
Hypomagnesemia in pediatric intensive care unit: etiology, risk factors and relationship of mortality
Hypomagnesemia in neonatology
Authors
Abstract
AimWe aimed to identify the etiology, risk factors, frequency, and mortality associated with hypomagnesemia in hospitalized patients in the pediatric intensive care unit (PICU) and to contribute to reducing mortality by addressing hypomagnesemia in these patients.
MethodsIn this study, the files of patients admitted to the Şahinbey Research and Practice Hospital PICU between January 2014 and August 2016 were retrospectively reviewed. Age, gender, diagnosis, underlying diseases, postoperative status, Pediatric Mortality Index, and Pediatric Mortality Risk Scores were recorded. The definition of hypomagnesemia is defined as the serum magnesium level below 1.7 mg / dL (0.7 mmol / L).
ResultsThe clinical features of the patients are as follows: A total of 229 cases were included, with a mean age of 57.29 months (range: 1-191 months). Of these, 118 (51.5%) were male, and 111 (48.5%) were female. Hypomagnesemia was present in 44 cases (19.2%) at the time of admission, and it developed in 162 cases (7.7%) during hospitalization. In 65 patients (28.4%), hypomagnesemia was not observed either before or during hospitalization. The average duration of hospitalization was 17.3 ± 21.9 days in patients with hypomagnesemia and 10.7 ± 22.8 days in those without hypomagnesemia (p=0.001). The mortality rate was 37.3% in the group with normal magnesium levels, 45.5% in patients with hypomagnesemia at admission, and 47.5% in patients who developed hypomagnesemia during hospitalization. Among the patients who developed hypomagnesemia during hospitalization, 81.5% had hypoalbuminemia, 30.9% had hypophosphatemia, and 35.5% had hypokalemia (p=0.001).
ConclusionHypomagnesemia is common in the PICU, and patients with hypomagnesemia tend to have a longer hospital stay, higher mortality rates, a greater need for mechanical ventilation, and are often accompanied by electrolyte disturbances. Magnesium levels should be closely monitored in the PICU. Larger prospective studies are needed to evaluate hypomagnesemia and its associated factors in pediatric intensive care units.
Keywords
Introduction
Magnesium (Mg) is the fourth most abundant essential element in the body and the second most abundant in the intracellular area. Magnesium, the main intracellular metal cation, plays an important role in basic cellular reactions. Magnesium acts as a cofactor for more than three hundred enzymes that contain ATP. It also plays a role in DNA transcription, neuromuscular stability, and protein synthesis.1
Magnesium deficiency causes potassium (K+) to flow out of the cell and induce depolarization, leading to cardiac arrhythmias. In Mg disorders, sodium (Na+) can change the K+ gradient and transmembrane potentials, resulting in neuromuscular excitability or irritability. In Mg deficiency, an increase in the levels of IL-1, TNFα, IFN-γ, substance P and CGRP (Calcitonin gene-related peptide) is observed among the cytokines circulating in the plasma.2,3,4,5
Hypomagnesemia has been reported in 2% of the general population, 10-20% of hospitalized patients, and 50-60% of intensive care patients.1,4 Mg levels at the time of admission to the intensive care unit (ICU) have been shown to be associated with mortality. Hypomagnesemia is often reported to be accompanied by electrolyte disturbances.6,7 Magnesium is used in pulmonary hypertension, neuromuscular hyperexcitability, bronchospasm, cardiac arrhythmia and neuroprotective treatment.1,3,6 Despite this, there are no sufficient studies on pediatric intensive care patients.
In our study, we aimed to determine the etiology, risk factors, frequency, and morbidity and mortality relationship of hypomagnesemia in pediatric intensive care unit (PICU) patients.
Materials and Methods
The study was conducted on patients hospitalized in the PICU of the Department of Child Health and Diseases of the Faculty of Medicine of Gaziantep University between January 2014 and August 2016. Data were collected by retrospective file scanning after the approval of the ethics committee. The study form recorded the gender of the patients, underlying disease, current disease, whether they were postoperative, length of stay, whether they were connected to a mechanical ventilator, whether they received inotropes, whether they received renal replacement therapy, whether they received plasmapheresis, the Mg+2 value during admission to the PICU, the etiology of hypomagnesemia if any, the Mg+2 value and etiology if hypomagnesemia developed during admission, the corrected Ca+2, phosphorus, albumin, Na+ and K+ values at the time of hypomagnesemia. Pediatric mortality index, Pediatric mortality risk scores and outcome were recorded.
Hypomagnesemia was defined as a serum magnesium level below 1.8 mg/dl (0.7 mmol/L). The inclusion criteria for the study were being between 1 month and 18 years old, having been in intensive care between January 2014 and August 2016, and having sufficient data entered. The exclusion criteria from the study were not having sufficient data collection and not being between 1 month and 18 years old.
The patients were divided into three groups. Group 1: Those with hypomagnesemia at the time of admission and the etiology, if any, was recorded. Group 2: Patients without hypomagnesemia at the time of admission but with hypomagnesemia during admission were considered to have acquired hypomagnesemia and serum Mg level, etiology of hypomagnesemia and the day of admission were recorded. Group 3: Those without hypomagnesemia at and during admission were recorded.
Ethical ApprovalThis study was approved by the Ethics Committee of Gaziantep University (Date: 14.11.2014, Decision No: 2016/301).
Statistical AnalysisSPSS for Windows version 22.0 package program was used for statistical analyses and p<0.05 was considered statistically significant. Shapiro Wilk test was used to control the conformity of continuous variables to normal distribution. Mann Whitney U Test was used to compare 2 independent groups for variables that did not have normal distribution. Relationships between categorical variables were tested with Chi-square analysis.
Reporting GuidelinesThis study was prepared in accordance with the STROBE guideline.
Results
Demographic and clinical characteristics of the cases are shown in Table 1. The frequency distribution of the cases in terms of primary pathologies was as follows; 18 (7.8%) were related to the respiratory system, 44 (19.2%) to the cardiovascular system, 40 (17.4%) to the renal system, 6 (2.6%) to the gastrointestinal system, 36 (15.7%) to the neurological system, 11 (4.8%) to the endocrine system, 15 (6.6%) to hematology, 32 (14%) to malignancy and solid tumors, 5 (2.2%) after surgery, and 22 (9.6%) to other causes (burn, drowning, drug intoxication, insect bites).
The frequency distribution of cases in terms of hospitalization was as follows: respiratory failure in 82 patients (35.8%), heart failure in 31 patients (13.5%), renal failure in 24 patients (10.5%), CNS failure in 16 patients (7%), sepsis in 35 patients (15.3%), liver failure in 3 patients (1.3%), hematological failure in 16 patients (34 patients (6.9%), multiple organ failure in 6 patients (2.6%), and postoperative follow-up in 12 patients (5.3%).
In terms of risk factors in patients with hypomagnesemia at PICU admission, malnutrition was detected in 17 cases (38%), bowel resection - short bowel syndrome in 2 cases (4.5%), drugs such as furosemide in 3 cases (6%), amikacin in 3 cases (6%), amphotericin-B in 6 cases (12%), cyclosporine in 4 cases (9%), 6 cases (23%), renal losses; polyureic phase of acute tubular necrosis in 1 case (2%), chronic metabolic acidosis in 7 cases (15%), increased phosphate intake in 4 cases (9%), and blood transfusion in 4 cases (9%).
In terms of risk factors and risk distribution of cases that developed hypomagnesemia during hospitalization;
1. Drugs: Thiazide or loop diuretics (furosemide) were detected in 41 (25%) cases, aminoglycosides (amikacin) in 21 (13%) cases, amphotericin in 42 (25.6%) cases, cyclosporine in 11 (7%) cases, ethanol in 1 (0.6%) case, proton pump inhibitor in 3 (1.8%) cases, insulin in 5 (3%) cases.
2. Redistribution: Acute pancreatitis was detected in 1 (0.6%) case, DKA insulin treatment in 1 (0.6%) case, blood transfusion in 101 (62%) cases.
3. GIS causes: malnutrition was detected in 10 (6%) cases, intestinal resection short bowel syndrome in 5 (3%) cases, chronic diarrhea or long-term laxative use in 8 (5%) cases, long-term use of proton pump inhibitors in 8 (5%) cases, Nasogastric (NG) drainage in 29 (18%) cases.
4. Endocrine and metabolic disorders: hypercalcemia was detected in 2 (1.2%) cases, and increased phosphate intake in 39 (24%) cases.
5. Increase in extracellular volume was detected in 32 (20%) cases.
6. Renal losses: increased diuresis after renal obstruction was detected in 1 (0.6%) case, polyureic phase of acute tubular necrosis in 3 (1.8%) cases, renal tubular acidosis in 1 (0.6%) case, hyperkalemia in 3 (1.8%) cases, chronic metabolic acidosis in 9 (5.6%) cases.
7. Syndromes causing congenital magnesium loss: Gittelman syndrome was detected in 2 (1.2%) cases, and nephrocalcinosis associated with Mg loss was detected in 2 (1.2%) cases.
Evaluation of cases with and without hypomagnesemia at admission in terms of risk factors is shown in Table 2. Age, length of stay and electrolyte levels of patients who developed hypomagnesemia during their stay were compared. The length of stay in PICU was longer in patients with hypomagnesemia during their stay (17.3 ± 21.9 days) compared to patients without hypomagnesemia (10.7 ± 22.8 days) and this was found to be statistically significant (p=0.001). Serum albumin (2.9 ± 0.6 gr/dl), serum phosphorus (3.9 ± 1.3 mg/dl) and serum potassium (3.7 ± 0.8 mEq/L) were found to be lower in patients who developed hypomagnesemia during their stay in the pediatric intensive care unit and this was found to be statistically significant (p=0.001).
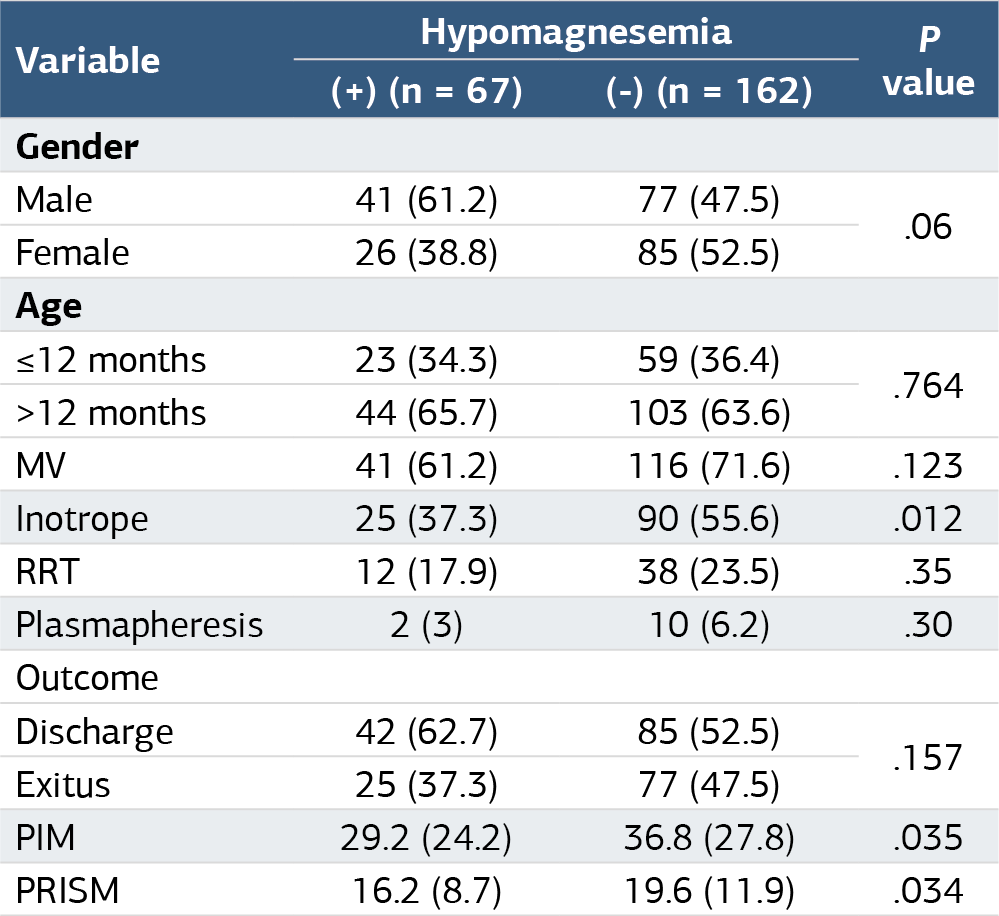
Evaluation of Demographic Characteristics in Cases with and without Hypomagnesemia During Hospitalization is shown in Table 3. In our study, there is a statistically significant relationship between hypomagnesemia and hypoalbuminemia, hypophosphatemia and hypopotassemia in terms of electrolytes in cases with and without hypomagnesemia during hospitalization (p=0.001). Of the cases that developed hypomagnesemia during hospitalization, 81.5% had hypoalbuminemia, 35.2% had hypokalemia, 30.9% had hypophosphatemia, 30.2% had hyponatremia and 6.8% had hypocalcemia.
When we compared the time of hypomagnesemia development and the duration of hospitalization in the group that developed hypomagnesemia during hospitalization, it was found to be 9.33 ± 8.47 days in those who developed hypomagnesemia in the first 5 days of hospitalization, 25.64 ± 27.76 days in those who developed hypomagnesemia after the 5th day. The duration of hospitalization was found to be longer in cases that developed hypomagnesemia after the 5th day and was statistically significant (p=0.001).
When we examined the distribution of serum Mg values of the cases according to primary disease etiologies, low Mg was found to be higher in renal and malignancy/solid tumor patients compared to the normal Mg group. The duration of hospitalization in the PICU was 14.1 ± 20.2 days in those with hypomagnesemia at admission, 17.3 ± 21.9 days in those who developed hypomagnesemia during admission, and 10.7 ± 22.8 days in the group with normal Mg. The duration of hospitalization was found to be shorter in the group with normal Mg compared to the other two groups.
Discussion
In our study, the serum Mg concentration we measured to evaluate Mg status represents only 0.3% of the total body Mg content. Standard serum total Mg concentration measurements are between 1.7–2.3 mg/dl and these values include ionized, protein-bound and complex forms. In our study, similar to other studies, hypomagnesemia was detected as 70.7%. In studies conducted on critically ill patients, the prevalence of hypomagnesemia was found to be between 14–70%, and total serum Mg measurements were mostly performed in patients.7,8
Many studies have shown that hypomagnesemia occurring in patients under PICU care prolongs the length of stay in hospital and intensive care, makes weaning from mechanical ventilation (MV) difficult, and increases mortality and morbidity.8,9,10,11,12,13 Therefore, hypomagnesemia and associated risk factors should be carefully monitored in intensive care patients, and Mg replacement therapy should be started immediately in patients who develop hypomagnesemia.
In a retrospective study conducted by Saleem et al. on 179 cases in the PICU, the frequency of hypomagnesemia was found to be 44.1%, 8.9% in the first 5 days and 34% in cases after the 5th day.14 Limaya et al. found hypomagnesemia in 52% of patients in a prospective study of 100 critical cases.15 Hypomagnesemia was detected in 61% of critically ill patients by Passakiotou et al., and hypomagnesemia was detected in 44–66% by Ribeiro et al., who measured total and erythrocyte Mg levels in 7000 critically ill patients.16,17 In our study, similar to other studies, hypomagnesemia was detected in 70.7%. In our study, MV connection was found to be 71.6% (116/162) in hypomagnesemia patients and 61.2% (41/67) in normomagnesemia patients. Although it was found to be high, it was not found to be statistically significant (p>0.05). In the study by Limaye et al., MV support was provided to 73% (38/52) of patients who developed hypomagnesemia, while ventilation support was provided to only 53% (22/41) of the normomagnesemia group, and MV support was found to be statistically significant with low Mg (p<0.05). The mean duration of MV in patients with low serum Mg was 8 ± 7.92 days, while in patients with normal serum Mg it was 6.17 ± 3.84 days, the difference was not found to be statistically significant (p>0.05).15 In the study conducted by Laddhad et al. in 100 patients, it was found that hypomagnesemia was significantly correlated with increased ICU stay and mortality, but it did not affect the duration of mechanical ventilation.18 Hypomagnesemia causes muscle weakness and respiratory failure, which makes it difficult to separate the patient from MV. In other studies, and in our study, it has been observed that hypomagnesemia patients require more frequent and longer-term ventilation support.
In our study, mortality rates were found to be 45.5% (20/44) in those with hypomagnesemia at admission, 47.5% (77/162) in those who developed hypomagnesemia during admission, and 37.5% (25/67) in the normomagnesemia group, but this was not statistically significant (p>0.05). In a study of Malinowska et al., it was found that 1505 patients with hypomagnesemia had a higher mortality rate compared to those with normal magnesium levels (normomagnesemia). The study highlighted a significant association between low magnesium levels and increased mortality in critically ill patients.19 In a study of Makwana et al., a total of 323 patients were analyzed. It was found that the mortality rate was significantly higher in hypomagnesemic patients compared to normomagnesemic patients.20 In our study and other studies, the mortality rates of hypomagnesemia patients were found to be significantly higher. The higher mortality rates in hypomagnesemia patients may be explained by the higher frequency of sepsis, septic shock, and electrolyte abnormalities, especially hypokalemia and cardiac arrhythmias, which are common causes of death in the ICU, and their relationship with hypomagnesemia.
In our study, the length of stay in the hypomagnesemia group was 17.3 ± 21.9 days, and in the normomagnesemia group, it was 10.7 ± 22.8 days. The length of stay in the hypomagnesemia group was significantly longer and statistically significant (p=0.001). In a study by Maqbali et al., a total of 410 patients were analyzed. It was found that hypomagnesemia patients had a significantly longer ICU length of stay compared to normomagnesemia patients, highlighting the potential impact of low magnesium levels on prolonged recovery in critically ill individuals.21 In their study on 100 patients, Laddhad et al. found that hypomagnesemic patients had a significantly longer ICU length of stay compared to normomagnesemic patients.18
It is stated that there is a strong relationship between hypomagnesemia and insulin resistance and that Mg supplementation reduces insulin requirements.22,23 In addition, use of both loop diuretics and thiazides can inhibit net Mg reabsorption and induce hypomagnesemia, which may trigger insulin resistance.24 Studies have also reported a significant relationship between antibiotic use and the development of hypomagnesemia.24,25 In our study, the highest risk factors determined as 62% of patients developing hypomagnesemia were blood transfusion, 25% thiazide or loop diuretics (furosemide), 13% aminoglycosides (amikacin), 25.6% amphotericin-B, 24% increased phosphate intake, and 18% NG drainage.
Limitations
The retrospective single-center design and the use of medical record data may limit the generalizability of the findings.
Conclusion
In conclusion, in our study, the rate of mechanical ventilation (MV) connection was 71.6% (116/162) in hypomagnesemic patients and 61.2% (41/67) in normomagnesemic patients. Although the rate was higher in hypomagnesemic patients, it was not statistically significant (p>0.05). While the length of stay in hypomagnesemic patients (8 ± 7.92 days) was longer compared to normomagnesemic patients (6.17 ± 3.84 days), this difference was also not statistically significant. The frequency of low serum magnesium levels was found to be significantly higher in children hospitalized in the PICU. Hypomagnesemic children had longer hospital stays, higher mortality rates, and more frequent electrolyte disturbances. Magnesium levels should be monitored closely in the PICU. Prospective and larger studies are needed to further evaluate hypomagnesemia and its associated factors in the PICU.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived because this retrospective study used anonymized patient data.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ICU: Intensive care unit
Mg: Magnesium
MV: Mechanical ventilation
PICU: Pediatric intensive care unit
References
-
Petho AG, Fulop T, Orosz P, Tapolyai M. Magnesium is a vital ion in the body: it is time to consider its supplementation on a routine basis. Clin Pract. 2024;14(2):521-535.
-
Alexander RT, Dimke H. Molecular mechanisms underlying paracellular calcium and magnesium reabsorption in the proximal tubule and thick ascending limb. Ann N Y Acad Sci. 2022;1518(1):69-83. doi:10.1111/nyas.14909
-
Piuri G, Zocchi M, Della Porta M, et al. Magnesium in obesity, metabolic syndrome, and type 2 diabetes. Nutrients. 2021;13(2):1-7. doi:10.3390/nu13020320
-
Rigo J, Pieltain C, Christmann V, et al. Serum magnesium levels in preterm infants are higher than adult levels: a systematic literature review and meta-analysis. Nutrients. 2017;9(10):1-10. doi:10.3390/nu9101125
-
Dokuyucu R, Gogebakan B, Yumrutas O, et al. Expressions of TRPM6 and TRPM7 and histopathological evaluation of tissues in ischemia reperfusion performed rats. Ren Fail. 2014;36(6):932-936. doi:10.3109/0886022x.2014.900405
-
Al Alawi AM, Majoni SW, Falhammar H. Magnesium and human health: perspectives and research directions. Int J Endocrinol. 2018;4(4):1-17. doi:10.1155/2018/9041694
-
Jiang P, Lv Q, Lai T, Xu F. Does hypomagnesemia impact on the outcome of patients admitted to the intensive care unit? A systematic review and meta-analysis. Shock. 2017;47(3):288-295. doi:10.1097/shk.0000000000000769
-
Solanki J, Runwal K, Beke N, Bahulikar A, Phalgune D. Serum magnesium levels in critically ill patients on admission in ICU and its correlation with outcome. J Assoc Physicians India. 2022;70(5):11-12.
-
Kim JY, Lee HJ, Lee HY, Lee SM, Lee J, Park TY. The effects of hypomagnesemia on delirium in middle-aged and older adult patients admitted to medical intensive care units. Acute Crit Care. 2022;37(3):407-414. doi:10.4266/acc.2022.00164
-
Dabla PK, Sharma S, Dabas A, et al. Ionized blood magnesium in sick children: an overlooked electrolyte. J Trop Pediatr. 2022;68(2):1-8. doi:10.1093/tropej/fmac022
-
Doyle KG, Blackstone MM, Barrett BC. Subacute gummy vitamin overdose as a rare manifestation of child neglect. Pediatr Emerg Care. 2021;37(8):479-482. doi:10.1097/pec.0000000000001718
-
Peres IT, Hamacher S, Oliveira FLC, Thome AMT, Bozza FA. What factors predict length of stay in the intensive care unit? Systematic review and meta-analysis. J Crit Care. 2020;60:183-194. doi:10.1016/j.jcrc.2020.08.003
-
Radu CP, Daniealopol V, Santini A, Darie R, Sala DT. Fatal hypocalcaemia due to hungry bone syndrome with secondary refractory hyperparathyroidism after parathyroidectomy: a case report. J Crit Care Med (Targu Mures). 2019;5(4):140-144. doi:10.2478/jccm-2019-0021
-
Haque A, Saleem AF. On-admission hypomagnesemia in critically ill children: risk factors and outcome. Indian J Pediatr. 2009;76(12):1227-1230. doi:10.1007/s12098-009-0258-z
-
Limaye CS, Londhey VA, Nadkart MY, Borges NE. Hypomagnesemia in critically ill medical patients. J Assoc Physicians India. 2011;59(1):19-22.
-
Passakiotou M, Lampiri C, Kopatzidis E, Sounidakis N, Asimaki M, Gritsi-Gerogianni N. Magnesium at admission: is it an outcome marker in the critically ill patient? Crit Care. 2005;9(1):416-423. doi:10.1186/cc3479
-
Ribeiro HS, Burdmann EA, Vieira EA, Ferreira ML, Ferreira AP, Inda-Filho AJ. Association of magnesium abnormalities at intensive care unit admission with kidney outcomes and mortality: a prospective cohort study. Clin Exp Nephrol. 2022;26(10):997-1004. doi:10.1007/s10157-022-02245-6
-
Laddhad DS, Hingane V, Patil TR, Laddhad DD, Laddhad AD, Laddhad SD. An assessment of serum magnesium levels in critically ill patients: a prospective observational study. Int J Crit Illn Inj Sci. 2023;13(3):111-117. doi:10.4103/ijciis.ijciis_11_23
-
Malinowska J, Małecka M, Ciepiela O. Variations in magnesium concentration are associated with increased mortality: study in an unselected population of hospitalized patients. Nutrients. 2020;12(6):1836-1843. doi:10.3390/nu12061836
-
Makwana S, Patel A, Sonagara M. Correlation between serum magnesium level and acute exacerbation in patients with chronic obstructive pulmonary disease. Cureus. 2022;1(1):1-9. doi:10.7759/cureus.26229
-
Al M, Al A, Abeyaratne, Majoni, Falhammar. Clinical outcomes in patients hospitalised with dysmagnesemia in the Northern Territory of Australia: a retrospective, longitudinal data-linkage study. Rural Remote Health. 2024;24(1):8515-8523.
-
Pitliya A, Vasudevan SS, Batra V, et al. Global prevalence of hypomagnesemia in type 2 diabetes mellitus: a comprehensive systematic review and meta-analysis of observational studies. Endocrine. 2023;84(3):842-851. doi:10.1007/s12020-023-03670-7
-
Drenthen LCA, de Baaij JHF, Rodwell L, van Herwaarden AE, Tack CJ, de Galan BE. Oral magnesium supplementation does not affect insulin sensitivity in people with insulin-treated type 2 diabetes and a low serum magnesium: a randomised controlled trial. Diabetologia. 2023;67(1):52-61
-
Lapointe A, Royer Moreau N, Simonyan D, et al. Identification of predictors of abnormal calcium, magnesium, and phosphorus blood levels in the emergency department: a retrospective cohort study. Open Access Emerg Med. 2021;13:13-21. doi:10.2147/oaem.s289748
-
Liamis G, Hoorn EJ, Florentin M, Milionis H. An overview of diagnosis and management of drug-induced hypomagnesemia. Pharmacol Res Perspect. 2021;9(4):829-835. doi:10.1002/prp2.829
Tables
Table 1. Demographic and clinical characteristics of the cases

Table 2. Evaluation of patients with hypomagnesemia at admission in terms of risk factors
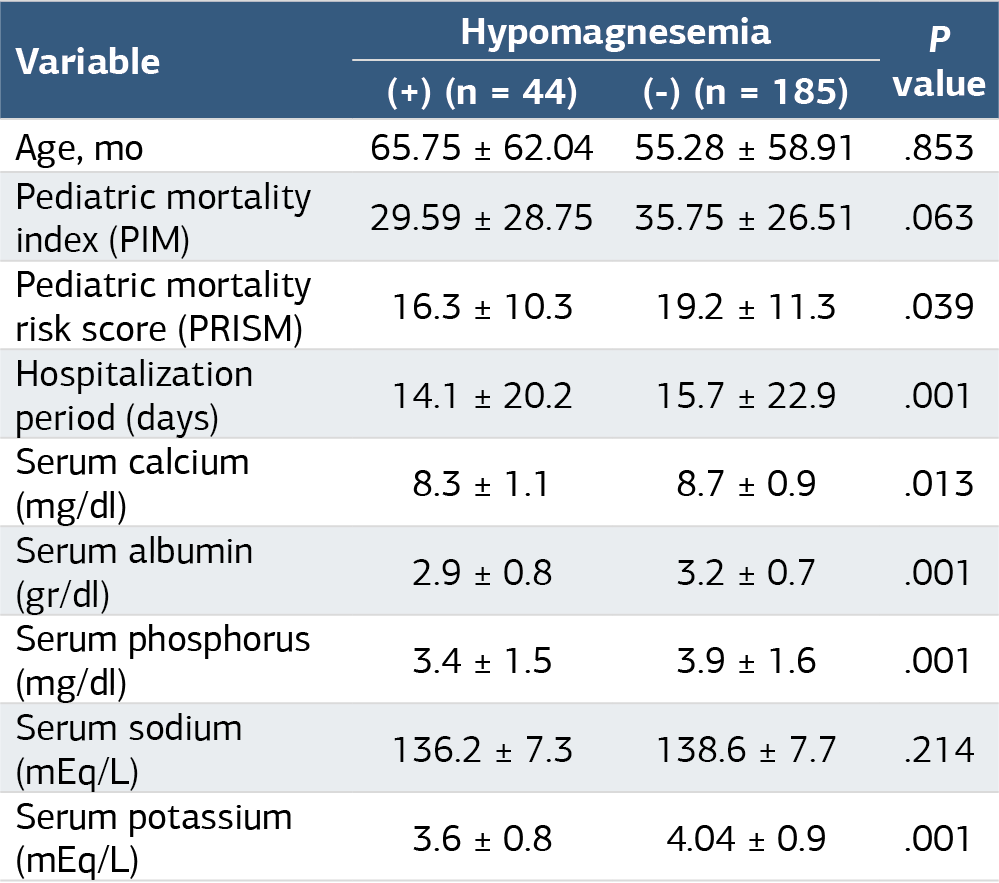
Table 3. Evaluation of demographic characteristics in patients with and without hypomagnesemia during hospitalization
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hasan Avşar, Metin Kılıç, Arzu Oto, Mehmet Boşnak. Hypomagnesemia in pediatric intensive care unit: etiology, risk factors and relationship of mortality. Ann Clin Anal Med 2025;16(5):336-340. doi:10.4328/ACAM.22398
- Received:
- September 10, 2024
- Accepted:
- October 21, 2024
- Published Online:
- December 10, 2024
- Printed:
- May 1, 2025