
Applicability of do-not-attempt-resuscitation in the emergency department
Do not attempt resuscitation
Authors
Abstract
AimThe issue of Do Not Attempt Resuscitation (DNAR), which is still being debated all over the world, is extremely complex and has not yet been discussed extensively in our country. Our aim in this study is to determine the place of DNAR in emergency services and the applicability of the DNAR concept.
MethodsThis study was designed as a cross-sectional survey in 2013 in Türkiye. The questions were designed to examine physicians' approaches to the concept of DNAR, whether they apply this concept, and why.
ResultsA total of 246 physicians were reached. Sixty-nine physicians (30%) stated that they used DNAR in practice, and metastatic terminal stage malignancy patients were found to be the most accepted DNAR group. There was a statistically significant difference between physicians' anxiety about physical violence.
ConclusionIn order to increase the quality of CPR, patients should be well analyzed. The applicability of the concept of DNAR in our country is not legally possible. However, this situation does not prevent the emergence of patients who will not benefit from treatment in the clinic. It is best to establish a committee on DNAR and redefine the legal rules within certain norms.
Keywords
Introduction
The purpose of resuscitation is to save life, improve health, relieve pain, decrease comorbidities, and respect the patient’s decisions, rights, and privacy.1 Additionally, regarding cardiopulmonary resuscitation (CPR), the very important aim is to prevent death.2 Although the general rule is that the urgent treatment for cardiac arrest, there are several occasions where not performing CPR is more convenient. In a study, it is shown that 54.9% of patients would not benefit from CPR.3 CPR should be performed on patients who will benefit the most. Inevitable failure should not be accepted.
Do Not Attempt Resuscitation (DNAR) means do not perform resuscitation. However, in various centers, Allow Natural Death (AND) replaces DNAR.1 DNAR definition should be well understood. Some physicians understand DNAR as just not performing CPR, whereas some advocate not providing any medical support to the patient. Not providing any medical support to the patient is not accepted; neither in our county nor in the whole world. Real DNAR decision only suggests not performing CPR. The next step should be determining the person making the DNAR decision. DNAR decision should be taken when the patient is having a cardiac arrest and needing CPR. This decision is too important to be made by a single person. In our country, at CPR, performing, ending, and resuscitating, usually health givers are managing the relations between the families, showing a paternalist approach. This paternalist approach is seriously criticized in developed countries and is slowly replaced with ethical attitudes involving the patient and his/her relatives.2 CPR decision should be made not just in arrest occasions but also regarding the underlying disease and the patient’s personal evaluation and current situation. Another important issue is the variations in health givers’ religious beliefs, occupations, ethnic features, and social status.3 In order to maintain a standard management, clinicians, medical ethic specialists, forensic medicine specialists, lawyers, sociologists, religion experts, and representatives of all different cultural groups should be involved to make a concrete decision.4
Since the DNAR term is not legitimately accepted in our country, it is not performed. However, this does not change the number of patients who will not benefit from CPR performance. The ‘slow codes’ (showing inefficient resuscitative efforts initially) occurring in such occasions are not an appropriate method.1 This application is a moral burden for the decision maker. It results in ethical bias among health givers, misinterpretation, and damages the doctor-patient relationship.1 Additionally, it also raises the CPR incidence of the country and decreases the successful CPR rate.5 DNAR is being fiercely debated around the world, and it is not generally discussed in our country, yet.
Our aim in this study is to evaluate the role of DNAR in emergency departments and to determine the practicability of DNAR terms.
Materials and Methods
Our study is a cross-sectional survey study. The survey questions are prepared by the researchers and distributed to the participants via e-mail. The participants are informed about the thesis study, and data are collected via e-mail. Questions are focused on the attitudes of physicians for DNAR definition, application of DNAR, and the reasons for application. There are questions regarding the responding physicians' DNAR experiences. The identity information of participants is not collected while completing the survey forms. All the emergency specialists who have answered the survey are involved in the study. Those who voluntarily left the answer unfinished and those who entered incomplete data were excluded from the study.
Ethical ApprovalThis study was approved by the Ethics Committee of Izmir Katip Çelebi University Non-Interventional Research Ethics Committee (Date: 26.04.2013, Decision No:113).
Statistical AnalysisSPSS for Windows 21.0 is used for statistical analysis of the data. Average and standard variation for numeric variants; number and percentage for categorical variants are given as definitive statistics. Chi-Square and Fisher’s Exact test for intergroup comparisons for categorical data are used. Since the distributions were not normal (Kolmogorov-Smirnov p<0.05) in numerical variations, intergroup comparisons are done via Mann-Whitney U for two groups, and Kruskal-Wallis H for more than 2 groups are used for statistical analysis. Results are accepted as statistically significant if p<0.05 in 95% confidence interval.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
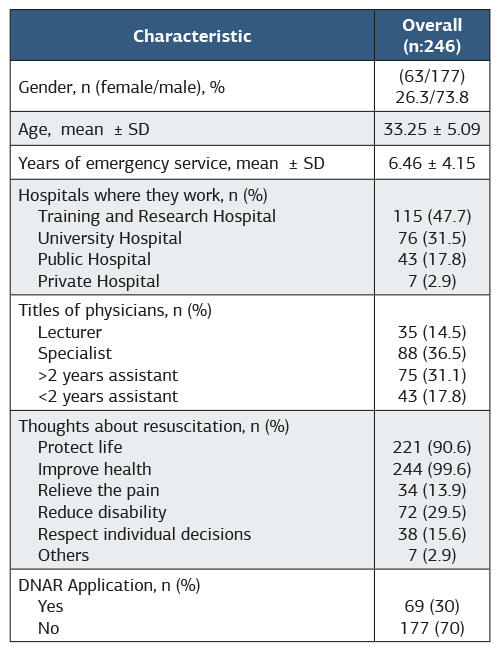
A total of 246 emergency specialists and trainees were included in the study. The average age of the group was 33,25 ± 5,09. The demographic features of the participants are shown in Table 1.
Among participants, 69 (30%) mentioned that they use DNAR in practice, and 65 (26.5%) think that the DNAR decision should be made by the physician. 78 participants (31.7%) mentioned that they understand not performing CPR as DNAR due to the inefficiency principle. Metastatic terminal stage malignancy patients are found to be the most DNAR patients (n = 187; 76.3%). DNAR decision-making compared among the titles of physicians, emergency specialists are the most physicians making this decision (p<0.05).
One hundred and fifty-one physicians (59.2%) mentioned that they did not receive a DNAR request from the patients’ relatives. When DNAR requests of the patient or his/her relatives are compared with those of the medical center, there is no statistically significant difference among groups. However, this request is found the highest in private hospitals. As the relationship between the title of the physician and the DNAR request rate was compared, the academic-titled physicians were found to be the most requested group, which is statistically significant (p<0.05). Only 12 physicians (11.4%) officially recorded a DNAR request. 84 physicians (36.1%) mentioned that DNAR application in the emergency department will be safe if this procedure is confirmed by law. This rate is found to be higher in the female group (n = 30; 51.7%).
It is not statistically significant among groups that share and do not share their DNAR decision-making with the relatives of the patients. Most of the reservations about not sharing DNAR decisions with patients’ relatives are found to be the legal uncertainty, which is statistically higher than other causes (p<0.05). When comparing the DNAR decision with the relatives and the physician’s working place, physical violence is found to be statistically significant (p<0.05). This ratio is found most in research and training hospitals (70.[60.9%]) and least in private hospitals (2.[28.6%]). When the titles of the physicians and not sharing DNAR decision are compared, the disturbance of physical violence is found least in academic titled physicians (11.[31.4%]) and most in trainees (26.[60.5%]) lasting more than 2 years. The relationship between reservation for not sharing DNAR decision with relatives and the working years in the emergency department is analyzed, and psychological, physical, and verbal violence and other causes did show a statistical significance (p<0.05). Psychological, physical and verbal violence is determined as a risk among physicians working less than 10 years in the emergency service. Violence rates among physicians working in emergency departments for more than ten years were found to be lower compared to other groups. Although a statistically significant difference for reservations due to legal mistrust is not observed, it is found to be lower in physicians working more than 10 years in emergency service.
Discussion
We have two main conclusions in our study. Especially DNAR being illegal in our country constrains the entire steps towards its application. Second, DNAR still stands as a responsibility fully taken by the physicians, which they cannot explain in all terms.
AHA guidelines suggest that if not eligible, health givers should not be forced to perform CPR.5 Patients and their relatives have the right to speak about the DNAR decision in Switzerland. In Europe and in our country, the paternalist approach, which externalizes patients/relatives, is still in use. Yang et al. have shown that physicians believe they are the only authority in DNAR decisions.6 Park et al. suggest nurses should be involved in DNAR decision while communicating with the health givers and patients/relatives.7 30% of our participants mentioned that they are actively applying DNAR, while 26% think that the decision is the physician’s responsibility. This points out that only 4% of the physicians think that patients/relatives should be included in decision making. Most of the physicians who are not willing to take full responsibility for self-made DNAR decisions are still performing CPR, although they know the patient will not benefit from it. Nevertheless, another study shows that inadequate knowledge about DNAR keeps physicians from this application.8 In the study of McIntosh et al, patients’, relatives’, and physicians’ awareness was raised with simple efforts, and they have made it.9 We did not make a query about DNAR education, which is a limitation of our study. As a traditional society with most of its citizens belonging to the Muslim religion, accompanied by a low sociocultural level, we believe these factors lack DNAR decision in our country. Religion is one of the most significant aspects for DNAR decision-making process. Most Muslims, with faith in God’s healing power and hope, prefer CPR, neglecting the prognosis of the underlying disease.10 With this background and the DNAR term being currently illegal, it seems impossible to debate about DNAR with relatives in our country. Initially, a well-organized study should be maintained, and then a legal basis should be prepared. Afterwards, the ideal way of language should be determined for community norms to share DNAR with patients/relatives.
The most important determinants in DNAR decision are found to be prognosis of the disease and expected quality of life.11 The most DNAR requests belong to malignant tumors, dementia, cerebrovascular disease sequels.12 Compatible with literature, in our study, “metastatic terminal stage malignancy patients”, elderly patients with multiple comorbid diseases, and patients with concrete evidence for irreversible death were found to have a tendency for DNAR. This result shows that our physicians still accept CPR as a treatment and are aware of the fact that it should not be performed on those who will not benefit from it. Regardless of the underlying disease prognosis, if the patient requests CPR, it should definitely beperformed. Whoever decides to limit or end life support to a patient should preserve the principles of providing necessary health care and not initiate or end unnecessary acts. Compatible with literature, the most important factor influencing DNAR decision is found to be the inexpediency principle. As the experience of the physician decreases, DNAR acceptance increases. Academically titled physicians might trust themselves more due to their experience and knowledge, or might be more cautious about malpractice incidence. As the training experience decreases due to long hours of work, it might diminish the physician’s time and energy and, they might give up more easily.
In the study of Bedell et al, it is shown that only in 19% of patients who had received CPR had discussed it with their physician, and in 33%, the family was consulted.13 Similarly, DNAR decision was shared with 77-86% with the relatives; only 14-22% was discussed with the patient.14 Murphey et al showed in their study that 41% of elders wanted CPR performance. 22% of the patients whose discharge or survival rates were determined as 10-17% accepted CPR performance after being fully informed about DNAR. When discharge or survival rates dropped to 0-5%, CPR performance requirement decreased to 5%.15 As a community, our country is not prepared for the DNAR condition. Our DNAR rate is found 40.1%. The cause of this might be related to the cultural background of the population or beliefs against DNAR. However, if the necessary acknowledgement is ensured precisely, we believe this ratio will rise in our country. This seems possible only with obligatory legal regulations. In a study, a special training is needed for DNAR elucidating because DNAR can be easily misunderstood by the patient/relatives and usually understood as euthanasia.8 DNAR request ratios are found to be higher compared to other centers. We believe that this finding is not conclusive due to the lack of an adequate number of physicians. Physicians working more than 2 years have a higher number of CPR performances, and so these physicians are more in dialogue with patients/relatives in their team leader roles. This may explain the higher rates of DNAR demand from relatives.
Legal obligations for DNAR are not fully determined in our country.16 In a couple of protocols signed with other countries entitle patients with right the of DNAR, whereas in some other protocols, the patient him/herself is not permitted to end his/her life.17 There are a lot of similar situations. The best step towards bias is to work on only the DNAR term, and concrete legal obligations should be gathered. Currently, DNAR performance and euthanasia are illegal and are punished as “first degree murder” (defined in law number 181, clause 43) in Türkiye. For this reason, the CPR rate is high, but the success rate is low in Türkiye. There is no national statistical data in our country.5 In most countries, DNAR orders are legally applicable. In our study, legal limitation is found to be the most determinant factor both for DNAR decision making and sharing this decision with the patient’s relatives. Nevertheless, this causes physicians to secure their DNAR decision from the relatives, and so relatives cannot have the right to object or agree to the DNAR decision. In the field, slow codes, which called ‘cosmetic CPR’, are preferred as DNAR. In our study, we had physicians who mentioned DNAR decision making, but these decisions did not reflect in the records. Knowing inefficient CPR but still continuing to perform CPR is a very big moral burden for physicians. This situation causes moral burdens to all CPR team and results in team trust.
Recently, it has been observed that DNAR decisions are more shared with patients/relatives in Europe.18 In our study, the acknowledgement rate of the relatives is found to be very low. This tendency may result in neglect of patient rights and patient respect. Probably, honor and respect are the last but most important wishes of a patient in the last moments.19 However, in countries like ours, where DNAR is illegal, DNAR decisions are made without official recording and without informing the patients/relatives.20 The two major limitations of DNAR decision making seem to be legal problems and violence risks that physicians face in emergency departments. These occasions are observed in government hospitals and education-training hospitals, which are found to be statistically significant. This finding may be explained as follows: 1. The sociocultural levels of patients admitting to government hospitals are relatively low and 2. The number of patients is much higher compared to university hospitals. In a country where physicians are getting killed by patient relatives, the insecurity of the physician for sharing DNAR decision is understandable. In a country where DNAR is not discussed due to religious beliefs, doctors killed by patient’s relatives are a major hypocrisy. The increasing number of malpractice cases also results in legal insecurity.
Limitations
The study was conducted on a voluntary basis. Only physicians who volunteered to participate in the study answered the survey questions.
Conclusion
As a result; patients should be analyzed carefully and CPR should be performed to those who will benefit the most. CPR should be directed regarding the experiences obtained from previous unsuccessful attempts. In this case, DNAR term is occurring; for DNAR decision legal confidence should be guaranteed to physicians. In our country, with current legal status, DNAR cannot be performed. DNAR is trialed equal to ‘first degree murder’. However this situation does not prohibit patients that will not benefit from medical support. In situations where the patient is assumed to die eventually, using total effort result both financial and time loss. Additionally utilizing all the resources to patients that will definitely not benefit may also result in reduced time and effort for those who may actually benefit. DNAR should be handled by a committee that should define the norms and legal aspects should be renewed. Necessary steps should be taken immediately; otherwise, physicians will continue to perform ineffective CPR with a huge moral burden and the rate of unsuccessful CPR will increase.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
The study was conducted in accordance with the Declaration of Helsinki and its later amendments.
Informed Consent
Informed consent was obtained from all participants prior to participation in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.S., P.H.K., E.E.Ü.
Methodology: A.S., E.E.Ü.
Data Curation: A.S.
Formal Analysis: P.H.K.
Investigation: A.S., P.H.K.
Writing – Original Draft Preparation: A.S.
Writing – Review & Editing: P.H.K., E.E.Ü.
Supervision: E.E.Ü.
Abbreviations
AAHA: American Heart Association
AND: Allow natural death
CPR: Cardiopulmonary resuscitation
DNAR: Do not attempt resuscitation
ED: Emergency department
SPSS: Statistical Package for the Social Sciences
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
References
-
Sasson C, Rogers MAM, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3(1):63-81. doi:10.1161/circoutcomes.109.889576
-
Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46-e215. doi:10.1161/circulationaha.109.192667
-
Pynn M, Morgan E, Gibson B, Benjamin A. More discussions needed about resuscitation? DNAR orders in a district general hospital. Clin Med (Lond). 2016;16(suppl 3):S13. doi:10.7861/clinmedicine.16-3-s13
-
Fan SY, Wang YW, Lin IM. Allow natural death versus do-not-resuscitate: titles, information contents, outcomes, and the considerations related to do-not-resuscitate decision. BMC Palliat Care. 2018;17(1):114. doi:10.1186/s12904-018-0367-4
-
American Heart Association. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 2: ethical issues. Circulation. 2005;112(24 suppl):IV1-IV203. doi:10.1542/peds.2006-0349
-
Yang GM, Kwee AK, Krishna L. Should patients and family be involved in “do not resuscitate” decisions? Views of oncology and palliative care doctors and nurses. Indian J Palliat Care. 2012;18(1):52-58. doi:10.4103/0973-1075.97474
-
Park YR, Kim JA, Kim K. Changes in how ICU nurses perceive the DNR decision and their nursing activity after implementing it. Nurs Ethics. 2011;18(6):802-813. doi:10.1177/0969733011410093
-
Hurst SA, Becerra M, Perrier A, et al. Including patients in resuscitation decisions in Switzerland: from doing more to doing better. J Med Ethics. 2013;39(3):158-165. doi:10.1136/medethics-2012-100699
-
McIntosh R, Webb H, Hartley M, Brooks M. Raising the issue of DNAR orders in vascular surgery patients. BMJ Qual Improv Rep. 2016;5(1):u206293.w3610. doi:10.1136/bmjquality.u206293.w3610
-
Alrimawi I, Abdelkader R, Saifan AR, Batiha AM. Palestinian community perceptions of do-not-resuscitate orders for terminally ill patients. J Clin Nurs. 2018;27(13-14):2719-2728. doi:10.1111/jocn.13905
-
Nakagawa Y, Inokuchi S, Kobayashi N, Ohkubo Y. Do not attempt resuscitation order in Japan. Acute Med Surg. 2017;4(3):286-292. doi:10.1002/ams2.271
-
O’Brien H, Scarlett S, Brady A, et al. Do-not-attempt-resuscitation (DNAR) orders: understanding and interpretation of their use in the hospitalised patient in Ireland. J Med Ethics. 2018;44(3):201-203. doi:10.1136/medethics-2016-103986
-
Bedell SE, Pelle D, Maher PL, Cleary PD. Do-not-resuscitate orders for critically ill patients in the hospital: how are they used and what is their impact? JAMA. 1986;256(2):233-237. doi:10.1001/jama.1986.03380020095030
-
Heyland DK, Cook DJ, Rocker GM, et al. Defining priorities for improving end-of-life care in Canada. CMAJ. 2010;182(16):E747-E752. doi:10.1503/cmaj.100131
-
Mockford C, Fritz Z, George R, et al. Do not attempt cardiopulmonary resuscitation (DNACPR) orders: a systematic review of the barriers and facilitators of decision-making and implementation. Resuscitation. 2015;88:99-113. doi:10.1016/j.resuscitation.2014.11.016
-
Murphy DJ, Burrows D, Santilli S, et al. CPR preferences and survival probability. N Engl J Med. 1994;330(8):545-549.
-
Michalowski S, Martin W. DNACPR decisions: aligning law, guidance and practice. Med Law Rev. 2022;30(3):434-456. doi:10.1093/medlaw/fwac007
-
Moon JY, Kim JO. Ethics in the intensive care unit. Tuberc Respir Dis (Seoul). 2015;78(3):175-179. doi:10.4046/trd.2015.78.3.175
-
Chochinov HM, Hack T, McClement S, et al. Dignity-conserving care—a new model for palliative care: helping the patient feel valued. JAMA. 2002;287(17):2253-2260. doi:10.1001/jama.287.17.2253
-
Downar J, Hawryluck L. What should we say when discussing “code status” and life support with a patient? A Delphi analysis. J Palliat Med. 2010;13(2):185-195. doi:10.1089/jpm.2009.0269
Tables
Table 1. The demographic features of the participants
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Conference Presentation
This study was presented as an oral presentation in International İzmir Democracy University Medical Congress, Izmir, Türkiye, 2019
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Aslı Şener, Pınar Hanife Kara, Erden Erol Ünlüer. Applicability of do-not-attempt-resuscitation in the emergency department. Ann Clin Anal Med 2026;17(6):533-537. doi:10.4328/ACAM.22387
- Received:
- August 27, 2024
- Accepted:
- June 2, 2025
- Published Online:
- June 17, 2025
- Printed:
- June 1, 2026