
Effectiveness of manual lymph drainage and low level laser treatment inimpacted lower molar surgery
Lymph drainage and laser
Authors
Abstract
AimThe aim of this study was to compare the efficacy of manual lymphatic drainage (MLD) and low level laser therapy (LLLT) on postoperative pain, edema and trismus in the impacted lower third molar tooth (ILTMT) surgery.
MethodsThe study included 36 patients with a mean age of 25.7 ± 5.9 years. Patients were randomized into 3 groups: MLD, LLTT and control groups. Pain (Visual Analogue Scale-VAS), edema (craniometric measurement) and trismus (maximum interincisal distance measurement) were evaluated. Evaluations were made before surgery, 24, 48 and 72 hours after surgery, and on the 7th day after surgery.
ResultsThe mean pain level between the 4th and 7th days of the two treatment groups and the use of additional pain medication during the treatment were significantly lower than the control group. The mean edema increase and mouth opening values did not differ significantly between the treatment groups in the postoperative 7th day compared to the preoperative period, but it was significantly higher in the control group.
ConclusionIt was concluded that MLD and LLLT after ILTMT surgery can be used effectively in the clinic to reduce pain and edema and improve mouth opening. It is thought that our study will provide a basis for future studies on MLD treatment in areas such as oral and maxillofacial surgery as well as orthognathic surgery.
Keywords
Introduction
Impacted lower third molar tooth (ILTMT) is one of the most frequently performed operations in oral and maxillofacial surgery.1 Edema, trismus, paresthesia, mandibular fracture and hemorrhage are among the frequently observed conditions in the early and late periods after ILTMT surgery.2,3 The variables underlying these changes are complex, but the inflammatory process caused by trauma is important. It is almost inevitable that pain, edema and trismus will occur as a result of the inflammatory response. This situation can lead to negative effects of living conditions, prolongation of the recovery process, and therefore social and economic losses.4,5,6
Post-surgical pain begins when the effect of anesthesia wears off, reaches its highest point in the first 3-5 hours, and then gradually decreases until the seventh day.5,6 Edema usually peaks between 12-48 hours and may take 5-7 days to resolve completely.7 The resulting edema surrounds the masseter muscle, causing decreased mandibular movements and reduced mouth opening. This condition, defined as trismus, may occur due to surgical procedures and local anesthesia. Trismus usually reaches its highest level on the 2nd day of surgery and completely decreases on the 7th day.8,9
In order to reduce complications, research has been conducted on treatment modalities such as analgesics, steroid and non-steroidal anti-inflammatory (NSAID) drugs, cryotherapy, different flap techniques, and LLLT.7,8,9,10,11,12 In one study, MLD application was observed.13 Since no effect was observed at the expected level, more reliable and comprehensive studies are needed. At the end of the study, it is thought that it will provide important data regarding the widespread applicability of MLD treatment as an alternative or complementary treatment to LLLT treatment in ILTMT surgery.
Materials and Methods
ParticipantsThe study was carried out with 36 patients aged between 18-45 who came to Faculty of Dentistry Department of Oral and Maxillofacial Surgery within the scope of 2018-2019 and who could undergo surgical extraction on their ILTMTs as a result of their radiographic and clinical evaluations. All participating patients signed an approved “Informed Consent Form” after being given detailed information about the purpose and method of the study.
Patient selection was made to include patients who fit American Society of Anesthesiologists 1 in the classification of ASA, have impacted teeth with bone retention, have sufficient cognitive capacity, and are between the ages of 19-45. Women who have a systemic disease that prevents oral surgery, have an infection, are allergic to the drugs to be given, have received NSAID treatment in the last 3 months, have a carotid endoarterectomy, have an inflammatory skin disease on the face or neck, have a hyperthyroid disorder, are receiving psychiatric treatment, are pregnant and are breastfeeding are included in the study. These patients were excluded from the study.
AssesmentDemographic information of individuals was recorded through the Personal Information Form. Pain levels were measured using the Visual Analogue Scale (VAS). The amount of edema was determined using the craniometric method. Distances measured from three separate extra-oral regions on the face (between the outer corner of the eye and the angulus mandible, between the tragus and the corner of the mouth, and between the tragus and the pogonion) were used to record the facial volume and the amount of edema. Trismus evaluation was made by measuring the maximum distance between the upper and lower teeth in millimeters while the patient was sitting in an upright position. Edema and trismus measurements were repeated at certain time periods (24th, 48th, 72nd hour and 7th day) before and after surgery.
Treatment ProgramA total of 36 patients participating in the study were randomly selected and divided into three groups: control group (n = 12), MLD group (n = 12) and LLLT group (n = 12). The average age of the participants, whose ages ranged from 19 to 45, was determined as 25.7 ± 5.9. MLD and LLLT were applied to the patients once a day for three days after surgery (at the 24th, 48th and 72nd hours) according to their groups. The control group received only routine drug therapy and ice therapy. As routine postoperative antibiotic prophylaxis, 875 mg of amoxicillin and 125 mg of clavulanic acid were given twice a day, as well as chlorhexidine gluconate mouthwash three times a day. Additionally, all individuals were asked to apply ice intermittently for the first 24 hours.
LLLT treatment was applied with a Medency brand laser device of Italian origin, at a wavelength of 810 nm, in continuous mode, with a power of 100 mW and an energy density of 4 J/ cm2 (0.1 W x 120 sec for a total of 12 J). The treatment was performed including intraoral and extraoral areas. Intraoral laser application was planned to be applied to the surgical area, masseter and internal pterygoid muscle, and retromolar area. These applications were performed without contact with the mouth, from a distance of approximately 1 cm. Extraoral application was made to the insertion area of the masseter muscle. Laser treatment was performed by an experienced dentist.
During the MLD technique, hand positions are adjusted taking into account the anatomy and physiology of the lymphatic system. The stroke sequence includes work and rest phases in which manual pressure slowly increases and decreases. The pressure intensity is adjusted to increase the elasticity of the skin and subcutaneous tissue to prevent unwanted vasodilation and lymphangiospasm. The operating time of each pulse was determined as 1 second, taking into account the viscosity of the lymph fluid. Each stroke was repeated 5-7 times for manual lymphatic drainage to be effective. The way the strokes work is to direct the lymph flow from blocked areas to healthy areas.
Ethical ApprovalThis study was approved by the Ethics Committee of Istanbul Medipol University (Date: 15.08.2018, Decision No: 447).
Statistical AnalysisThe significance level was set at 0.05; In this context, it was concluded that there was a p<0.05 was considered statistically significant, and that there was no significant difference if p>0.05. SPSS 22.0 package program was used for statistical analysis.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
According to the findings of our study, the groups did not differ significantly (p>0.05) in terms of demographic characteristics (Table 1). As a result of our study, it was observed that ILTMT surgery is performed more frequently in women. In all participant groups, the highest pain levels were reported to be at the 6th hour. No significant difference was observed between the groups in VAS scores before surgery and on the 2nd day after surgery. However, VAS scores from day 4 to day 7 in the treatment groups were lower than those in the control group. It was determined that participants in the MLD and LLLT groups were significantly less likely to receive additional analgesics after surgery compared to the control group. When pain was compared by gender, it was observed that women had lower pain tolerance than men and were more prone to analgesic medication.
No significant difference was observed between the groups in terms of mean edema levels before surgery. In all groups, edema levels were highest on the 2nd day after surgery. Moreover, in all groups, the average edema level on the 2nd day after surgery showed a significant increase compared to the pre-surgery period, while the average edema level on the 7th day after surgery showed a significant decrease compared to the 2nd day after surgery. It was reported that the edema level on the 2nd and 7th postoperative day did not show a significant difference between the treatment groups and was significantly higher in the control group compared to the MLD and LLLT groups.
There was no significant difference in the increase in edema on the 2nd day after surgery compared to before surgery between the MLD and LLLT groups. However, it was found that the increase in edema on the second day after surgery was higher in the control group compared to the MLD and LLLT groups. While edema values on the 7th day after surgery in the MLD group did not show a significant change compared to the pre-surgery, they showed a significant increase in the control and LLLT groups. No significant difference was observed in the increase in edema on the 7th day between the MLD and LLLT groups. However, in the control group, the increase in edema on the 7th day after surgery compared to before surgery was significantly higher than in the MLD and LLLT groups (Table 2). No difference was observed in preoperative trismus values between the groups. However, trismus averages were at their lowest level on the 2nd day after surgery in all groups. In all groups, the trismus value on the 2nd and 7th day after surgery showed a significant decrease compared to the pre-surgery, while the trismus value on the 7th day after surgery showed a significant increase compared to the 2nd day after surgery. No significant difference was observed between the groups in terms of trismus values on the 2nd and 7th days after surgery. While the decrease in trismus value on the second day after surgery compared to before surgery did not show a significant difference between the MLD and LLLT groups, it was found to be significantly higher in the control group compared to the MLD and LLLT groups. While the trismus value on the 7th day after surgery compared to the pre-surgery did not show a significant difference in the MLD and LLLT groups, this difference was significant in the control group. Moreover, although it was not statistically significant, the trismus value of the MLD group on the 7th postoperative day was very close to the postoperative value (Table 3).
Discussion
Differences are observed between the results of various studies examining the effects of LLLT after ILTMT surgery. For example, in a meta-analysis study conducted by BrignardelloPetersen et al., it was reported that DELT did not have any positive effect on pain and edema, but provided a moderate benefit for trismus.14 However, in a study conducted by He et al., DELT was reported to be effective in edema, trismus, and pain.9 These differences are thought to be due to the lack of a standard approach to variables such as the properties of the laser applied and the application protocol.15 There are many studies in the literature on the effect of LLLT wavelength and energy density in reducing complications.15,16 In our study, it was determined that the 810 nm wavelength affects deep tissues and is in the range where biostimulation effects are best observed, and 4J/cm² energy density was preferred because it is a dose that generally yields positive results. According to our results, none of the participants in the LLLT group needed to use additional painkillers, and the VAS scores recorded from the 4th day to the 7th day after surgery were lower than the control group. In addition, the increase in edema and the decrease in trismus values on the 2nd and 7th days after surgery compared to before surgery were found to be significantly higher in the control group compared to the LLLT group. These findings show that laser is an effective method in reducing complications. The issue of the number of sessions in which laser treatment will be applied is still research-oriented. Although the application protocol we use is frequently encountered in the current literature, the application frequency can vary from a single session to four sessions. In the literature, it is recommended to perform at least five sessions for MLD therapy to yield positive results, but since the patients recover in a short time after this surgery and since the work will be done in a small area, it was thought that three sessions would be sufficient and the treatment protocol was created accordingly.
There are also studies comparing the effectiveness of LLLT according to the application region. Kahraman reported in his study that intraoral application provides more effect than extraoral application.6 Aras et al., in their study comparing the effects of extraoral and intraoral application, observed that extraoral laser application was more effective than intraoral application in reducing edema and trismus.17 Ferrante et al., in their study where they performed combined application, observed that pain, edema and trismus values were lower compared to the control group.18 In our study, combined laser application was performed, similar to the findings in the literature. The results showed that pain, edema and trismus values were significantly lower in the laser group than in the control group.
New areas for the medical use of MLD are being discovered every day. Increasing drug allergies and drug-related side effects increase the tendency towards alternative methods such as MLD. Yaedu et al. found that the edema level in the MLD group after bimaxillary orthognathic surgery decreased faster compared to the control group, but there was no significant difference between the groups in terms of edema and pain. Additionally, it has been reported that there is no relationship between pain and edema and that surgical duration does not affect edema. This study shows that MLD treatment after orthognathic surgery is effective in reducing post-surgical facial edema.19 MLD treatment is thought to increase the carrying capacity of lymph vessels by increasing lymphangiomotor activity and stimulating the lymph nodes. In their study in 2017, Szolnoky and colleagues investigated the effects of MLD on pain and edema after bilateral ILTMT surgery. As a result of the study, it was reported that with MLD application, the VAS score, which was 35.5 ± 20.60 before surgery, decreased to 22 ± 19.32 mm. A significant positive effect was observed on the quality of life of the MLD group. When the distances between anatomical regions determined to evaluate the intensity of edema were examined, it was observed that there were positive and significant differences in the MLD group compared to the control group.13 The method of our study is similar to the previous study. MLD treatment was administered in 45-minute sessions once a day for the first three days after surgery. In the comparison between the MLD and LLLT groups, although no statistically significant difference was detected in VAS scores during the specified time periods, it was observed that the pain level in the MLD group was lower throughout the entire process. It has been thought that MLD is performed by applying light pressure and is more effective than laser treatment in increasing lymphatic drainage by directly stimulating new lymphatic pathways. It is thought that the manual application of MLD, accompanied by a specialist physiotherapist, and the fact that it is a technique that gives confidence to the patient, may have a positive effect on the treatment results.
Limitations
The small sample size, short follow-up period, and single-center design may limit the generalizability of the findings. In addition, insufficient reporting of randomization and possible lack of blinding may introduce bias.
Conclusion
It was concluded that MLD and LLLT after ILTMT surgery can be used effectively in the clinic to reduce pain and edema and improve mouth opening. It is thought that our study will provide a basis for future studies on MLD treatment in areas such as oral and maxillofacial surgery as well as orthognathic surgery.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ASA: American society of anesthesiologists
ILTMT: Impacted lower third molar tooth
LLLT: Low-level laser therapy
MLD: Manual lymphatic drainage
NSAID: Non-steroidal anti-inflammatory drug
VAS: Visual analogue scale
References
-
Alan H, Yolcu Ü, Koparal M, Özgür C, Öztürk SA, Malkoç S. Evaluation of the effects of low-level laser therapy on swelling, pain, and trismus after removal of impacted lower third molar. Head Face Med. 2016;12(1):1-6.
-
Farhadi F, Eslami H, Majidi A, Fakhrzadeh V, Ghanizadeh M, KhademNeghad S. Evaluation of adjunctive effect of low-level laser therapy on pain, swelling and trismus after surgical removal of impacted lower third molar: a double blind randomized clinical trial. Laser Ther. 2017;26(3):181-187. doi:10.5978/islsm.17-or-13
-
Aravena PC, Astudillo P, Miranda H, Manterola C. Reliability and validity of measuring scale for postoperative complications in third molar surgery. BMC Oral Health. 2018;18(1):1-7.
-
McGrath C, Comfort MB, Lo EC, Luo Y. Changes in life quality following third molar surgery: the immediate postoperative period. Br Dent J. 2003;194(5):265-268. doi:10.1038/sj.bdj.4809930
-
Pol R, Ruggiero T, Gallesio G, Riso M, Bergamasco L, Mortellaro C, et al. Efficacy of anti-inflammatory and analgesic effects of superpulsed low-level laser therapy after impacted mandibular third molar extractions. J Craniofac Surg. 2016;27(3):685-690. doi:10.1097/scs.0000000000002523
-
Kahraman SA, Cetiner S, Strauss RA. The effects of transcutaneous and intraoral low-level laser therapy after extraction of lower third molars: a randomized single blind, placebo-controlled dual-center study. Photomed Laser Surg. 2017;35(8):401-407. doi:10.1089/pho.2016.4252
-
Laureano Filho JR, de Oliveira e Silva ED, Batista CI, Gouveia FM. The influence of cryotherapy on reduction of swelling, pain and trismus after third-molar extraction: a preliminary study. J Am Dent Assoc. 2005;136(6):774-778. doi:10.14219/jada.archive.2005.0261
-
Moraschini V, Hidalgo R, Porto Barboza E. Effect of submucosal injection of dexamethasone after third molar surgery: a meta-analysis of randomized controlled trials. Int J Oral Maxillofac Surg. 2016;45(2):232-240. doi:10.1016/j.ijom.2015.09.008
-
He WL, Yu FY, Li CJ, Pan J, Zhuang R, Duan PJ. A systematic review and meta-analysis on the efficacy of low-level laser therapy in the management of complication after mandibular third molar surgery. Lasers Med Sci. 2015;30(6):1779-1788. doi:10.1007/s10103-014-1634-0
-
Balevi B. Laser therapy has minimal clinical efficacy at reducing postsurgical complications after the removal of impacted mandibular third molars. J Evid Based Dent Pract. 2018;18(2):162-164. doi:10.1016/j.jebdp.2018.03.006
-
Brajković D, Biočanin V, Milič M, Vučetić M, Petrović R, Brković B. Quality of analgesia after lower third molar surgery: a randomized, double-blind study of levobupivacaine, bupivacaine and lidocaine with epinephrine. Vojnosanit Pregl. 2015;72(1):50-56.
-
Kazancioglu HO, Ezirganli S, Demirtas N. Comparison of the influence of ozone and laser therapies on pain, swelling, and trismus following impacted third-molar surgery. Lasers Med Sci. 2014;29(4):1313-1319. doi:10.1007/s10103-013-1300-y
-
Szolnoky G, Szendi-Horváth K, Seres L, Boda K, Kemény L. Manual lymph drainage efficiently reduces postoperative facial swelling and discomfort after removal of impacted third molars. Lymphology. 2007;40(3):138-142.
-
Brignardello-Petersen R, Carrasco-Labra A, Araya I, Yanine N, Beyene J, Shah PS. Is adjuvant laser therapy effective for preventing pain, swelling, and trismus after surgical removal of impacted mandibular third molars? A systematic review and meta-analysis. J Oral Maxillofac Surg. 2012;70(8):1789-1801. doi:10.1016/j.joms.2012.01.008
-
Landucci A, Wosny AC, Uetanabaro LC, Moro A, Araujo MR. Efficacy of a single dose of low-level laser therapy in reducing pain, swelling, and trismus following third molar extraction surgery. Int J Oral Maxillofac Surg. 2016;45(3):392-398. doi:10.1016/j.ijom.2015.10.023
-
Clokie C, Bentley KC, Head TW. The effects of the helium-neon laser on postsurgical discomfort: a pilot study. J Can Dent Assoc. 1991;57(7):584-586.
-
Aras MH, Güngörmüş M. Placebo-controlled randomized clinical trial of the effect of two different low-level laser therapies (LLLT)—intraoral and extraoral—on trismus and facial swelling following surgical extraction of the lower third molar. Lasers Med Sci. 2010;25(5):641-645. doi:10.1007/s10103-009-0684-1
-
Ferrante M, Petrini M, Trentini P, Perfetti G, Spoto G. Effect of low-level laser therapy after extraction of impacted lower third molars. Lasers Med Sci. 2013;28(3):845-849. doi:10.1007/s10103-012-1174-4
-
Yaedú RYF, Mello MDAB, Tucunduva RA, Da Silveira JSZ, Takahashi MPMS, Valente ACB. Postoperative orthognathic surgery edema assessment with and without manual lymphatic drainage. J Craniofac Surg. 2017;28(7):1816-1820. doi:10.1097/scs.0000000000003850
Tables
Table 1. Comparison of demographic characteristics of groups
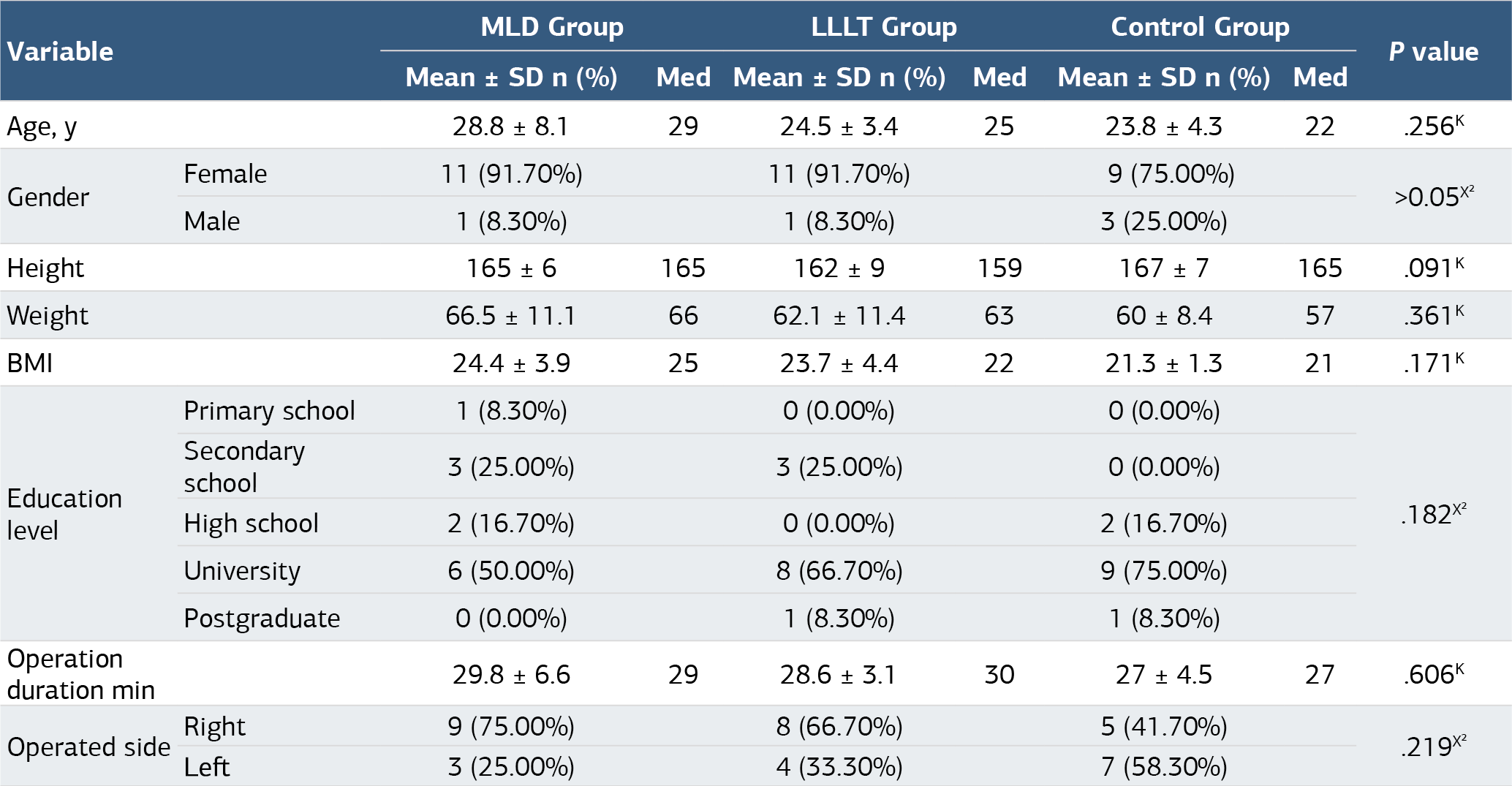
K Kruskal-wallis (Mann-whitney u test) / X² Ki-kare test, Manuel lymphatic drainage; LLLT: Low level laser therapy, Med: median; SD: Standard Deviation
Table 2. Comparison of Mean Edema Values of Groups Over Time

K Kruskal-wallis (Mann-whitney u test) /w Wilcoxon test
Table 3. Comparison of Trismus Values of Groups According to Time

K Kruskal-wallis (Mann-whitney u test) /w Wilcoxon test
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Büşra İnce, Fatma Mutluay, Barış Çağrı Delilbaşı. Effectiveness of manual lymph drainage and low level laser treatment inimpacted lower molar surgery. Ann Clin Anal Med 2025;16(1):72-76. doi:10.4328/ACAM.22374
- Received:
- August 20, 2024
- Accepted:
- September 24, 2024
- Published Online:
- November 4, 2024
- Printed:
- January 1, 2025