
In-depth evaluation of violence against women
Violence against women
Authors
Abstract
AimViolence against women is a leading public health issue that poses a threat to every woman’s life. It has a negative physical, psychological, social, cultural, and economic impact on women. The study aimed to examine the nature, location, level of injury, and treatment needs of women who were victims of domestic violence, as well as their previous psychiatric admissions and diagnoses.
MethodsThis quantitative study retrospectively reviewed the records of 203 women who were presented to the emergency department for cases of domestic violence. This study examined the forms of domestic violence, forensic records, and medical history of these women.
ResultsThe mean age of the women was 32.62 ± 11.62 (16–75) years. It was found that 72.4% of them were married, and 8.37% (n = 17) were exposed to violence during pregnancy. Moreover, 93.6% of these victims were exposed to physical violence, and 90.6% had blunt injuries. Most injuries (65.1%) were observed in the head area. Bone fractures were found in 4.9% (n = 10) of the cases, of which 60% were nasal fractures. Although 195 women were treated as outpatients, six required hospitalization, and two women died.
ConclusionBecause emergency services are often the first point of contact for women who have been victims of violence, emergency medicine physicians must be able to suspect and diagnose all types of assault. They are usually present more frequently than other healthcare personnel, especially in busy emergency departments.
Keywords
Introduction
Violence against women is a leading public health problem and poses a threat and danger to women’s lives.1 The World Health Organization (WHO) defines violence as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, which either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation”. Violence affects women negatively in a multifaceted way: physically, psychologically, socially, culturally, and economically.2
Yam stated that 42% of the women killed for any reason were killed by their spouses or people living with them.3 In a study conducted by the Turkish Prime Ministry General Directorate on the Status of Women in 2009 with a total of 24,048 households across Turkey, it was stated that 39% of women experienced physical violence, 15% experienced sexual violence, and 44% experienced emotional violence at some point in their lives. The impact of domestic violence on women makes it a critical health issue that requires identification and intervention. It’s important to recognize that without action, violence against women can result in loss of life. Violence against women is a preventable health problem. The health sector, particularly emergency department professionals, plays a crucial role as the first point of contact for women who are victims of violence. After family and friends, as well as the police, emergency departments are the most utilized point of contact for women who experience violence.4,5 Two previous studies stated that women who were subjected to domestic violence applied to emergency departments three times more commonly compared to other women.6,7 Two different studies found that women who were subjected to domestic violence used healthcare services more commonly for a variety of reasons. However, women are unable to express their problems due to various reasons, such as shame from medical personnel, fear of their assailant, and guilt.8,9
In this study, we retrospectively examined the forensic reports and medical histories of women who sought a judicial report at the emergency department due to domestic violence. We looked at the demographic data of the women, the type of violence they experienced, requested medical examinations, treatments received, injury scores, need for consultation, number of visits to the psychiatric outpatient clinic, diagnoses received, hospitalization status, and the time between psychiatric admission and marriage date.
Materials and Methods
This retrospective study was carried out by examining the files of 203 female cases who applied to Ahi Evran University Faculty of Medicine Training and Research Hospital Emergency Department between 01 July 2018 and 31 December 2019 due to domestic violence. This hospital is the sole tertiary care facility offering psychiatric outpatient services to a population of 400.000.
Identity and demographic data of the cases were obtained from standard forms of domestic violence issued by the Health Directorate. In addition, data about the educational status, marital status, type of domestic violence, and type of injury of the cases were also obtained from these forms. The type of violence, injury type and region, imaging methods performed, the treatment method, the need for consultation, and data on outcome were obtained from the forensic reports issued for the cases. In addition, information about the number of admissions to the psychiatric outpatient clinic in the last ten years, the time of application, the diagnoses received, and hospitalization status in the psychiatric clinic were obtained from the hospital automation system. Missing data were collected by talking with some of the patients via telephone.
Women who arrived at the emergency department due to trauma from falls, car accidents, or altercations with others were not included in the study. Twenty-seven cases were excluded due to missing data. The chi-square, Fisher-Freeman-Halton, and Fisher exact tests were used for univariate analysis of the variables.
Ethical ApprovalThis study was approved by the Ethics Committee of Ahi Evran University Faculty of Medicine (Date: 25.02.2020, Decision No: 2020-03/24).
Statistical AnalysisStatistical analysis was performed using Statistical Package for the Social Sciences for Windows (IBM SPSS version 25.0, Armonk, NY, USA) software. Categorical variables were expressed as number (n) and percentage (%). The chi-square, Fisher-Freeman-Halton, and Fisher exact tests were used for univariate analysis of the variables. A two-sided p value of <0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The mean age of women included in the study was 32.62 ± 11.62 years (range: 16-75). 35.5% of the cases were in the 20-30 age group. The least applications were made by those 70 years old and over. 31.5% of the cases were primary school graduates. 72.4% of the cases were married. 93.6% of the cases brought to the emergency room due to domestic violence were subjected to physical violence, 3.9% were subjected to verbal violence, and 2.5% were subjected to sexual violence (Table 1).
50.2% of the cases had previously applied to the emergency department due to domestic violence. 8.37% (n = 17) of the cases were subjected to violence during their pregnancy. While thirteen women were subjected to violence in the first trimester of pregnancy, two women were subjected to violence in the second trimester, and two women were subjected to violence in the third trimester. One of the women who was subjected to violence in the third trimester had a stillbirth within a week. In terms of injury types, the most common injuries were blunt injuries, with a rate of 90.6%. Bone fractures occurred in 4.9% of cases (n = 10), of which 60% were nasal bone fractures. The most commonly requested radiological imaging method was X-ray, with a rate of 51.2%. In 65.5% of cases (n = 132), injuries were left to secondary healing. The most common consultations requested were neurosurgery and ear, nose, and throat consultations (Table 1). While 195 cases were treated as outpatients in the emergency department and discharged, six cases were hospitalized, and two cases died from domestic violence. The injury score of 91.1% of cases was 1, while the injury score of 2 cases was 6. Emergency room doctors most issued conclusive forensic reports with a rate of 73.8% (Table 1).
In the present study, no statistical relationship was found between the type of injury and age, educational status, marital status, type of violence, and fracture status. However, there was a statistically significant difference between the type of injury and treatment needs (p=0.000). Most blunt injuries (38.0%) did not require treatment, and 56.5% were left to secondary healing. Primary repairs were performed in 47.4% of penetrating injuries. There was also a statistically significant difference between the type of injury and the outcome (p=0.010). While 96.7% of blunt injuries were treated as outpatients and discharged, this rate was 89.5% for penetrating injuries (p<0.010). No patients died from blunt injuries. However, 10.5% of the patients suffering from penetrating injuries died. There was also a statistically significant difference between the abbreviated injury scale and injury type (p=0.016). While 92.4% of blunt injuries were minor, this rate was only 78.9% for penetrating injuries (Table 2). On the other hand, no significant relationship was found when the same parameters concerning the type of violence (verbal, physical, sexual) were compared.
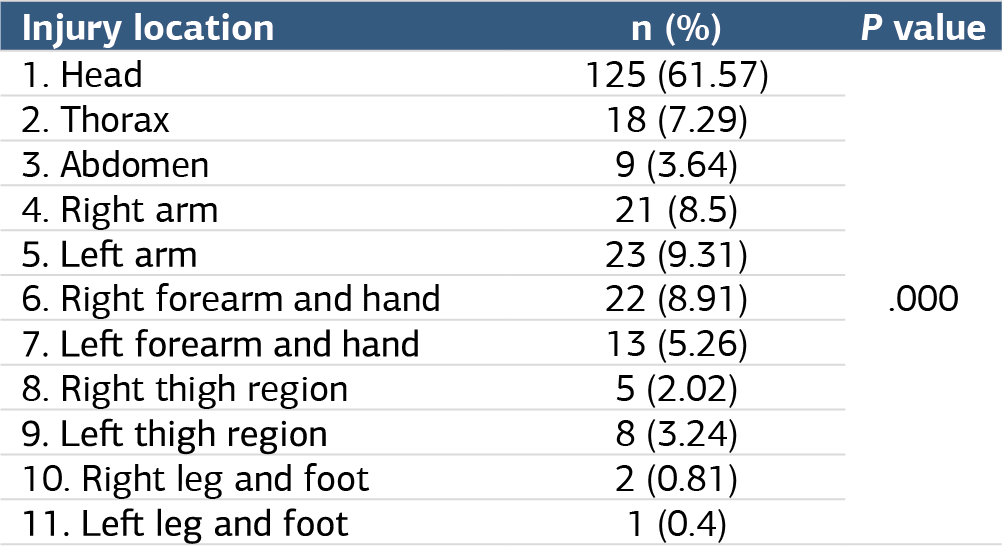
When the victims were examined in terms of the region of trauma on the body, it was found that 61.5% (n = 125) had trauma in the head region, followed by the upper extremities (38.9%). The least number of injuries were observed in the lower extremities (feet and ankles) (Figure 1). Significant results were obtained when the victims were examined in terms of the impact areas on the bodies (Table 3). Injuries resulting in death were caused by penetrating injuries to the thorax and abdomen. The present study divided the head into eight separate sections and evaluated. Lesions were observed in 22.4% of the cases on the scalp area, 20.8% of the cases on the neck area, 14.4% of the cases on the cheek and forehead area, 11.2% of the cases on the eye and supraorbital area, 11.2% of the cases on the lip and mouth area, 10.4% of the cases on the nose, 7.2% of the cases on the ear and 2.4% of the cases on the jaw area. Fractures were most commonly observed on the nasal bone, with a rate of 60% (Figure 1).
Since our hospital is the sole provider of psychiatric outpatient services for a population of 400.000, we were able to access ten years’ worth of psychiatric archives. In the present study, we investigated the admission rates of patients in the psychiatry outpatient clinic before and after their marriage. It was found that 16% of the women applied to the psychiatry outpatient clinic before their marriage, and the admission rate of patients after their marriage increased to 51.6%. Thus, it was determined that after their marriage, women applied to psychiatry outpatient clinics three times more often than those before marriage.
In our study, we found that the most common psychiatric diagnosis among women who visited the psychiatric outpatient clinic was anxiety and adjustment disorder, with a rate of 34.9% (n = 71). This was followed by depression, with a rate of 26.1% (n = 53); bipolar affective disorder, with a rate of 3.9% (n = 10); obsessive-compulsive disorder, with a rate of 0.5% (n = 4); and, lastly, schizophrenia, with a rate of 0.5% (n = 2). These diagnoses in the psychiatric outpatient clinic were found to be statistically significant (p=0.000). On the other hand, 47.3% (n = 96) of patients had no psychiatric diagnosis.
Discussion
Violence against women is increasing in Turkey and globally. According to a 2014 WHO report, one in three women has experienced physical or sexual violence from an intimate partner at least once in their lives.10 According to the Center for Disease Control estimates, domestic violence against women leads to many health problems (disabilities, sexually transmitted diseases, perinatal complications, HIV, depression, suicide, anxiety, drug-alcohol addiction, post-traumatic stress disorder) and the lack of an established and reliable support system for women who are victims of violence and inadequate legal regulations against violence results in an increase in violence against women. In two previous studies conducted in Turkey, the mean age of women who were victims of domestic violence was 34 and 35.7, and the age period where domestic violence was most common was 30-40.1,11 The mean age of the victims included in the present study is consistent with the literature (32.5); however, the age period where domestic violence was most common was found to be 21-30. Muelleman et al. stated that the mean age of women who suffered from intimate partner violence (IPV) was 29, but the mean age of women who applied to health institutions due to non-IPV causes (other traumas) was 32.12
In three separate studies conducted in Turkey, the marriage rates of women who were victims of violence were reported to be 91.2% in 2006, 85.6% in 2010, and 79.2% in 2020.1,11,13 In the present study, 72.4% of the victims were married. This rate is decreasing steadily as more women who suffer from domestic violence get separated from their partners. Almeida et al. stated that almost 50% of women were exposed to at least one form of violence during pregnancy.14 In three previous studies conducted in Turkey, the ratio of women who were exposed to violence during pregnancy was determined as 3.9%, 7.6%, and 9.7%, respectively.1,11,15 This ratio was 8.37% in the present study. These rates are lower in Turkey, most likely because verbal violence is not considered a type of violence and reported. In addition, Berhanine et al. reported that women who were subjected to violence during pregnancy gave birth to underweight babies or gave birth prematurely three times more commonly compared to those who were not subjected to violence.16
Consistent with many studies in the literature, women who were subjected to domestic violence were mainly primary school graduates.1,11,13 Canpolat et al. mentioned that 69.8% of the cases they evaluated had been subjected to domestic violence before.11 In the present study, 50.2% of the cases had been previously admitted to the emergency department due to domestic violence.
In the present study, the most common region of trauma was the head area, with a rate of 61.57%. Muelleman et al. also reported that women who were victims of violence were most commonly injured in the head area (76.37%). Muelleman et al. divided the head area into three regions and reported that the injuries were most commonly on the face area.12 In the present study, we divided the head area into eight regions to provide a more detailed evaluation. However, when the cases were evaluated by the categorization of Muelleman et al., the most common region of trauma was the face, followed by the scalp and neck area. Similarly, a meta-analysis conducted by Wu et al. also concluded that the most common region of trauma among women who were subjected to violence was the head.17
Wu et al. stated that Head Neck Facial (HNF) injuries or multiple injuries are important markers for IPV cases, whereas isolated thoracic, abdominal, and pelvic injuries are not specific to IPV. In the same study, it was stated that IPV should be considered in women with HNF injuries with no witnesses or if there are injuries anywhere else in the body. Two studies reported that cases that died due to IPV applied to trauma centers due to similar traumas before they died, which was described as a missed opportunity if no diagnosis had been made during these previous applications. In the present study, two women died due to IPV.12,17 One of these cases was a Turkish citizen, and the case had applied to the emergency department twice in the last year due to IPV. The other case was a 23-year-old woman of Afghan nationality who had just come to Turkey. Therefore, patient history could not be obtained.
Two previous studies in the literature reported that maxillofacial trauma was observed in about half of the women subjected to violence. Similarly, head trauma was the most common form of trauma in the present study, and 50% of the cases had maxillofacial trauma.18,19 Mulleman et al. reported that fascial region contusion was the most common type of injury in women subjected to violence.12 In the present study, the most common lesion observed in the cases was blunt trauma in the fascial region.
Although a significant number of domestic violence cases occur each year in Turkey, the rates of emergency room admissions and official registration of these cases are relatively low. Campbell et al. noted that women subjected to IPV used health services more commonly for headaches and other reasons compared to other women.17,20 The present study determined that these cases applied to the emergency department with various subjective complaints. Therefore, some cases of domestic violence can only be detected in the emergency room thanks to the attention of doctors and nurses. For this reason, emergency healthcare personnel must consider domestic violence in cases with lesions, especially in the head and facial areas.
Limitations
One of the primary limitations of our study is its retrospective nature and the fact that it was conducted at a single center. Consequently, the potential for bias cannot be discounted.
Conclusion
Violence against women is a degrading act that should be addressed at every level of the healthcare system. This study emphasizes the importance of identifying and finding solutions to this problem. Emergency departments are often the initial point of contact for women who experience violence, so it is crucial to ensure that these departments can diagnose violence and provide the necessary psychological support, counseling, guidance, and security for the victims.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
HNF: Head, neck, and facial
IPV: Intimate partner violence
SPSS: Statistical Package for the Social Sciences
WHO: World Health Organization
References
-
Ocal O, Ozdemir S, Demir H, Eroglu SE, Onur OE, Ozturk TC. Evaluation of domestic violence against women admitted to the emergency room. Turk J Emerg Med. 2013;13(3):133-137. doi:10.5505/1304.7361.2013.02360
-
Yaman Ş. Acil servis hemşirelerinin kadına yönelik aile içi şiddete ilişkin rol ve sorumlulukları [The role and responsibilities of emergency nurses regarding domestic violence against women]. Fırat Univ Sağlık Bilim Tıp Derg. 2012;26(1):49-54.
-
Yam M. Seen but not heard: battered women’s perceptions of the ED experience. J Emerg Nurs. 2000;26(5):464-470. doi:10.1067/men.2000.110432
-
Hoffman RM, Ryus C, Tiyyagura G, Jubanyik K. Intimate partner violence screening during COVID-19. PLoS One. 2023;18(4). doi:10.1371/journal.pone.0284194
-
Duchesne E, Nathoo A, Walker M, Bartels SA. Patient and provider emergency care experiences related to intimate partner violence: a systematic review of the existing evidence. Trauma Violence Abuse. 2023;24(5):2901-2921. doi:10.1177/15248380221118962
-
Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331-1336. doi:10.1016/s0140-6736(02)08336-8
-
Feder GS, Hutson M, Ramsay J, Taket AR. Women exposed to intimate partner violence: expectations and experiences when they encounter health care professionals; a meta-analysis of qualitative studies. Arch Intern Med. 2006;166(1):22-37. doi:10.1001/archinte.166.1.22
-
Coker AL, Bethea L, Smith PH, Fadden MK, Brandt HM. Missed opportunities: intimate partner violence in family practice settings. Prev Med. 2002;34(4):445-454. doi:10.1006/pmed.2001.1005
-
Kothari CL, Rhodes KV. Missed opportunities: emergency department visits by police-identified victims of intimate partner violence. Ann Emerg Med. 2006;47(2):190-199. doi:10.1016/j.annemergmed.2005.10.016
-
Butchart A, Mikton C, Dahlberg LL, Krug EG. Global status report on violence prevention 2014. Inj Prev. 2015;21(3):213. doi:10.1136/injuryprev-2015-041640
-
Canpolat Ö, Demir M. Acil servise kadına yönelik aile içi şiddet nedeniyle başvuran vakaların değerlendirilmesi [Evaluation of case applied to emergency department due to domestic violence against women]. Gazi Sağlık Bilim Derg. 2020;5(1):1-9. doi:10.30569/adiyamansaglik.622934
-
Muelleman RL, Lenaghan PA, Pakieser RA. Battered women: injury locations and types. Ann Emerg Med. 1996;28(5):486-492. doi:10.1016/s0196-0644(96)70110-5
-
Kocacik F, Dogan O. Domestic violence against women in Sivas, Turkey: survey study. Croat Med J. 2006;47(5):742-749.
-
Almeida FSJ, Coutinho EC, Duarte JC, et al. Domestic violence in pregnancy: prevalence and characteristics of the pregnant woman. J Clin Nurs. 2017;26(15-16):2417-2425. doi:10.1111/jocn.13756
-
Yanikkerem E, Karadaş G, Adigüzel B, Sevil U. Domestic violence during pregnancy in Turkey and responsibility of prenatal healthcare providers. Am J Perinatol. 2006;23(2):93-103. doi:10.1055/s-2006-931802
-
Berhanie E, Gebregziabher D, Berihu H, Gerezgiher A, Kidane G. Intimate partner violence during pregnancy and adverse birth outcomes: a case-control study. Reprod Health. 2019;16(1):22. doi:10.1186/s12978-019-0670-4
-
Wu V, Huff H, Bhandari M. Pattern of physical injury associated with intimate partner violence in women presenting to the emergency department: a systematic review and meta-analysis. Trauma Violence Abuse. 2010;11(2):71-82. doi:10.1177/1524838010367503
-
Saddki N, Suhaimi AA, Daud R. Maxillofacial injuries associated with intimate partner violence in women. BMC Public Health. 2010;10:268. doi:10.1186/1471-2458-10-268
-
Rezaee N, Mardani-Hamooleh M. A qualitative study of the health-related perceptions of married Iranian women who have experienced domestic violence. J Forensic Nurs. 2021;17(1):34-42. doi:10.1097/jfn.0000000000000314
-
Campbell J, Jones AS, Dienemann J, et al. Intimate partner violence and physical health consequences. Arch Intern Med. 2002;162(10):1157-1163. doi:10.1001/archinte.162.10.1157
Figures
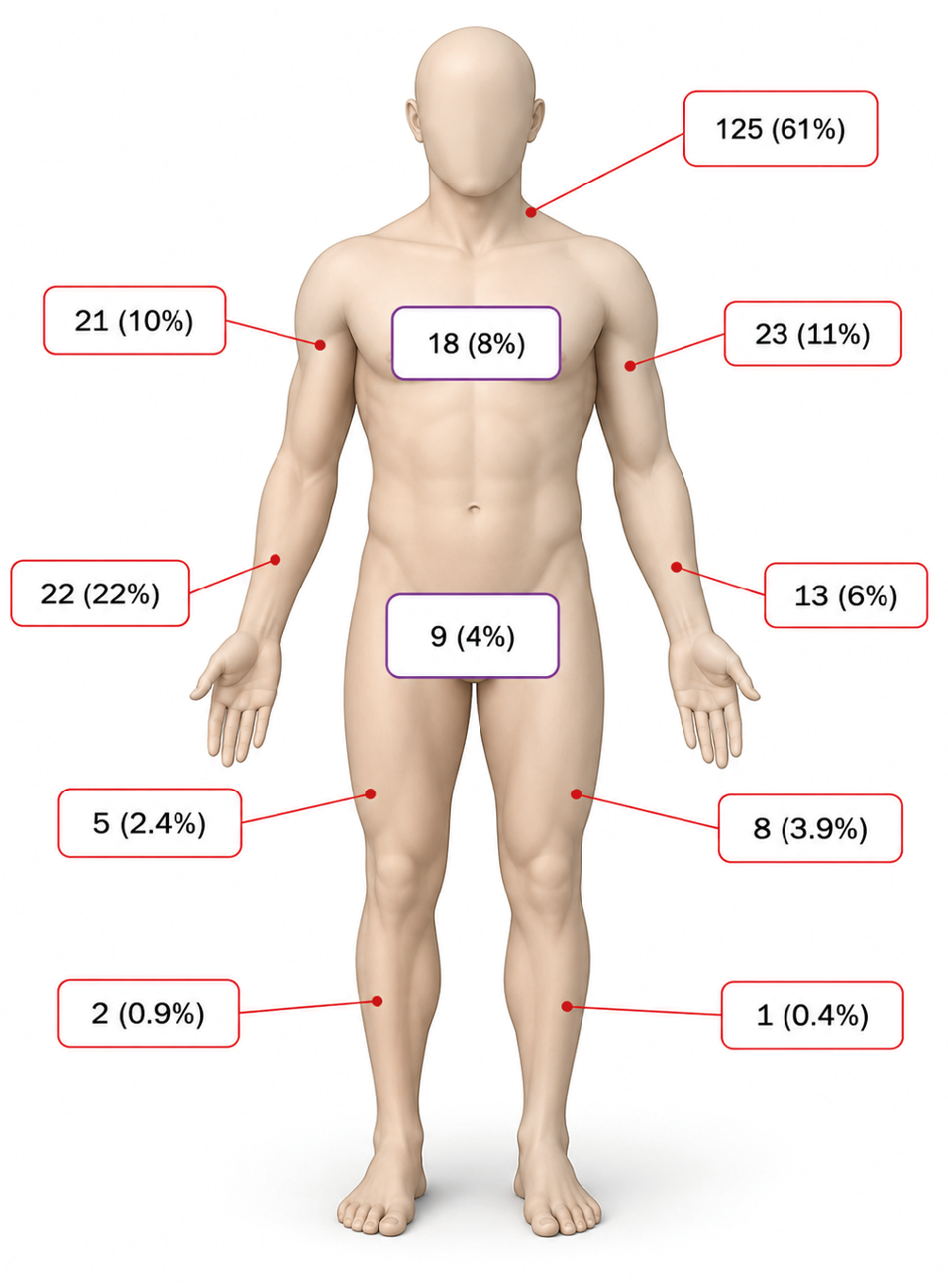
Figure 1. Injury locations
Tables
Table 1. Demographic and clinical characteristics of study population (n = 203)
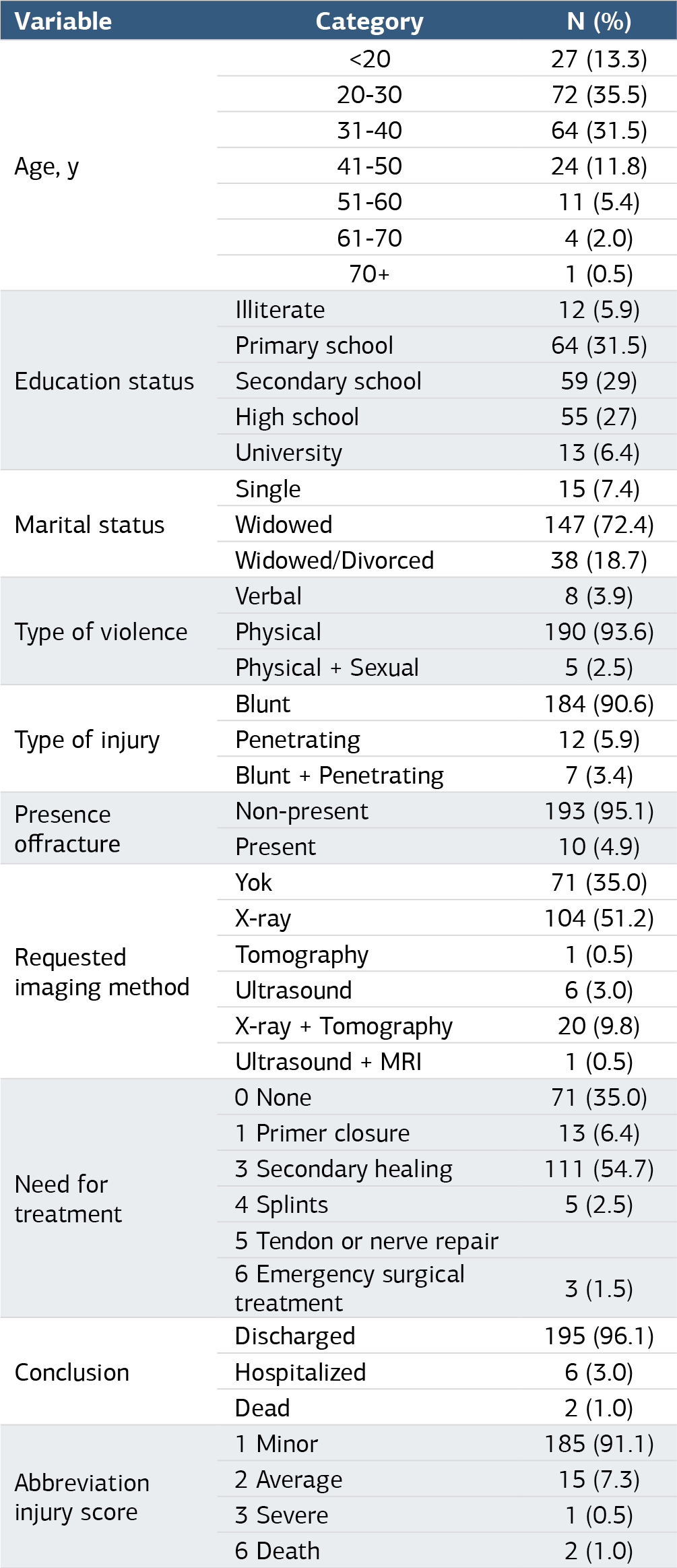
Table 2. Type of injury and demographic and clinic characteristics

Table 3. Injury location
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hacı Mehmet Çalışkan, Ömer Jaradat, Süleyman Ersoy, Şafak Taktak, Burak Çelik. In-depth evaluation of violence against women. Ann Clin Anal Med 2025;16(4):292-297. doi:10.4328/ACAM.22430
- Received:
- September 30, 2024
- Accepted:
- September 30, 2024
- Published Online:
- November 26, 2024
- Printed:
- April 1, 2025