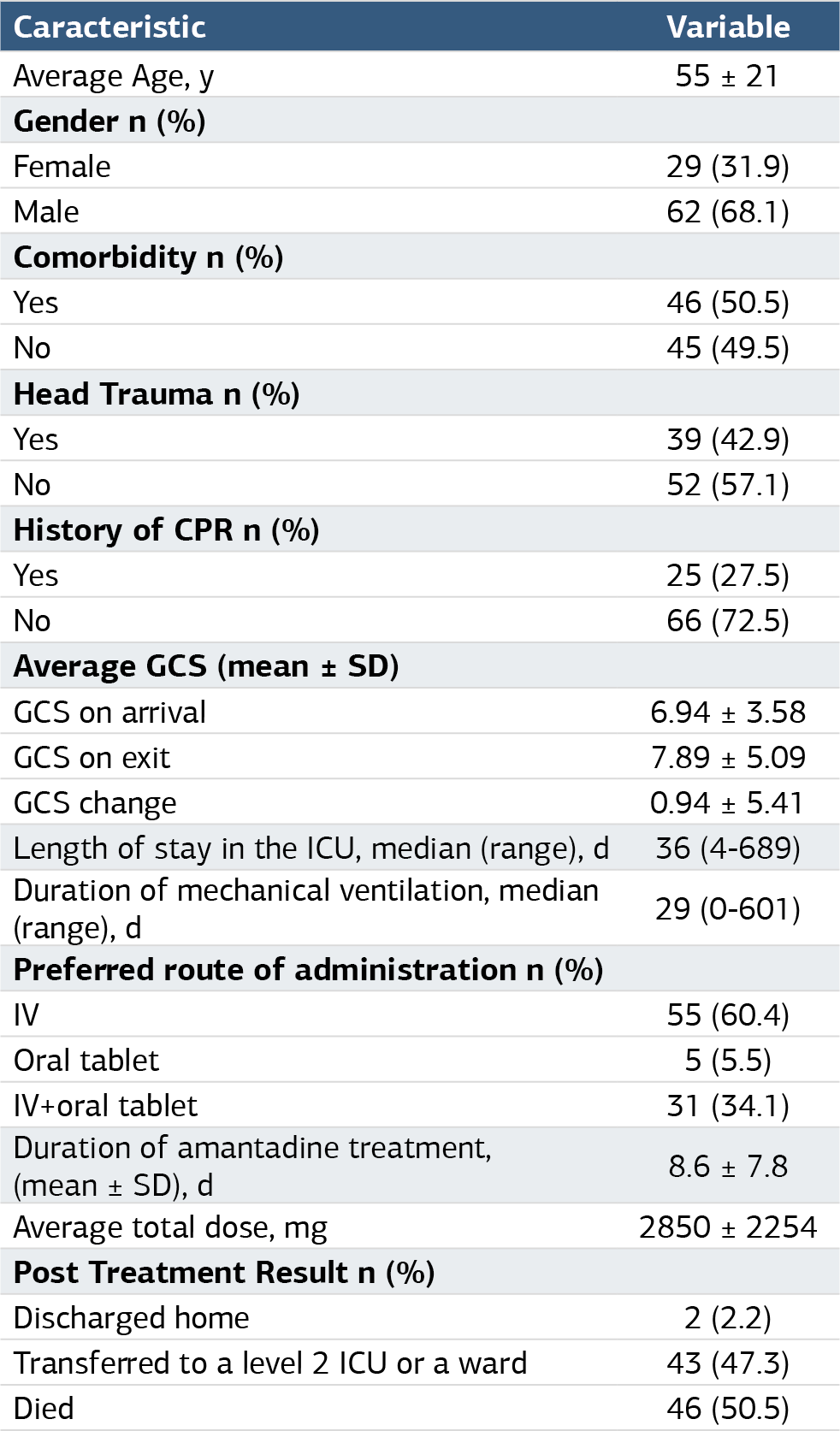
Table 2. Post hoc analysis of mechanical ventilation and length of stay in intensive care unit according to GCS changes

Table 3. Descriptive data of cases treated with amantadine for head trauma
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ezgi Balıkoğlu, Murat Aksun, Mehmet Ali Coşar, Senem Girgin, Mensure Çakırgöz, Atilla Şencan, Nagihan Karahan. The role of amantadine in the anesthesia intensive care unit. Ann Clin Anal Med 2025;16(5):331-335. doi:10.4328/ACAM.22364
- Received:
- August 8, 2024
- Accepted:
- October 21, 2024
- Published Online:
- December 14, 2024
- Printed:
- May 1, 2025