
Relationship between platelet mass index and coronary slow flow phenomenon
Coronary slow flow and platelet mass index
Authors
Abstract
AimCoronary slow flow (CSF) is an important clinical entity that may cause anginal symptomatology, acute coronary syndrome or even sudden cardiac death. Its pathogenesis is complex, and previously, several hematological parameters were shown to be independently associated with CSF. Platelet mass index (PMI) is a novel platelet index showing bodily inflammation and thrombogenesis status. Our aim was to assess the relationship between PMI and CSF in anginal patients undergoing coronary angiography.
MethodsOur study is retrospective and a total of 92 patients with CSF and 100 age- and sex-matched subjects with normal coronary flow were included between June 2020 and October 2023. Data regarding demographic, clinical and angiographic characteristics were retrieved from digital hospital database. TIMI frame count (TFC) were calculated by two independent cardiologists blinded to the study protocol. PMI was calculated as platelet count multiplied by mean platelet volume (MPV).
ResultsMean TFC was (43.93 ± 9.56 vs 20.0 ± 4.1, respectively, p<0.001). Respective MPV and PMI of CSF and control groups were 8.64±0.88 fL vs 8.64±0.88 fL (p<0.001) and 2983.5 (2692.5-3217.2) vs 2261.5 (2100-2456) (p<0.001). PMI (rho=0.578, p<0.001) and MPV (rho=0.395, p<0.001) were correlated with CSF. In regression analysis, MPV and PMI were independently associated with CSF. In ROC analysis, MPV cut-off was 80.5 fL with 70% sensitivity and 68% specificity (AUC: 0.755), and PMI cut-off was 2564 with 80% sensitivity and 82% specificity (AUC: 0.866).
ConclusionPMI and MPV are increased in CSF, and PMI and MPV are independently associated with CSFP.
Keywords
Introduction
Coronary slow flow phenomenon (CSFP) is characterized by the delayed transmission of contrast dye to the distal part of the coronary arteries without overt stenosis. While its incidence is reported to be between 1% and 7% of all the coronary angiography procedures,1 the exact mechanism by which CSFP occurs is yet to be totally resolved. However, several mechanisms have been put forth as the etiology such as increased microvascular tonus, microvascular inflammation1,2 and endothelial dysfunction.3 It is well known that CSFP is associated with angina pectoris, cardiac arrhythmias, acute coronary syndromes and even sudden cardiac death.1
Previous studies have shown that platelet indices, such as platelet count, platelet distribution width and mean platelet volume (MPV), are likely to be related with acute coronary syndrome (ACS) and coronary artery disease (CAD) progression.4,5 Despite a greater number of studies regarding the association of MPV and CSFP,6,7 there are some other studies oppose this association, too.8,9,10 In most of the studies, there have been no significant difference with regard to mean platelet counts between the CSFP and control groups, although some reported greater platelet counts in CSFP groups. Platelet mass index has been proposed as a relatively new platelet and inflammation index, which is calculated by multiplying the MPV with platelet count. As a novel index of both platelet activity and inflammation, PMI has been proposed to have a superior predicting ability compared to lone MPV or platelet count.11,12 However, studies on the association of PMI with CAD are scanty. It was reported in a previous study that an increased PMI in psoriasis might be a relevant factor of coronary plaque formation due to close interplay between CAD formation and psoriasis.13 The preliminary studies regarding PMI were on platelet transfusion in preterm newborns in neonatal intensive care units.14,15 There has been a fine balance between MPV and platelet count, where a decreasing platelet counts due to various reasons, for example inflammation, intravascular coagulation or platelet alloimmunization, cause an increase in MPV due to newly-formed younger platelets characterized with greater megakaryocyte cytoplasm. There is, on the other hand, no study investigating the relationship between PMI and CSFP. In the present study, the relationship of PMI with CSFP was investigated, and our hypothesis was that increased PMI would be observed in patients with CSFP.
Materials and Methods
Study Designation and Patient EnrollmentThis is a cross-sectional and retrospective study. Coronary angiographic data of 158 patients with CSFP were analyzed retrospectively between June 2020 and October 2023 and, after excluding 66 patients based on our exclusion criteria, a final 92 subjects having CSFP in at least one epicardial coronary artery without a prominent stenosis were included in the study as the CSPF group. Furthermore, 100 subjects with angiographically-depicted normal coronary arteries without any CSFP were selected as controls. All subjects of the study cohort underwent coronary angiography due to anginal chest pain, along with ischemic findings in non-invasive stress tests. The clinical and demographic features of the subjects were retrieved from the hospital digital database. The exclusion criteria included: a history of acute coronary syndrome; history of rheumatic, hematological, or oncological disease; moderate-to-severe valvular heart disease; chronic inflammation; severe hepatic or kidney disease; and presence of dilated or hypertrophic cardiomyopathy.
Echocardiographic evaluation via Vivid S5 (GE Vingmed Ultrasound AS, Horten, Norway) was implemented in all the study subjects and modified Simpson’s rule was utilized in the calculation of left ventricular ejection fraction (LVEF). The body-mass index (BMI) was computed as subject’s weight divided by the square of his/her height. A BMI >30 kg/m2 was accepted as obesity. Patients with a mean of repeated office blood pressure >140/90 mmHg or on anti-hypertensive therapy were considered to have hypertension. Diabetes mellitus was defined by a fasting blood glucose >126 mg/dL, HgA1c>6.5 or the use of antidiabetic drugs. Hyperlipidemia was defined as: triglycerides >150 mg/dL, low density lipoprotein (LDL) >130 mg/dL, or total cholesterol >200 mg/dL.
Coronary Angiographic ProceduresCoronary angiography was performed using Judkins technique in each subject with Artis Zee (Siemens Medical, Erlangen, Germany) via femoral or radial access. Angiographic views were recorded at 15 frames per second and two consultant cardiologists blinded to the study data assessed the angiographic views in Axiom workstation (Siemens Medical, Erlangen, Germany). The diagnosis of CSFP was confirmed using the TIMI frame count (TFC) method. Briefly, the number of total cine-frames for contrast agent to reach the distal part of the left anterior descending artery (LAD), right coronary artery (RCA) and the left circumflex artery (Cx) was determined with the help of frame counter. The distal part of the each major epicardial artery was defined as follows: LAD: distal bifurcation; Cx: artery’s distal bifurcation or obtuse marginal artery’s distal bifurcation on the basis of their length and, RCA: first branch of posterolateral artery.16,17,18,19 As the course of LAD is longer than both Cx and RCA, a correction was applied using the formula LAD TFC/1.7 to obtain an ultimate corrected LAD TFC (cTFC).16 Gibson et al.16 described the TFC normal values as 21.1±1.5 for LAD; 22.2±4.1 for Cx; and, 20.4±3.0 for RCA. The sum of the each TFM for LAD, Cx and RCA was divided by three to end up with the mean TFC. Moreover, we multiplied the TFCs that we counted by two, because the standardized recording rate for the given normal values was 30 frames per second.16 TFC calculations were performed by 2 consultant cardiologists and if a disagreement occurs between these two cardiologists, a third cardiologist blinded to the study data resolved this conflict. Subjects with greater TFC than the normal values were regarded as having CSFP.
Biochemical and Hematological ParametersThe blood samples were collected from each subject via a venous route before angiography and were analyzed in 10-15 minutes after sampling. An automated analyzer (Roche Hitachi Cobas c8000 autoanalyzer, Roche Diagnostic Corp., Mannheim, Germany) was used to measure serum biochemistry. Moreover, a Beckman Coulter (Miami, FL, USA) was utilized for complete blood count. PMI was computed as platelet count multiplied by MPV.
Ethical ApprovalThe study was approved by the Ethics Committee of Necmettin Erbakan University (Date: 15.12.2023, Decision No: 118).
Statistical AnalysisThe normality of the distribution of the parameters was assessed using the Kolmogorov-Smirnov test. Variables with a normal distribution were expressed as mean ± standard deviation. The variable that are not normally distributed were expressed as median (25th-75th percentiles). Categorical parameters were expressed as counts and percentages. The bivariate analysis of the study parameters was performed using the Chi Square test, Mann-Whitney-U test and independent t test where appropriate. Correlations between the variables were assessed using Pearson or Spearman correlation analysis, as appropriate. We performed a multinominal logistic regression analysis to define the parameters independently associated with CSFP. Finally, receiver operating characteristic (ROC) curve analysis was utilized in order to define the cot-off of PMI to predict CSFP. A p-value was accepted statistically significant when it is <0.05. All the calculations were implemented using the Statistical Package for Social Sciences (SPSS) for Windows, version 29.0 (SPSS Inc., Chicago, IL, USA).
Reporting GuidelinesThe study was reported in accordance with the STROBE guideline.
Results
The study included 92 patients with CSFP (mean age 58.4±9.2, 85.5% male) and 100 controls with normal epicardial blood flow (mean age 56.5±10.1; 86.6% male). Clinical and demographic features of two groups were presented in Table 1. There were no significant differences between the groups in terms of gender, age, systolic and diastolic pressures, pulse rate, HT, DM, dyslipidemia, smoking, LVEF, glucose, cholesterol levels, urea, creatinine, WBC, hemoglobin, platelet count, and platelet distribution width (p>0.05). However, patients with CSFP were more obese compared with the controls (25.6% vs 20%, respectively, p=0.035). Platecrit, MPV and PMI were significantly greater in the CSFP group as compared with the control group [for platecrit: 0.215±0.043% vs 0.201±0.025, respectively, p=0.022; for MPV: 8.64±0.88 fL vs 8.64±0.88 fL, respectively, p<0.001; for PMI: 2983.5 (2692.5-3217.2) vs 2261.5 (2100-2456), respectively, p<0.001].
As for the angiographic characteristics of the subjects. TFC in all major coronary arteries was higher in the CSFP groups compared with the controls (p<0.001 for all cLAD artery, LCx artery and RCA). Moreover, the mean TFC in CSFP was significantly greater than in the control group (43.93±9.56 vs 20.0±4.1, respectively, p<0.001) (Table 1).
Correlation analysis shows that TFC was significantly correlated with PMI (rho=0.578, p<0.001), MPV (rho=0.395, p<0.001) and platecrit (rho=0.188, p=0.016) (Table 2).
Table 3 demonstrates univariate and multivariate logistic regression analysis. Smoking,[OR: 1.51 (1.10-2.21), p=0.024] obesity,[OR: 1.04 (1.01-1.06), p=0.027] TFC,[OR: 6.361 (1.15-35.2), p=0.034] MPV [OR: 1.103 (1.026-1.215), p=0.013] and PMI [OR: 1.407 (1.04-2.015), p=0.026] were found to be independently associated with CSFP. In ROC curve analysis, MPV cut-off was 80.5 fL with 70% sensitivity and 68% specificity (AUC: 0.755) (Figure 1). PMI cut-off was 2564 with 80% sensitivity and 82% specificity (AUC: 0.866) (Figure 2). The AUC for PMI was greater than AUC for MPV.
Discussion
Our study investigated the relationship between PMI and CSFP, and demonstrated the following findings: 1- PMI and MPV were higher in the CSFP group than those of the controls; 2- PMI and MPV significantly correlated with TFC; 3- PMI and MPV were independently associated with CSFP; 4- PMI better predicted CSFP compared with MPV due to its greater AUC. To our knowledge, our study is the first to evaluate the relationship of PMI with CSFP.
The exact principle underlying mechanism of CSFP has still been yet to be totally elucidated. But, a number of hypotheses have been introduced regarding the topic, including endothelial damage caused by high asymmetric dimethyl arginine and decreased nitric oxide level in plasma.20,21 Pakdemir et al.3 demonstrated a diffuse atherosclerotic state in the coronary vasculature with the help of fractional flow reserve. Mangiery et al.22 on the other hand, performed histopathological examinations on cardiac biopsies and showed traces of microvascular resistance to blood circulation such as fibromuscular hyperplasia, neointimal proliferation, and vessel wall thickening in CSFP patients.
Platelets exert a significant influence over thrombosis and inflammation, and also pathophysiology of various cardiovascular diseases (CVDs) such as stroke, acute coronary syndrome carotid artery disease, pulmonary embolism, CAD.8,23 Among the platelet indices which shows the platelet activation is MPV. Larger platelets are more active due to increased number of granules containing prothrombotic and adhesion molecules. MPV represents a critical factor in the emergence of CVDs including CSFP.6,7 However, findings of some other studies stand against this association. Kaya et al.8 performed a study on 76 patients with CSFP and 389 controls and found no independent association of MPV with CSFP. Nurkelam et al. reported that MPV had not been associated with CSFP patients presenting with stable angina pectoris; however, MPS had been associated with CSFP patients presenting with unstabil angina pectoris. Most of the previous studies assessed the MPV and platelet count in the context of hematological indices, and ignored the platelet mass as calculated by the platelet count X MPV. In only one study, Akpınar et al.23 demonstrated that platecrit, a surrogate marker of platelet mass, is independently associated with CSFP. PMI is another novel parameter representing another surrogate marker of platelet mass. In our current investigation, PMI was also revealed to be significantly associated with CSFP.
Studies on PMI is sparce. Preliminary studies regarding PMI were mainly conducted over the need of platelet transfusion in pediatric patients in neonatal intensive care unit.14,15 There seems to be a balance in the PMI, since megakaryocytes expedite platelet production on the expense of larger cytoplasm upon decrease in platelet number for various reasons such as inflammation, intravascular coagulation or platelet alloimmunization, thereby increasing the MPV.14 In most of the studies regarding the hematological parameters in CSFP reported no association between platelet count and CSFP, and mean platelet numbers are similar between CSFP and the controls.7,8 Due to discrepancies in previous studies, sole platelet count or MPV would seem to be a poor clinical predictor of CSFP; and therefore, it would be prudent to hypotheses that PMI as addressed by platelet count X MPV might be more predictive as compared with the platelet count or MPV alone.
There is no clear-cut reference range for PMI. However, it seems that greater PMI is likely to be more predictor. In this regard, Demir et al.24 showed that PMI could be a more useful predictor of patent ductus arteriosus closure in preterm neonates compared with the platelet count alone. Günday et al.12 demonstrated that PMI was a more valuable predictor than MPV alone in coronary bypass operations. Unal13 reported an increased PMI and MPV in his study encompassing psoriatic patients, and concluded that the increase in these parameters may put the psoriasis patients to a more vulnerable state as regards atherosclerotic plaque complications.
Limitations
Among the limitations of the current study are: First, our patient population is relatively small. For this reason, there is a need for future studies encompassing larger cohorts confirm our results. Secondly, we did not perform a prospective study where catheter sizes and amount and administration pressure of contrast dye would be more predictable.
Conclusion
It was demonstrated in the present study that PMI and MPV are increased in patients with CSFP, and PMI and MPV are positively correlated with TFC. Moreover, PMI and MPV are independently associated with CSFP. Further studies are needed to validate our results.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ACS: Acute coronary syndrome
BMI: Body mass index
CAD: Coronary artery disease
CSF: Coronary slow flow
CSFP: Coronary slow flow phenomenon
Cx: Circumflex artery
DM: Diabetes mellitus
HDL: High-density lipoprotein
LAD: Left anterior descending artery
LDL: Low-density lipoprotein
LVEF: Left ventricular ejection fraction
MPV: Mean platelet volume
PDW: Platelet distribution width
PMI: Platelet mass index
RCA: Right coronary artery
ROC: Receiver operating characteristic
SPSS: Statistical Package for the Social Sciences
TFC: TIMI frame count
TIMI: Thrombolysis in Myocardial Infarction
WBC: White blood cell count
References
-
Aparicio A, Cuevas J, Morís C, Martín M. Slow coronary blood flow: pathogenesis and clinical implications. Eur Cardiol. 2022;17. doi:10.15420/ecr.2021.46
-
Altas Y, Kurtoglu E, Yaylak B, et al. The relationship between eosinophilia and slow coronary flow. Ther Clin Risk Manag. 2015;11:1187-1191.
-
Pekdemir H, Cin VG, Ciçek D, et al. Slow coronary flow may be a sign of diffuse atherosclerosis: contribution of FFR and IVUS. Acta Cardiol. 2004;59(2):127-133. doi:10.2143/ac.59.2.2005166
-
Uysal HB, Dağlı B, Akgüllü C, et al. Blood count parameters can predict the severity of coronary artery disease. Korean J Intern Med. 2016;31(6):1093-1100. doi:10.3904/kjim.2015.199
-
Wang H, Li H, Wang Y, et al. Hematological parameters and early-onset coronary artery disease: a retrospective case-control study based on 3366 participants. Ther Adv Chronic Dis. 2023;14:20406223221142670. doi:10.1177/20406223221142670
-
Demir M, Coşar S, Melek M. Evaluation of plasma eosinophil count and mean platelet volume in patients with coronary slow flow. Clinics (Sao Paulo). 2014;69(5):323-326. doi:10.6061/clinics/2014(05)05
-
Yılmaz M, Dağlı MN, Uku Ö, et al. Focusing on a complete blood cell parameter: mean platelet volume levels may be a predictor of coronary slow flow. Vasc Health Risk Manag. 2017;13:255-261. doi:10.2147/vhrm.s126105
-
Kaya Z, Günebakmaz Ö, Yıldız A, et al. Mean platelet volume is not associated with coronary slow flow: a retrospective cohort study. Anatol J Cardiol. 2015;15(1):18-24. doi:10.5152/akd.2014.5142
-
Seyyed-Mohammadzad MH, Khademvatani K, Kerachian A, Eskandari R, Rezaei Y. Slow coronary flow phenomenon and increased platelet volume indices. Korean Circ J. 2014;44(6):400-405. doi:10.4070/kcj.2014.44.6.400
-
Nurkalem Z, Alper AT, Orhan AL, et al. Mean platelet volume in patients with slow coronary flow and its relationship with clinical presentation. Turk Kardiyol Dern Ars. 2008;36(6):363-367.
-
Günday M, Çiftçi Ö. Comparison of platelet mass index in on-pump and off-pump coronary artery bypass surgery. Heart Surg Forum. 2020;23(2):154-159. doi:10.1532/hsf.2803
-
Korkmaz L, Baştuğ O, Ozdemir A, et al. The efficacy of propranolol in retinopathy of prematurity and its correlation with the platelet mass index. Curr Eye Res. 2017;42(1):88-97. doi:10.3109/02713683.2016.1158272
-
Unal M. Platelet mass index is increased in psoriasis: a possible link between psoriasis and atherosclerosis. Arch Med Sci Atheroscler Dis. 2016;1(1):145-149. doi:10.5114/amsad.2016.64444
-
Zisk JL, Mackley A, Clearly G, Chang E, Christensen RD, Paul DA. Transfusing neonates based on platelet count vs platelet mass: a randomized feasibility-pilot study. Platelets. 2014;25(7):513-516. doi:10.3109/09537104.2013.843072
-
Kahvecioglu D, Erdeve O, Alan S, et al. The impact of evaluating platelet transfusion need by platelet mass index on reducing the unnecessary transfusions in newborns. J Matern Fetal Neonatal Med. 2014;27(17):1787-1789. doi:10.3109/14767058.2013.879708
-
Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93(5):879-888. doi:10.1161/01.cir.93.5.879
-
Suner A, Cetin M. The effect of trimetazidine on ventricular repolarization indexes and left ventricular diastolic function in patients with coronary slow flow. Coron Artery Dis. 2016;27(5):398-404. doi:10.1097/mca.0000000000000373
-
Sanghvi S, Mathur R, Baroopal A, Kumar A. Clinical, demographic, risk factor and angiographic profile of coronary slow flow phenomenon: a single centre experience. Indian Heart J. 2018;70(suppl 3). doi:10.1016/j.ihj.2018.06.001
-
Sucu M, Ucaman B, Ozer O, Altas Y, Polat E. Novel ventricular repolarization indices in patients with coronary slow flow. J Atr Fibrillation. 2016;9(3):1446. doi:10.4022/jafib.1446
-
Selcuk MT, Selcuk H, Temizhan A, et al. Asymmetric dimethylarginine plasma concentrations and L-arginine/asymmetric dimethylarginine ratio in patients with slow coronary flow. Coron Artery Dis. 2007;18(7):545-551. doi:10.1097/mca.0b013e3282eff1c6
-
Sezgin N, Barutcu I, Sezgin AT, et al. Plasma nitric oxide level and its role in slow coronary flow phenomenon. Int Heart J. 2005;46(3):373-382. doi:10.1536/ihj.46.373
-
Mangieri E, Macchiarelli G, Ciavolella M, et al. Slow coronary flow: clinical and histopathological features in patients with otherwise normal epicardial coronary arteries. Cathet Cardiovasc Diagn. 1996;37(4):375-381.
-
Akpinar I, Sayin MR, Gursoy YC, et al. Plateletcrit and red cell distribution width are independent predictors of the slow coronary flow phenomenon. J Cardiol. 2014;63(2):112-118. doi:10.1016/j.jjcc.2013.07.010
-
Demir N, Peker E, Ece İ, Ağengin K, Bulan KA, Tuncer O. Is platelet mass a more significant indicator than platelet count of closure of patent ductus arteriosus? J Matern Fetal Neonatal Med. 2016;29(12):1915-1918. doi:10.3109/14767058.2015.1067296
Figures

Figure 1. ROC curve analysis of mean platelet volume to predict coronary slow flow

Figure 2. ROC curve analysis of platelet mass index to predict coronary slow flow
Tables
Table 1. Demographic, clinical and laboratory characteristics of the study groups
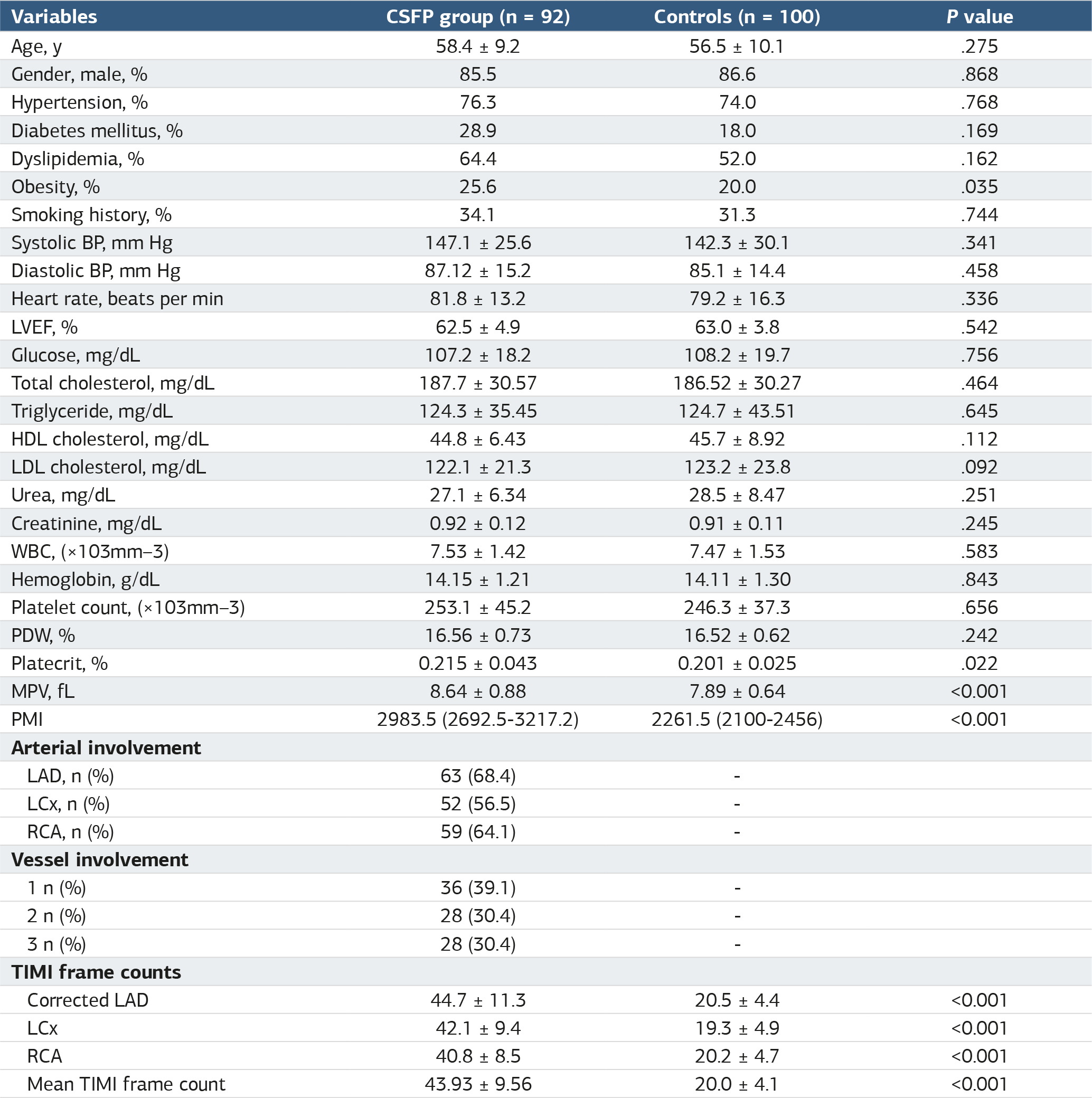
BP, blood pressure; LVEF, left ventricular ejection fraction; HDL, high-density lipoprotein; LDL, low-density lipoprotein; WBC, white blood cell count; PDW, platelet distribution width; MPV, mean platelet volume; PMI, platelet mass index.
Table 2. Correlation analysis of TIMI frame count with other variables

** Correlation is significant at the 0.01 level. * Correlation is significant at the 0.05 level.
Table 3. Multivariate logistic regression analysis to predict CSFP

TFC, TIMI frame count; MPV, mean platelet volume; PMI, platelet mass index.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Erdoğan Sökmen, Muhammet Salih Ateş. Relationship between platelet mass index and coronary slow flow phenomenon. Ann Clin Anal Med 2024;16(4):286-291. doi:10.4328/ACAM.22423
- Received:
- October 2, 2024
- Accepted:
- November 11, 2024
- Published Online:
- November 18, 2024
- Printed:
- April 1, 2024