
The effects of lower uterine segment involvement on angiolymphatic invasion, tumor grade, and staging in patients with early-stage endometroid type endometrial cancer
Predictivity of lower uterine segment tumor
Authors
Abstract
AimEndometrial cancer (EC) is the most common malignancy of the female reproductive system in developed countries. EC is surgically staged. EC’s most important prognostic factors are stage, grade, lymphovascular space involvement (LVSI), and histologic subtype. We designed this study to determine the predictive value of lower uterine segment involvement (LUSI) in terms of angiolymphatic invasion, tumor grade, and lymph node involvement in patients with early-stage endometrioid type endometrial cancer (EEC).
MethodsThe study was performed as a retrospective clinical study in patients with stages 1A and 1B (FIGO 1988) who were operated for EEC (total abdominal hysterectomy + bilateral salpingo-oophorectomy (TAH+BSO) ± lymph node dissection) in the Gynecologic Oncology Clinic of Gazi University Hospital.
ResultsOf the 98 patients in the study group, 53 (54.1%) had LUSI, while in the remaining 45 cases (45.9%), LUSI was negative. A statistically significant difference was found between LUSI and pelvic lymph node metastasis (p=0.049). There was a statistically significant difference between LUSI and depth of myometrial invasion (MI) (p=0.03). There was also a statistically significant difference between tumor diameter size and LUSI (p=0.001). However, LUSI was not substantial for other prognostic factors such as LVSI, tumor grade, and age.
ConclusionWe showed that lower uterine segment involvement is important for myometrial invasion and pelvic lymph node metastasis and may determine the extent of surgery.
Keywords
Introduction
Endometrial cancer is the most common malignancy of the female reproductive system in developed countries. It is the fourth most common cancer in women after breast, lung, and colorectal cancer.1 The lifetime risk of developing EC is 2.6%, and the average age of onset is 62 years.2 Approximately 80% of endometrial cancers diagnosed in developed countries are endometrioid type.3 Prognosis, recurrence, and survival mainly depend on the surgical stage of the tumor. There are many risk factors for the development of EC, the majority being unmet estrogen and its causes. These include endometrial hyperplasia, polycystic ovary syndrome, obesity, nulliparity, infertility, history of infertility treatment, early menarche-late menopause, and prolonged estrogen exposure such as the use of estrogen therapy without progesterone at menopause. Medical conditions such as diabetes, hypertension, and hypothyroidism have also been shown to be associated with endometrial cancer. Conditions that decrease estrogen exposure or increase progesterone levels (such as oral contraceptives or smoking) have a protective effect.4
The main complaint in 90% of endometrial cancer patients is abnormal vaginal bleeding, most commonly postmenopausal bleeding. Intermenstrual bleeding or prolonged heavy bleeding in perimenopausal and anovulatory premenopausal patients should also be suspected. Endocervical curettage and endometrial biopsy should be performed in all patients with suspected endometrial cancer. Planning for definitive treatment is done in case of a positive endometrial biopsy. Stage, grade, lymphovascular area involvement, and histologic subtype are the most important prognostic factors in endometrial cancer. 70-80% of patients with endometrial cancer are stage 1 at the time of diagnosis. Stage 3 and stage 4 cancer are less common. The 5-year survival in stage 1 endometrial cancer is over 90%.5 The first approach in the treatment of endometrial cancer is surgery. The surgical approach is total abdominal hysterectomy and bilateral salpingo-oophorectomy in the early stage, bilateral pelvic paraaortic lymphadenectomy and omentectomy in selected cases, and debulking in the advanced stage.5 The therapeutic usefulness of systematic pelvic and paraaortic lymphadenectomy is controversial.5
Lymphatic drainage of the uterus occurs in the pelvic lymph nodes, inguinal region, and paraaortic lymph nodes via the infundibulopelvic ligament. The frequency of lymph node metastasis in endometrial cancer varies between 7.7-21%. Of this rate, 3.3-12% is pelvic lymph node metastasis only, 2.5-8.8% is both pelvic and paraaortic metastasis, and 0.7-2% is paraaortic metastasis only. As pelvic lymph node involvement increases, paraaortic lymph node involvement also increases.6,7,8
Endometrial carcinoma originates from the uterine corpus and fundus, but lower uterine segment involvement (LUSI) is observed in 3-6% of cases.9 Tumors originating from the lower uterine segment (LUS) are located between the uterine corpus and cervix and show histologic features of both. Therefore, they sometimes complicate the differential diagnosis of uterine corpus and cervical adenocarcinomas when the primary tumor needs to be identified for further investigation and prognosis.10 Tumors arising from or involving the LUS also differ from tumors of the uterine corpus by their thin mucosal and myometrial layers and poor hormonal response to estrogen.11
In some reports, LUS carcinoma does not have the characteristics of type I endometrial cancer. It tends to show characteristics of type II, thought to be due to the thin endometrial layer of the LUS and a weak endometrial response to estrogen.12 Clinically, type I cases are characterized by irregular menstruation, unmet estrogen, nulliparity, infertility, and a high frequency of PCOS (polycystic ovary syndrome). In contrast, type II cases show weak estrogen and progesterone receptors and p53 mutation expression and have similar features to LUS carcinoma.13,14,15,16,17
The endometrial layer of LUS carcinoma is similar to the endometrium in cell distribution and histochemistry, but the volume of the endometrium tends to be smaller in LUS.18 Because the endocervical mucosa histologically transitions gradually to the LUS endometrium, endocervical and endometrial epithelial features show combinations in LUS. Because cases of endometrial cancer originating from the LUS are rare, few studies have compared the characteristics of LUS tumors with tumors originating from the uterine corpus. There are conflicting reports on the effect of LUS involvement as a prognostic factor in endometrial cancer.
In this study, we aimed to investigate the effects of uterine lower segment involvement on lymph node involvement, myometrial invasion, angiolymphatic invasion, and staging in patients with early-stage endometrioid-type endometrial cancer.
Materials and Methods
In cases operated for early-stage endometrioid type endometrial cancer, the predictive value of uterine lower segment involvement on lymph node involvement, myometrial invasion, angiolymphatic invasion, and staging was evaluated. Patients with histologic types other than endometrioid type endometrial cancer (serous, clear cell, undifferentiated, etc.), patients with advanced endometrial cancer, and patients who would not provide reliable data due to incomplete information were not included in the study. All patients who participated in the study were patients who underwent endometrial sampling due to perimenopausal or postmenopausal bleeding preoperatively and were diagnosed with endometrioid type endometrial cancer by pathology. TAH+BSO, bilateral pelvic lymph node dissection and ± paraaortic lymph node dissection were performed. The degree of myometrial invasion, tumor diameter size, histological grade, and cervical metastasis were evaluated by a frozen section of the hysterectomy slice. While only pelvic lymph node dissection was performed in patients with good prognostic data, total pelvic and paraaortic lymph node dissection was performed in the poor prognostic group with grade 3 tumor, myometrial invasion depth >1/2, tumor diameter >2cm, isthmus-cervix invasion, extrauterine disease (abdominal metastasis) invasion. Dissection was performed up to the renal vein level in surgically suitable cases. All materials were analyzed in our hospital’s pathology laboratory. FIGO surgical staging system was used for endometrial cancer staging. FIGO was used for grade classification, and the World Health Organization Classification of Tumors system was used for histological classification. Age, date of operation, type of operation, histological type of tumor, grade of tumor, diameter of tumor, percentage of tumor invasion into myometrium, stage of disease, number/location of lymph nodes removed, number/location of metastatic lymph nodes removed, presence of lymphovascular invasion, LUSI and surgical stage were evaluated. In patients with LUSI, the depth of uterine myometrial invasion and tumor diameter, grade, and LVSI were evaluated to determine whether they were predictive values for lymph node involvement.
Ethical ApprovalThis study was approved by the Ethics Committee of Gazi University Hospital (Date: 24.04.2017, Decision No: 185).
Statistical AnalysisThe research data were evaluated using the SPSS 17.0 statistical package program. Descriptive statistics were presented as mean, median (min; max), frequency distribution, and percentage. Pearson Chi-Square, Yates Corrected Chi-Square Test, and Fisher’s Test were used as statistical methods. The statistical significance value was accepted as p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
A total of 98 patients were included in the study. Patients underwent TAH+BSO, bilateral pelvic lymph node dissection, ± paraaortic lymph node dissection. The mean age of the patients in the study group was 61.2 ( ± 9.3) years. The final pathology of all patients was endometroid-type adenocarcinoma. 12(12.2%) patients were grade 1, 65(66.3%) were grade 2, and 21(21.4%) were grade 3. After postoperative histopathologic evaluation, 17(17.3%) patients were stage 1A, 65(66.3%) were stage 1B, 7(7.1%) were stage 3C1, and 8(8.2%) were stage 3C2. The depth of myometrial invasion was below ½ in 42(42.9%) patients and above ½ in 56(57.1%) patients. Tumor diameter size was below 4 cm in 43(43.9%) patients and above 4 cm in 55(56.1%) patients. LVSI was positive in 25(25.5%) and negative in 72(73.5%) patients. Of the 98 patients in the study group, 53(54.1%) had LUS involvement, and 45(45.9%) had no LUSI. Of the 98 patients in the study group, 7 patients underwent only hysterectomy and salpingo-oophorectomy operation due to co-morbid diseases. The mean age of the patients with LUSI was 60.5( ± 9.19), while the mean age of the patients without LUSI was 62.0( ± 9.45). Pelvic lymph node dissection was performed in 20 of 52 patients with LUSI, while pelvic paraaortic lymph node dissection was performed in 32 patients. Of 39 stage 1B patients without LUSI, 12 patients underwent hysterectomy + pelvic lymph node dissection, while 27 patients underwent pelvic + paraaortic lymph node dissection. Lymph node metastasis was detected in 11 patients with LUSI, while pelvic and paraaortic lymph node involvement was detected in 4 patients without LUSI (Table 1). No patients without myometrial involvement were among the 98 patients who participated in the study. A statistically significant difference was found between LUSI and MI depth (p=0.03). A statistically significant difference was also between LUSI and tumor diameter size (p=0.001). A statistically significant difference was found between LUSI and pelvic lymph node metastasis (p=0.049). There was no statistically significant difference between LUSI, tumor grade, and LVSI (p=0.392 and p=0.852, respectively).
Discussion
Endometrial cancer is the most common gynecologic cancer in women in developed countries. Currently, most patients with endometrial cancer require surgical staging according to the FIGO staging system. Lymphadenectomy is one of the most controversial issues in endometrial cancer surgery.19 Since lymph node metastasis in endometrial cancer affects the prognosis of the patient, lymphadenectomy has diagnostic value and therapeutic value. LUS is anatomically located between the uterine corpus and cervix and shows histologic features of both of these parts. The main aim of our study is to perform lymph node surgery in patients with tumors located in the LUS only when necessary. In our study, the mean age of the patient group with LUSI was 60.5( ±9.19), while the mean age of the patient group without LUSI was 62.08( ± 9.45). Our study found no significant correlation between age and LUSI (p=0.543).
Brown et al. investigated whether LUSI was associated with the depth of MI and showed that LUSI was a determinant for the depth of myometrial invasion (p=0.02).20 In our study, LUSI was found to be associated with the depth of myometrial invasion (p=0.030). A study by Phelan et al. investigating whether LUSI was associated with tumor grade showed that LUSI was not a determinant of tumor grade (p=0.20).21 Of the 98 patients included in our study, the grade was 1 in 8(15.1%), 2 in 36(67.9%), and 3 in 9(17%) patients (p=0.392). Our study found no significant correlation between tumor grade and LUSI.
In a study by Gemer et al., age, depth of myometrial invasion, tumor grade, depth of myometrial invasion, depth of myometrial invasion lymphovascular area invasion were examined in patients with endometrial cancer with AUS involvement and evaluated whether they had predictive value for LUSI. In a retrospective study of 138 patients, tumor grade (p=0.002), LVAI (p=0.01), and depth of MI (p<0.001) were statistically significant in patients with LUSI.22
In a study by Erkaya et al., depth of MI, tumor grade, tumor diameter, lymph node metastasis, depth of myometrial invasion, and lymphovascular area invasion were examined in patients with endometrial cancer who had LUSI and evaluated whether they had predictive value for LUSI. In a retrospective study of 139 patients, tumor grade (p<0.0001), LVAI (p<0.001), depth of MI (p<0.001), and tumor diameter (p=0.01) showed a significant correlation in terms of LUSI. They also found that the risk of pelvic and paraaortic lymph node involvement increased in patients with AUS involvement, and this relationship was statistically significant (p=0.001 and p=0.005, respectively).23 In our study, LUSI was found to be associated with MI depth, tumor size, and pelvic lymph node involvement, which is consistent with the literature. However, no significant results were found in terms of LVSI and tumor grade. This may be related to the heterogeneity in tumor grade of the 98 patients included in our study. In addition, the effect of LUSI on survival was investigated in this study by Erkaya et al., but no significant difference was found (p>0.05).
A study by Kizer et al. evaluated whether LUSI is a predictive value for tumor grade and LVSI in endometrial cancer patients. In a retrospective study of 481 patients, LVSI was found to be associated with LUSI. It was reported that LUSI was associated with decreased survival.24 In our study, LUSI was not found to be statistically significant for LVSI. This may be due to the need for more cases in the study to evaluate the association with LUSI.
A study by Madom et al. evaluated whether LUSI, MI, and LVSI have a predictive value in terms of lymph nodes in endometrial cancer patients. In a retrospective study of 324 patients, LVSI, LUSI, and MI were found to be predictive of lymph node involvement.25 Of the 97 patients included in our study, 25(25.7%) had LVSI, and 72(74.3%) did not have LVSI. Eight of 25(25.7%) patients with LVSI had lymph node metastasis, while 8 of 72(74.3%) patients without LVSI had lymph node metastasis, and this was statistically significant (p=0.044). Of the 15 patients with lymph node metastases, 7 had LVSI. LVSI was added to the 2023 FIGO Endometrial cancer staging updated last year, and the disease is considered stage 2 when diffuse LVSI is present.
Limitations
The research(thesis study) was presented at the 1st International and 16th National Gynecologic Oncology Congress (November 21st - 25th, 2018) held in Antalya. (Oral Presentation-31).
Conclusion
Understanding the prognostic value of LUSI may be useful in planning the extent of surgery, adjuvant treatment, and survival. Prospective studies with more patients are needed for more meaningful results to have the last word on the subject.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BSO: Bilateral salpingo-oophorectomy
EC: Endometrial cancer
EEC: Endometrioid type endometrial cancer
FIGO: International Federation of Gynecology and Obstetrics
LUS: Lower uterine segment
LUSI: Lower uterine segment involvement
LVSI: Lymphovascular space invasion
MI: Myometrial invasion
TAH: Total abdominal hysterectomy
References
-
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11-30. doi:10.3322/caac.21166
-
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71-96. doi:10.3322/ca.2007.0010
-
Prat J, Gallardo A, Cuatrecasas M, Catasús L. Endometrial carcinoma: pathology and genetics. Pathology. 2007;39(1):72-87. doi:10.1080/00313020601136153
-
Ignatov A, Ortmann O. Endocrine risk factors of endometrial cancer: polycystic ovary syndrome, oral contraceptives, infertility, tamoxifen. Cancers (Basel). 2020;12(7):1766. doi:10.3390/cancers12071766
-
Fujimoto T, Fukuda J, Tanaka T. Role of complete para-aortic lymphadenectomy in endometrial cancer. Curr Opin Obstet Gynecol. 2009;21(1):10-14. doi:10.1097/gco.0b013e32831ac3ac
-
Fujimoto T, Nanjyo H, Nakamura A, et al. Para-aortic lymphadenectomy may improve disease-related survival in patients with multipositive pelvic lymph node stage IIIc endometrial cancer. Gynecol Oncol. 2007;107(2):253-259. doi:10.1016/j.ygyno.2007.06.009
-
McMeekin DS, Lashbrook D, Gold M, et al. Nodal distribution and its significance in FIGO stage IIIc endometrial cancer. Gynecol Oncol. 2001;82(2):375-379. doi:10.1006/gyno.2001.6278
-
Watari H, Todo Y, Takeda M, et al. Lymph-vascular space invasion and number of positive para-aortic node groups predict survival in node-positive patients with endometrial cancer. Gynecol Oncol. 2005;96(3):651-657. doi:10.1016/j.ygyno.2004.11.026
-
Davidesko S, Meirovitz M, Shaco-Levy R, et al. The significance of lower uterine segment involvement in endometrial cancer. Eur J Surg Oncol. 2024;50(3):108007. doi:10.1016/j.ejso.2024.108007
-
Westin SN, Lacour RA, Urbauer DL, et al. Carcinoma of the lower uterine segment: a newly described association with Lynch syndrome. J Clin Oncol. 2008;26(36):5965-5971. doi:10.1200/jco.2008.18.6296
-
Miyoshi A, Kanao S, Naoi H, Otsuka H, Yokoi T. Investigation of the clinical features of lower uterine segment carcinoma: association with advanced stage disease and indication of poorer prognosis. Arch Gynecol Obstet. 2018;297(1):193-198. doi:10.1007/s00404-017-4576-5
-
Hachisuga T, Fukuda K, Iwasaka T, Hirakawa T, Kawarabayashi T, Tsuneyoshi M. Endometrioid adenocarcinomas of the uterine corpus in women younger than 50 years of age can be divided into two distinct clinical and pathologic entities based on anatomic location. Cancer. 2001;92(10):2578-2584. doi:10.1002/1097-0142(20011115)92:103.0.co;2-v
-
Jacques SM, Qureshi F, Ramirez NC, Malviya VK, Lawrence WD. Tumors of the uterine isthmus: clinicopathologic features and immunohistochemical characterization of p53 expression and hormone receptors. Int J Gynecol Pathol. 1997;16(1):38-44. doi:10.1097/00004347-199701000-00007
-
Watanabe Y, Nakajima H, Nozaki K, et al. Clinicopathologic and immunohistochemical features and microsatellite status of endometrial cancer of the uterine isthmus. Int J Gynecol Pathol. 2001;20(4):368-373. doi:10.1097/00004347-200110000-00009
-
Lax SF, Pizer ES, Ronnett BM, Kurman RJ. Clear cell carcinoma of the endometrium is characterized by a distinctive profile of p53, Ki-67, estrogen, and progesterone receptor expression. Hum Pathol. 1998;29(6):551-558. doi:10.1016/s0046-8177(98)80002-6
-
Lax SF, Kendall B, Tashiro H, Slebos RJ, Hedrick L. The frequency of p53, K-ras mutations, and microsatellite instability differs in uterine endometrioid and serous carcinoma: evidence of distinct molecular genetic pathways. Cancer. 2000;88(4):814-824. doi:10.1002/(sici)1097-0142(20000215)88:43.0.co;2-u
-
Jiko K, Tsuda H, Sato S, Hirohashi S. Pathogenetic significance of p53 and c-Ki-ras gene mutations and human papillomavirus DNA integration in adenocarcinoma of the uterine cervix and uterine isthmus. Int J Cancer. 1994;59(5):601-606. doi:10.1002/ijc.2910590505
-
Masuda K, Banno K, Yanokura M, et al. Carcinoma of the lower uterine segment: clinicopathological characteristics and association with Lynch syndrome. Curr Genomics. 2011;12(1):25-29. doi:10.2174/138920211794520169
-
Sehouli J, Camara O, Stengel D, Köhler G, Lichtenegger W; Arbeitsgruppe Endometriumkarzinom der Nord-Ostdeutschen Gesellschaft für Gynäkologische Onkologie e.V. Multizentrische Umfrage zum Stellenwert der Lymphonodektomie beim Endometriumkarzinom in Deutschland [Multi-institutional survey on the value of lymphadenectomy in endometrial carcinoma in Germany]. Gynakol Geburtshilfliche Rundsch. 2003;43(2):104-110. doi:10.1159/000069163
-
Brown AK, Madom L, Moore R, Granai CO, DiSilvestro P. The prognostic significance of lower uterine segment involvement in surgically staged endometrial cancer patients with negative nodes. Gynecol Oncol. 2007;105(1):55-58. doi:10.1016/j.ygyno.2006.10.058
-
Phelan C, Montag AG, Rotmensch J, Waggoner SE, Yamada SD, Mundt AJ. Outcome and management of pathological stage I endometrial carcinoma patients with involvement of the lower uterine segment. Gynecol Oncol. 2001;83(3):513-517. doi:10.1006/gyno.2001.6407
-
Gemer O, Gdalevich M, Voldarsky M, Barak F, Ben Arie A, Schneider D, et al. Lower uterine segment involvement is associated with adverse outcome in patients with stage I endometrioid endometrial cancer: results of a multicenter study. Eur J Surg Oncol. 2009;35(8):865-869. doi:10.1016/j.ejso.2008.10.007
-
Erkaya S, Öz M, Topçu HO, Şirvan AL, Güngör T, Meydanli MM. Is lower uterine segment involvement a prognostic factor in endometrial cancer? Turk J Med Sci. 2017;47(1):300-306. doi:10.3906/sag-1602-137
-
Kizer NT, Gao F, Guntupalli S, et al. Lower uterine segment involvement is associated with poor outcomes in early-stage endometrioid endometrial carcinoma. Ann Surg Oncol. 2011;18(5):1419-1424. doi:10.1245/s10434-010-1454-9
-
Madom LM, Brown AK, Lui F, Moore RG, Granai CO, Disilvestro PA. Lower uterine segment involvement as a predictor for lymph node spread in endometrial carcinoma. Gynecol Oncol. 2007;107(1):75-78. doi:10.1016/j.ygyno.2007.05.026
Tables
Table 1. Comparison of uterine corpus endometrioid tumors with and without LUSI
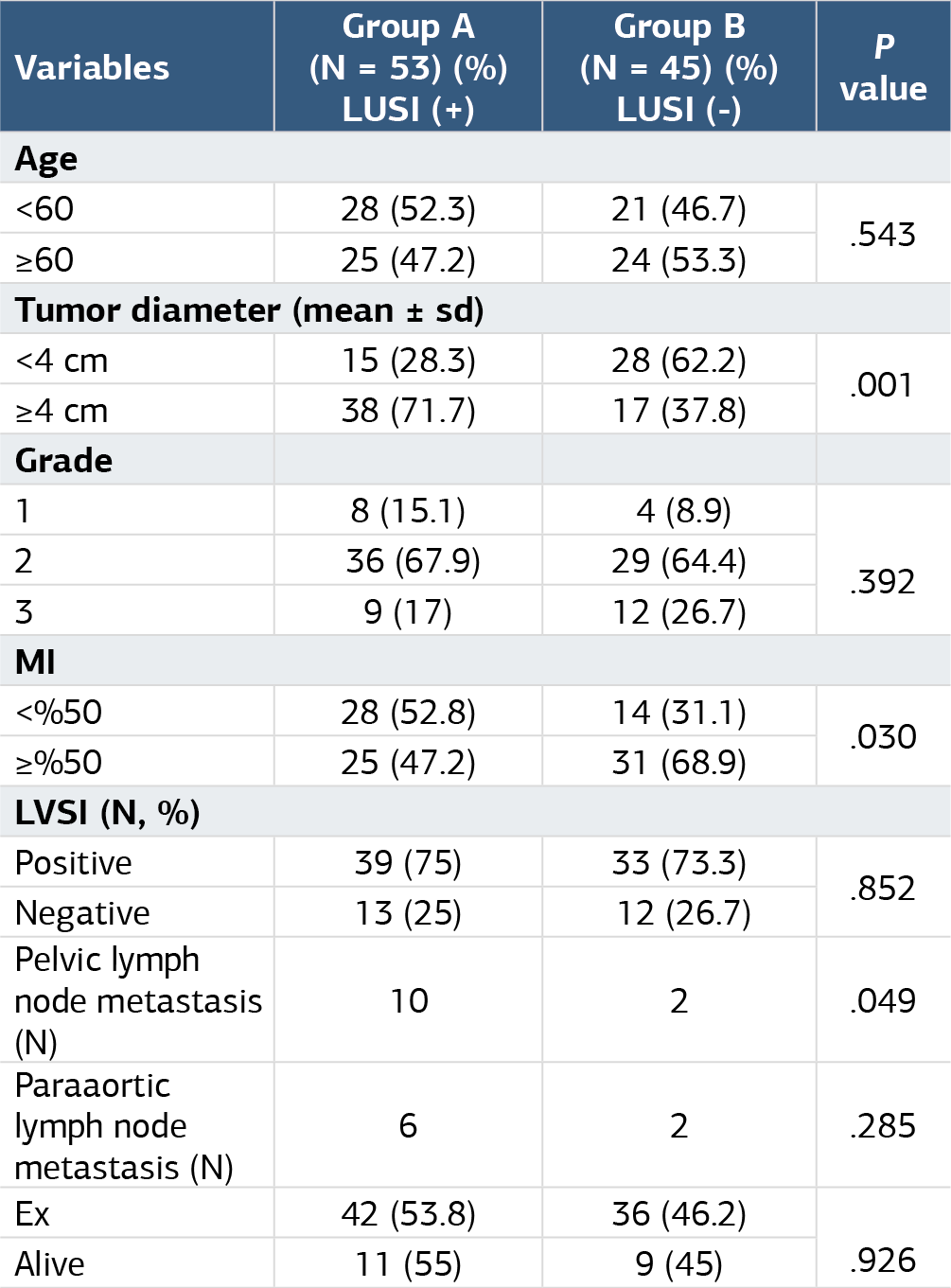
Fisher’s Exact test, Ki-re trend analysis, LUSI: Lower uterine segment involvement, MI: Myometrial invasion, LVSI: Lymphovascular space invasion, N: Number, P: Probability value.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Yağmur Soykan, Asiye Ugras Dikmen, Özlem Erdem, Mehmet Anıl Onan. The effects of lower uterine segment involvement on angiolymphatic invasion, tumor grade, and staging in patients with early-stage endometroid type endometrial cancer. Ann Clin Anal Med 2025;16(4):276-280. doi:10.4328/ACAM.22389
- Received:
- August 28, 2024
- Accepted:
- October 21, 2024
- Published Online:
- November 9, 2024
- Printed:
- April 1, 2025